Article Text

Abstract
Background Clinical decision rules (CDRs) are commonly used to guide imaging decisions in cervical spine injury (CSI) assessment despite limited evidence for their use in paediatric populations. We set out to determine CSI incidence, imaging rates and the frequency of previously identified CSI risk factors, and thus assess the projected impact on imaging rates if CDRs were strictly applied as a rule in our population.
Methods A single-centre prospective observational study on all aged under 16 years presenting for assessment of possible CSI to a tertiary paediatric emergency department over a year, commencing September 2015. CDR variables from the National Emergency X-Radiography Utilization Study (NEXUS) rule, Canadian C-Spine rule (CCR) and proposed Paediatric Emergency Care Applied Research Network (PECARN) rule were collected prospectively and applied post hoc.
Results 1010 children were enrolled; 973 had not received prior imaging. Of these, 40.7% received cervical spine imaging; 32.4% X-rays, 13.4% CT scan and 3% MRI. All three CDRs identified the five children (0.5%) with CSI who had not received prior imaging. If CDRs were strictly applied as a rule for imaging, projected imaging rates in our setting would be as follows: NEXUS-44% (95% CI 41% to 47.4%), CCR-at least 48.4% (95% CI 45.3% to 51.7%) and PECARN-68% (95% CI 65.1% to 71.1%).
Conclusion CSIs were rare (0.5% of our cohort), however, 40% of children received imaging. CDRs have been designed to guide imaging decisions; if strictly applied as a rule for imaging, the CDRs assessed in this study would increase imaging rates. Projected rates differ considerably depending on the CDR applied. These findings highlight the need for a validated paediatric-specific cervical spine imaging CDR.
- imaging
- CT/MRI
- imaging
- x-ray
- trauma
- spine and pelvis
- paediatrics
- paediatric injury
- paediatric emergency medicine
Data availability statement
Deidentified data are available on reasonable request and with appropriate permissions from regulatory authorities.
Statistics from Altmetric.com
- imaging
- CT/MRI
- imaging
- x-ray
- trauma
- spine and pelvis
- paediatrics
- paediatric injury
- paediatric emergency medicine
Key messages
What is already known on this subject
In adults, well-evidenced clinical decision rules (CDRs) such as NEXUS rule and Canadian C-Spine rule (CCR) rule can be used to guide the decision to image or not image for possible cervical spine injury (CSI).
In children, the validity of CDRs mainly derived in adults is limited and a paediatric risk tool for CSI from the Pediatric Emergency Care Applied Research Network (PECARN) is only in development.
The performance of these tools in children, including their potential impact on imaging rates, has not been adequately studied.
What this study adds
In a single-centre prospective cohort study of 973 children aged under 16 years with possible CSI, radiographically confirmed CSIs were rare (0.5%).
Use of NEXUS, CCR and PECARN tool to guide the decision to image or not image could increase the baseline imaging rate of 41% to between 44% and 68%.
Introduction
Paediatric cervical spine injury (CSI) is rare, occurring in an estimated 1%–2% of trauma presentations,1–4 but can have devastating consequences including death and long-term disability. Clinicians therefore seek to identify all CSIs, generally through the use of imaging modalities such as plain X-ray films (XR), computed tomography scans (CT) and magnetic resonance imaging (MRI).
Imaging carries risks including exposure to ionising radiation and increased lifetime cancer risk,5–8 and the need for sedation and its associated risks in some young or unco-operative children.9–11 Cervical spine immobilisation and imaging also has resource implications in terms of cost, staff time and prolonged bed occupancy in the emergency department (ED). Prolonged immobilisation can be distressing and may cause harm (skin pressure injuries, respiratory compromise).12 13 ED clinicians are thus faced with the decision of which children should receive imaging and for whom it can be safely avoided.14–16
To address these concerns, attempts have been made to risk stratify patients with blunt trauma, identifying those at higher risk of CSI, and thus in need of imaging, through the use of clinical decision rules (CDRs). The most well known of these are the US derived National Emergency X-Radiography Utilization Study Low Risk Criteria (NEXUS)17 18 and the Canadian C-Spine rule (CCR).19 The CCR has not been validated in children although use or modified use in paediatric cohorts and guidelines has been described.15 16 20 The validity of NEXUS in younger paediatric cohorts has been questioned given the limited number of included children with CSI.3 16 21 Some studies applying rule criteria retrospectively3 21 have found neither perform well enough for use in children under 8 years. More recently, the Pediatric Emergency Care Applied Research Network (PECARN)22 described eight variables associated with paediatric CSI which, if applied as CDR, would have detected 98% of CSIs in their retrospective derivation cohort and may have reduced imaging rates in this population by up to 25%.
In the absence of a better tool, and despite concerns with applying essentially adult-derived CDRs for CSI to paediatric populations, these rules and proposed rules are often used ad hoc in practice to guide clinician decision making in children presenting with blunt neck trauma. They may be used in combination or with individual practitioner or institutional modification based on clinical experience.4 20 All three CDRs were likely known at our centre at the time of the study and were referenced in a local practice guideline. Given the paucity of information in paediatric CSI assessment, we set out to determine CSI incidence, imaging rates and the frequency of previously identified CSI risk factors, and thus assess the projected impact on imaging rates if CDRs were strictly applied as a rule for imaging in our population.
Methods
Study setting and design
A prospective observational study was conducted within the ED of a specialist paediatric hospital in Brisbane, Australia. The hospital is the state’s only paediatric trauma centre, serves a population of 4.9 million and has an annual ED census of over 65 000. Participants were recruited over 1 year (September 2015 to September 2016).
Participant selection
Participants were eligible for inclusion if they were aged under 16 years and met at least one of the following: (1) immobilisation pre arrival for possible CSI, (2) presentation with neck pain in the context of trauma or (3) otherwise considered at risk of neck injury by the ED team (eg multi- trauma patient or trauma patient with abnormal neurology, posturing or altered consciousness level). Participants were excluded if they declined participation, did not wait to be seen or a successful follow-up phone call was viewed as unlikely (eg overseas resident, no easily identifiable guardian, transient living situation, insufficient English language). Children assessed by our ED clinicians as having had their cervical spines fully assessed and cleared at another hospital prior to transfer for the definitive management of other injuries were excluded.
ED clinical staff identified and enrolled patients. No specific guidance on management, including imaging, was given and staff were instructed to manage patients as they normally would.
Verbal consent for inclusion was obtained in ED by clinical staff or by research staff during telephone follow-up. An ethical waiver of consent for inclusion was granted for children who died (or had a family member die) of injuries associated with their presentation.
Data collection and measurements
Data were collected at three discrete times: initial clinical assessment, post-discharge medical record review and telephone follow-up 1–3 months post presentation.
Telephone follow-up was conducted to ensure no CSIs were missed. It was attempted for all patients apart from those with a waiver of consent (maximum six attempts). Where follow-up identified patients imaged outside the study hospital, radiology reports were requested and reviewed. Patients unable to be contacted were not excluded if consent had been obtained in ED. In these patients, hospital records were rescreened for possible missed injury or representation. As our hospital is the only paediatric spinal referral centre in the large geographical area it serves and the community of paediatric spinal surgeons is small, it was thought highly unlikely that a significant injury would have been missed in this process.
Presentation details (history, prior imaging, mechanism, examination) and initial management plan were recorded on initial assessment. Imaging, admission or operative details were collected on later record review. Participants who received cervical spine imaging prior to ED arrival were excluded from further analysis in this paper.
The presence of CDR-specific criteria was collected prospectively by clinicians (table 1).
Comparison of NEXUS, CCR and PECARN criteria: study type, ages, inclusion criteria and ‘rule’ features
Outcomes
Primary outcome was the presence of any radiologically-determined CSI as defined below. Secondary outcomes included rates of imaging and clinical clearance, and first-line imaging choice.
Definitions
Clinical clearance was defined as cervical spine clearance without imaging.
CSI was defined as any radiological CSI on XR, CT or MRI as reported by specialist paediatric radiologists. Clinically significant CSI has been variably defined in previously published studies.17–19 22
Suspected other substantial injuries were defined as injuries that were life-threatening, required surgical intervention or warranted inpatient admission consistent with another large paediatric study.22 This variable was collected at two time points: prospectively by clinicians based on information available during initial assessment in ED and retrospectively by researchers when complete clinical notes were available to assess for variation. Clinician assessment was considered the primary CDR variable.
The presence of distracting injury was determined by the clinician (no specific definition supplied). For comparison, the presence of a distracting injury was also determined retrospectively from clinical notes by the research team using the published NEXUS definition.17 Clinician assessment was considered the primary variable.
Triage urgency was categorised using the Australian Triage Scale where patients in categories 1, 2, 3, 4 and 5 are to be seen immediately and within 10, 30, 60 and 120 min, respectively.
For NEXUS and PECARN rules, children were considered ‘rule positive’ if they had at least one CDR variable definitively present. Both identify individuals to be at lower risk if no CDR criteria are present and suggest imaging may be avoided in these patients. In this study, when strictly applying CDRs to our population, we considered ‘rule positive’ children to have imaging indicated. Unknown and missing variables were considered as not present when assessing rule positivity to ensure projected imaging rates with strict rule application were not overestimated. The CCR was more complex to apply due to the stepwise nature of the rule itself and an unintended omission in our study variable collection where we did not identify the specific presence of two of the five low-risk features which determine suitability for neck movement assessment (seated position on ED arrival, simple rear end motor vehicle collision). As such, we could only determine a minimum number of ‘rule positive’ individuals in our study. Children were thus defined as CCR ‘rule positive’ if they had a definite indication for imaging as defined by positive high-risk features or documented neck movement restriction to less than 45° (table 1). Strictly applied, the CCR excludes children. It also excludes those with a Glasgow Coma Scale Score<15, acute paralysis and known vertebral disease. For study purposes, these children were considered ‘rule positive’ with imaging indicated.
Data management and analysis
Data were directly entered into a Redcap database.23 Quantitative data including descriptive and comparative analyses were undertaken using SPSS V.25 (IBM Corp, Armonk, NY).
Patient and public involvement
Patients and the public were informally involved in the design and conduct of the research. No formal patient advisory group was established but is intended for future-related projects.
Results
A total of 973 children who had not received imaging prior to arrival were assessed for possible CSI (figure 1). Five children (0.5%) had CSIs. Loss to telephone follow-up rate was 6.8%. As per our previously stated rationale, these children have been included in the analysis. There were no known missed injuries.
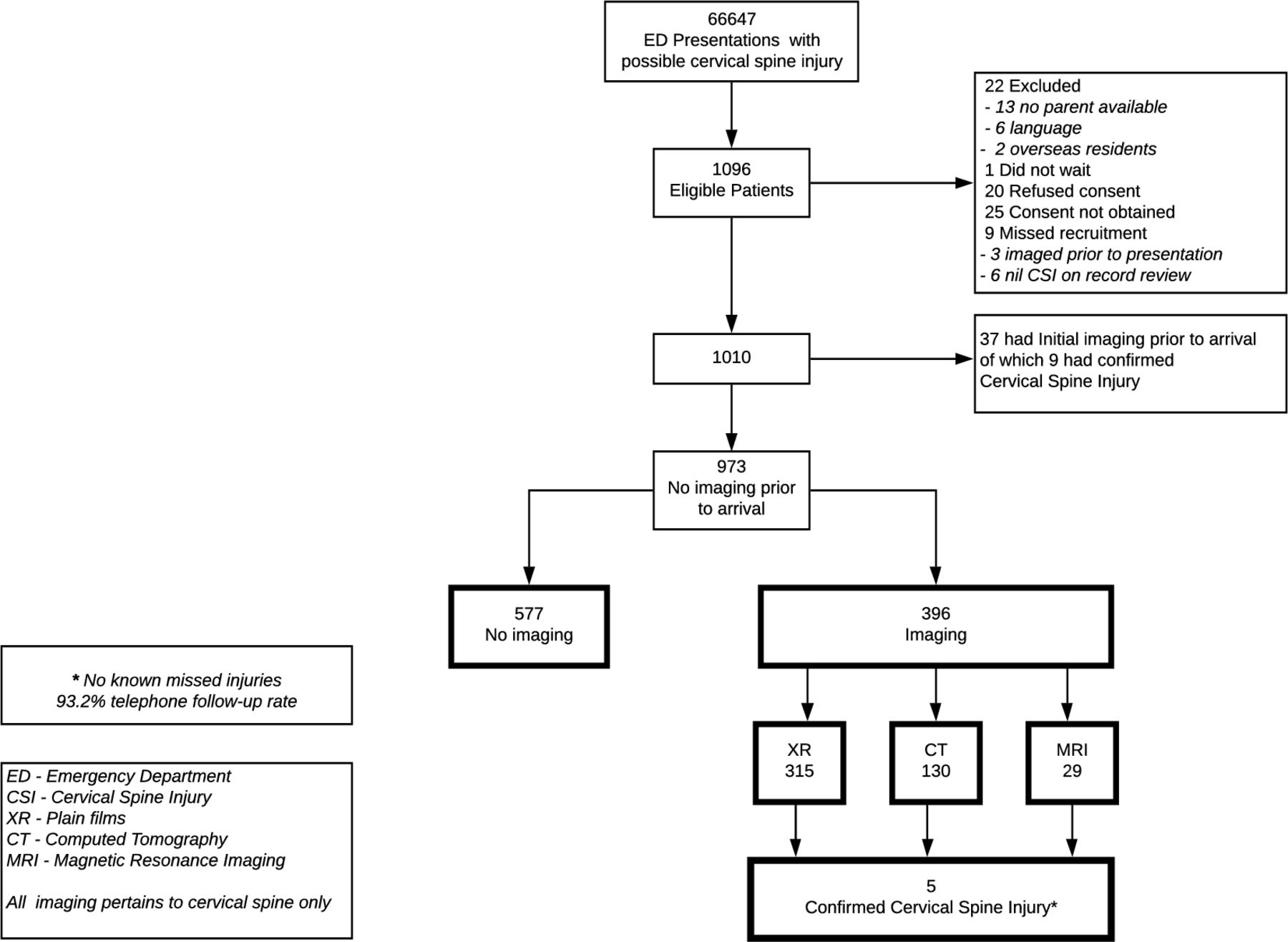
Children aged less than 16 years assessed for possible cervical spine injury across 1 year.
Demographics, mechanism of injury and imaging undertaken
Sixty-six percent of participants were male. Median age was 10.9 years; 30% were aged under 8. Injury mechanism was identified as a fall in 54.5% and motor vehicle related in 21%. Seventy-three percent arrived directly via ambulance, a further 3% respectively arrived as a primary retrieval or interhospital transfer and 20.6% via private transport. Ninety percent were triaged 1–3 by Australasian Triage Scale (table 2).
Children assessed for possible cervical spine injury with no prior imaging (n=973): demographics, mechanism of injury, imaging and outcomes
Glasgow Coma Scale Score was 15 in 92%. Neck pain was the most common complaint (45.9%), followed by tenderness on examination (42.9%); only 27.4% had definite posterior midline tenderness. Overall, 6% of participants had focal neurology and 23.9% suspected substantial other injuries.
In children presenting with no prior imaging, 40.7% had their cervical spine imaged after ED arrival; 32.4% received XRs, 13.5% a CT and 3% MRI. Nearly all (98%) XRs and CTswere conducted while the patient was in ED.
Prevalence of individual CDR criteria in children without prior imaging
The prevalence of CSI risk factors identified in NEXUS, CCR and PECARN studies in our population is shown in figure 2, alongside the percentage of children imaged in our population with these individual risk factors.

{kind=link}
{kind=link}
Presence of individual rule criteria in cohort and percentage of children actually imaged with each criteria (n=973). CCR, Canadian C-Spine rule;16 CSI, cervical spine injury; ED, emergency department; GCS, Glasgow Coma Scale Score; MV, motor vehicle; MVA, motor vehicle accident; NEXUS, National Emergency X-Radiography Utilization Study Low Risk Criteria;14 15 PECARN, Pediatric Emergency Care Applied Research Network.19
CDR positive
NEXUS
A total of 430 children (44.2%, 95% CI 41% to 47%) definitively met ≥1 NEXUS criteria (excluding unknowns), that is, were CDR positive (table 3). An online supplemental table shows the impact on this number when risk criteria definitions are varied.
Supplemental material
Number of CDR-positive (+) children* and number of CDR+ children actually imaged (n=973)
Of the 430 considered NEXUS CDR-positive, 325 were imaged (75.6%).
PECARN
The number of children positive for at least one of the PECARN criteria varies according to how certain risk variables are interpreted (online supplemental table). When any history of neck pain (pre-hospital or ED) in a child aged 2 years and older, and any restriction of neck movement, is considered, this percentage is 68.1% (663 children,95% CI 65.1% to 71.1%).
Of the 663 children meeting with these criteria, 359 were imaged (54%).
CCR
For reasons discussed, CCR positivity is more difficult to interpret and only a minimum number can be calculated. Using only definitive indications for imaging as specified in the ‘Methods’ section and the most conservative estimates of bicycle collision, 472 children (48.4%,95% CI 45.3% to 51.7%) would have had imaging indicated.
Of the 472 with definitive CCR imaging criteria, 236 (50.0%) were imaged.
Percentage of children imaged who were CDR positive
A total of 396 children (40.7%) without prior imaging received imaging in ED. Of these, 82.1% of all imaged children were rule positive for NEXUS (85.3% if any NEXUS criteria were positive or unknown); 90.7% were positive for the most inclusive PECARN interpretation (91.4% if at least one positive or unknown criterion).
Children with cervical spine injuries
Five children had CSI. Ages ranged from 7 to 14 years (median 10.9); all were males. Mechanisms were varied and included vehicle-related, contact sports and falls. Clinical features also varied—intubated (2), neck pain (3) and abnormal neurology (1). CT was performed as first-line imaging in three children, XR in two. First-line imaging did not identify the injury in two cases (one CT, one XR). Injuries varied: C1 fractures, annular tears, upper cervical spine anterolisthesis with oedema, cord oedema and ligamentous injuries. Three children had upper CSIs only (occiput—C2), one lower and one both.
All three CDRs identified the children with CSI.
Online supplemental table describes the impact of varying CDR interpretation on the number of CDR-positive children and number of CDR-positive children actually imaged.
Discussion
The incidence of CSI in our population among those assessed for possible CSI was low (0.5%). This is consistent with other published studies1 2 and with our sample size precludes formal validation of the CDRs studied. Despite this low CSI incidence, over 40% of children assessed for possible injury received imaging.
While the three CDRs identified all children with radiologically confirmed CSI, projected imaging rates when any of the studied CDRS were strictly applied in our cohort ranged from 44% to 68%, highlighting the potential for strict application of these CDRs to further increase imaging rates in our population. This unintended consequence of CDRs has been noted previously with the desired high sensitivity often achieved at the expense of specificity.24 For CDRs in paediatric CSI assessment, both less than perfect sensitivity and lack of specificity (with high imaging rates) carry significant risks and costs. The challenge lies in balancing the risk of missed spinal injuries against an increased risk of future malignancy, excess resource use and unnecessary immobilisation and potential sedation-related adverse events.
Currently, there are no well-validated paediatric CDRs, although both CCR and NEXUS rules are often used in practice to inform clinical decision-making and institutional guidelines. The CCR19 was derived from a cohort of 8924 patients aged 16 years and older. While it has been suggested that the CCR may have better diagnostic accuracy than NEXUS in adult subjects25 and includes mechanism of injury (identified as an important predictive factor in other paediatric CSI studies),22 26 the CCR has not been validated in a paediatric cohort.
The NEXUS study of 34 069 patients included 3065 patients younger than 18 years and had 100% sensitivity in identifying paediatric CSI (95% CI 87.8 to 100%).18 Of the 30 children with CSI, only four were aged under 9 years (none under 2). As noted by the authors and others since,3 16 21 this questions the validity of this rule in younger children. One paediatric retrospective single-centre study of 187 children with CSI (34 younger than 8 years) found that two to nine CSIs would have been missed in children<8 years by strict NEXUS criteria application; sensitivity was 100% among older children.3 Another retrospective case–control study21 found that neither CCR nor NEXUS performed well enough to be used as designed in children younger than 10 years.
A recent Cochrane review16 identified similar concerns with both rules, finding insufficient evidence for use of CCR in paediatric cohorts, advising caution with NEXUS use in paediatric patients given sensitivity concerns and finding no evidence for use in children under 8 years. Future large multicentre studies are needed to assess individual CDR performance and projected effects on imaging rates across different paediatric age groups, with particular consideration given to younger cohorts.
PECARN sought to redress the paucity of paediatric-specific CSI CDRs, publishing a retrospective study (540 children with CSI across 17 centres, case-matched against controls) identifying eight CSI-associated variables22 and a subsequent prospective study of 4000 children assessing the performance of the retrospective and a de novo model.27In the retrospective study, the presence of one or more factors was 98% sensitive for CSI (95% CI 96% to 99%) with a possible 25% decrease in imaging if these factors were applied as a CDR. In the prospective study, the retrospectively derived criteria had a sensitivity of 90.5% (95% CI 83.9 to 97.2) and specificity of 45.6 (95% CI 44.0 to 47.1). In our study, while these retrospectively derived criteria identified all children with injuries, strict application would potentially have increased our imaging rates. The baseline imaging rate in the prospective PECARN study was also higher than ours (78% vs 41%). This may be due to differing inclusion criteria, however, it may also relate to differences in local imaging practices; lower imaging rates have been described for paediatric head injury in Australia and New Zealand when compared with North American studies.28
In addition to identifying all serious injuries, imaging-related CDRs also often aim to safely reduce imaging rates. This is particularly important in children where exposure to ionising radiation has been associated with increased lifetime cancer risk.5–8 Strict application of all three CDRs or proposed CDRs in our cohort may have potentially increased imaging rates. As the CDRs investigated were known at the study hospital, it is possible that their criteria have already influenced clinical decision-making. Collection of predictor variables was not linked to specific CDR or tool guidance, however, the conduct of the study may have influenced clinical decisions. We are unable to compare the study imaging rates with data in a preceding period as only prospective case identification would have provided a comparable denominator. Current CDRs do not address the other pressing question of paediatric cervical spine assessment—not only who we should image, but how, that is, which modality we should be using. In our cohort, 13% children underwent CT imaging, 25% of these children first received XRs.
This study was a single-centre cohort with low numbers of CSI. As such, formal validation of any CDR is not possible. Similarly, no child required operative intervention for their injuries although one of the four who died had a significant CSI. No missed injuries were identified, however, 6.8% of children were lost to telephone follow-up and thus the potential, albeit unlikely, exists. Varying definitions and clinical interpretation of criteria such as distracting injury and substantial torso injury may influence the number of ‘rule positive’ children, however, little difference was found when we varied criteria interpretation. Using clinician interpreted criteria may better reflect real world application. CDR positivity may also vary across different paediatric age groups (eg infants vs adolescents); our numbers were too low to accurately explore this. While our study was done in a single paediatric centre and this may limit generalisability, it does highlight concerns with CDRs as currently exist for paediatric CSI.
While CSIs are uncommon, the potential for missed injury still clearly concerns clinicians given current imaging rates. Available CDRs offer some guidance but should be interpreted with caution due to the potential for increasing imaging rates in children presenting for assessment. Further multicentre research should be considered to formally validate the rules currently in use in adults and those newly developed for children; and to determine whether a more refined tool for paediatric patients, particularly for those at younger ages, can be developed.
Data availability statement
Deidentified data are available on reasonable request and with appropriate permissions from regulatory authorities.
Ethics statements
Ethics approval
The Children’s Health Queensland Human Research Ethics Committee, Brisbane, Queensland, Australia, approved the study (HREC/14/QRCH/56).
Acknowledgments
The authors would like to thank patients, families and staff at the Queensland Children’s Hospital (QCH) Emergency Department, Brisbane, Australia, research staff from Paediatric Emergency Research Unit, QCH—Erin Inwood, Kelly Foster, Trey McHale and Christopher Phillips and Sharon O’Brien and Meredith Borland of the Perth Children’s Hospital for their input into study case report form design.
References
Footnotes
Handling editor Richard John Parris
Contributors All authors designed the study, approved publication, contributed substantially to its revision and agreed to be accountable for all aspects of its work. NP conceived the study. NP, K-AA, SM, KR, JA and RB undertook recruitment and managed the data including quality control. NP and FEB provided statistical support. NP analysed the data, wrote the initial draft of the article, provided overall supervision and takes responsibility for the paper as a whole.
Funding The study was funded by a grant from the Emergency Medicine Foundation (Australasia) Queensland Program—EMSS-404R21-2014. NP, JA, RB, GA and MW obtained grant funding.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.