Article Text

Abstract
Introduction There is currently concern in the UK that injuries and deaths caused by firearms are increasing. This is supported by small local studies but not by wider research to inform targeted prevention programmes.
Methods A retrospective analysis was performed of firearm injuries from the Trauma Audit and Research Network (TARN) database (1998–2007), the largest national registry of serious injuries. Data were analysed to determine temporal trends in the prevalence of firearm injuries and demographic characteristics of firearm victims. The UK Office of National Statistics provided data on all deaths by firearms as TARN does not record prehospital deaths.
Results Of 91 232 cases in the TARN database, 487 (0.53%) were due to firearm injury. There were 435 men and 52 women of median age 30 years. The median New Injury Severity Score in men was 18 with a mortality of 7.4%, compared with 15.5 and 3.8% for women. The highest rate of firearm injuries as a proportion of all injuries was submitted from London (1.4%), with the South East (0.23%) submitting the lowest rate. 90.5% resided in urban areas, 78% presented outside ‘normal’ hours and 90% were alleged assaults. As a proportion of all injuries submitted, a small upward trend in the prevalence of deaths due to firearms was demonstrated over the study period. An increase in homicides since 2000 was also noted with an increasingly younger population being involved. In contrast, data from the Office of National Statistics showed that the greatest number of deaths were self-inflicted rather than homicides (984 vs 527), with Wales having the highest number of such deaths and predominantly involving older men.
Conclusions Deaths and serious injuries caused by firearms remain rare in the civilian population of England and Wales, although an upward trend can be described. Victims of assault and homicide are predominantly young men living in urban areas and the population involved is getting younger. However, of all deaths, self-inflicted wounds are nearly twice as common as assaults, affecting predominantly older men living in more rural areas.
- Firearm
- gun
- homicide
- assault
- death
- injury
Statistics from Altmetric.com
Introduction
UK police, politicians and media describe the emergence of a ‘gun culture’, particularly in some inner city areas. These descriptions, in combination with a number of recent high profile firearm homicides throughout the country, have generated concerns that civilian deaths and injuries caused by firearms are increasing. In 2005, according to the US Centre for Disease Control there were 12 337 homicides and 69 825 non-fatal injuries caused by firearms.1 In contrast, UK Home Office figures for 2005/6 cite 49 homicides and 4955 non-fatal injuries.2 The figures remain low by comparison, thought mainly to be due to the UK's strict gun control laws. However, despite progressive tightening of the legislation since the 1980s, the annual reported incidence of firearm crimes where injuries were sustained by non-air weapons has shown an upward trend (figure 1).2
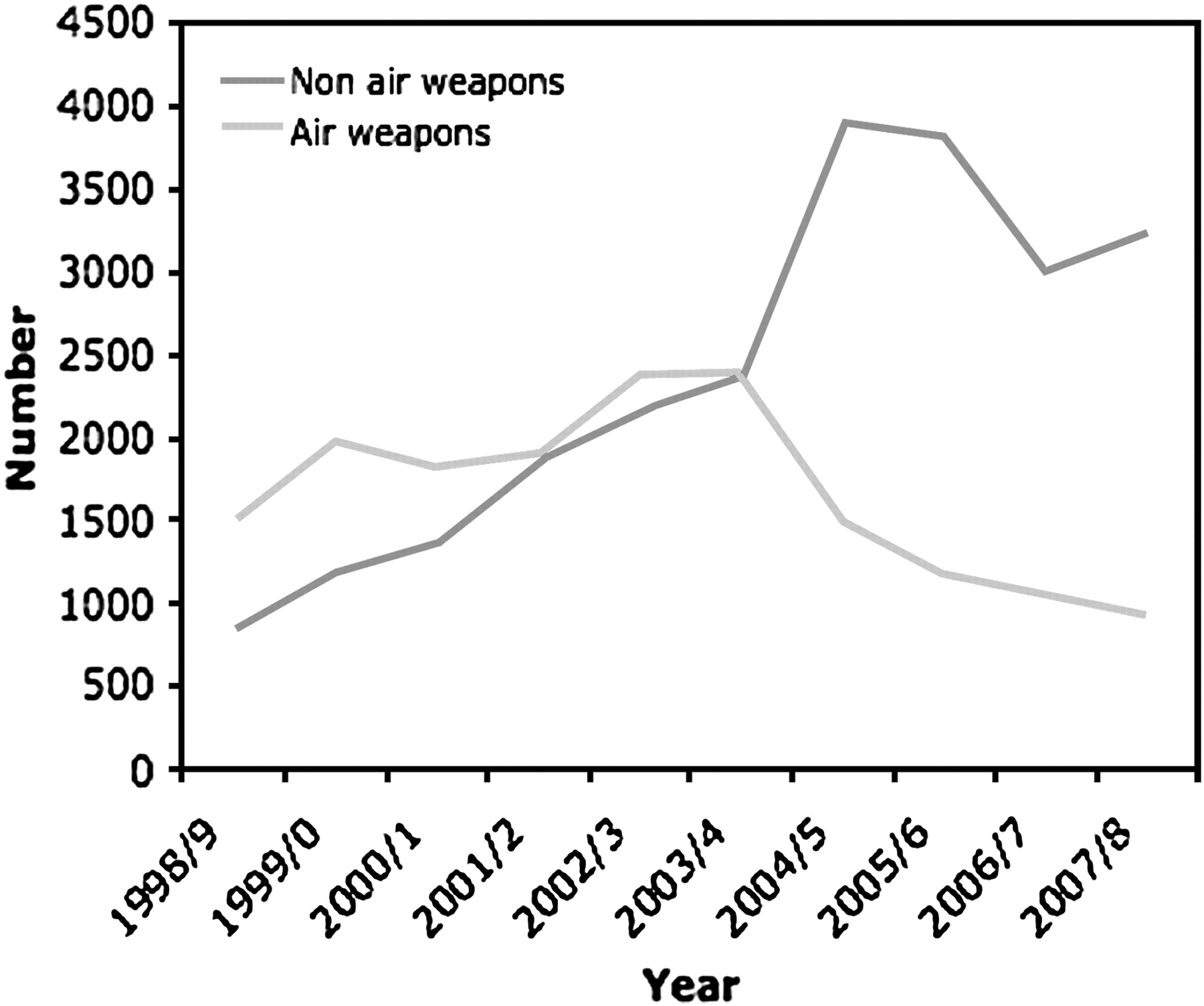
Crimes recorded by police in England and Wales in which firearms were used and injuries sustained.
Fifty-five per cent of all non-air weapon firearm offences in England and Wales occurred in just three police authorities (Metropolitan (Greater London), Greater Manchester and West Midlands), with 35% of the non-air weapon firearm offences occurring in the Metropolitan Police area alone.2 Internationally, large-scale urbanisation has been associated with increased levels of firearm use and injury.3 The Home Office figures are reflected in a number of UK studies demonstrating an increase in firearm injuries seen in emergency departments (EDs).4 5 Persad et al noted a fourfold increase in their inner city London ED between 1998 and 2002.5 Men are over-represented as victims of firearm crime in UK and international studies.6–8 A review of 187 admissions over a 54-month period in Manchester found that 162 men (87%) were injured compared with 25 women (13%).6 Victims also tend to be young. This same study found that the mean age of patients was 21 years with 66% being aged <25 years. These findings are replicated in other UK studies.4 5
People from minority ethnic groups have also been shown to be over-represented among victims of firearm injuries. One UK study found that, of 61 patients who were admitted, 84% were of African-Caribbean or mixed race. However, this distribution was very different to the ethnic distribution in the local catchment area with minority ethnic people being disproportionately affected.5 These UK studies reflect international studies into the demographics of civilian firearm injuries which show young black men to be at higher risk.9 10 It is also of note that, although the calendar distribution of these injuries has been shown to be fairly even,4 the vast majority of victims are admitted outside normal working hours. Indeed, one UK study showed that 68% attended during this period and had significant service implications.5
Detailed epidemiological information is the basis for planning the control and prevention of disease in communities. In the USA, such data has been used to inform a number of gun control strategies, some of which have shown significant falls in gun crime and injury.11–13 However, little is known about the epidemiology of patients seriously injured or killed through civilian use of firearms in the UK.4 Previous studies have been small and localised to individual centres in major inner city areas.4–6 The purpose of this study was to perform a wider analysis of firearm injuries and deaths throughout England and Wales, identifying trends over time and the demographic and injury characteristics of those injured. Such information will enable us to direct injury prevention methods appropriately.
Methods
The Trauma Audit and Research Network (TARN; which includes around 70% of trauma receiving hospitals in England and Wales) collects data on patients attending participating hospitals who sustain an injury resulting in immediate admission to hospital for ≥3 days, admission to an intensive care or high dependency unit, or death within 93 days. Patient data are recorded at the time of discharge and entered remotely onto the TARN database. All patient identifiers are removed. Details of TARN have been described previously.14
TARN classifies injuries using the Abbreviated Injury Scale (AIS)15 and records the anatomical severity of injuries using the New Injury Severity Score (NISS).16 NISS is defined as the sum of the squares of the AIS of each of the patient's three most severe AIS injuries, regardless of the body region in which they occur.
We carried out a search of the TARN database from 1 January 1998 to 31 December 2007 to identify all patients who had been injured by firearms. Information was collected on the prevalence of such injuries, both regionally and nationally on the database, and the characteristics of those involved. Timing of the incident was taken as the time the patient was booked into hospital. Information regarding ethnicity was unable to be analysed as it is not routinely collected. It was also not possible to determine the type of firearm or characteristics of bullet used (whether the weapon was an air weapon or non-air weapon).
Classification of the patients' residential area was obtained by cross-referencing each patient's home postcode sector with the UK Office of National Statistics (ONS) Rural and Urban Area Classification 2004. Regional population figures were taken at mid-2004 estimates by the ONS. The total number of firearms covered by certificate was taken as at 31 March 2006.17
The annual prevalence of firearm injuries was calculated as a proportion of all injuries submitted to TARN. Regionally, the prevalence of firearm injuries was again calculated as a proportion of all injuries. Rates were calculated with 95% CIs and median values were used to describe non-parametric data with interquartile ranges.
As TARN only records data on patients reaching hospital alive, in order to provide a complete epidemiological picture the UK ONS were asked to provide data on all firearm deaths as registered on death certificates (excluding deaths caused by legal intervention or war). Data were extracted from the SOPHIE database identifying underlying cause of death between 1 January 1998 and 31 December 2007 that were given International Classification of Disease (ICD) codes consistent with death by firearm injury (ICD-9 codes E922, E955, E965.0–E965.4 and E985.0–E985.4 for 1998–2000 and ICD-10 codes W32–W34, X93–X95, X72–X74 and Y22–Y24 for 2001–2007). Cases were analysed by year of death occurrence, age at death, geographical region of death certification, gender and intent (unintentional, undetermined, homicide or suicide).
Results
From January 1998 to December 2007 the TARN database held data on 91 232 trauma cases and, of these, 487 (0.53%) were due to firearm injuries (table 1).
Trauma Audit and Research Network firearm injuries: patient demographics, injury severity and outcome by gender
The median length of stay in hospital was 8.8 days (IQR 4–10), with 31% of patients being admitted to the intensive care unit. In 446 cases (91.5%) where the level of the most senior ED doctor treating the patient was known, 37.4% received consultant input, 16.2% were managed by registrar level doctors and 37.9% were managed by senior house officer/foundation grades.
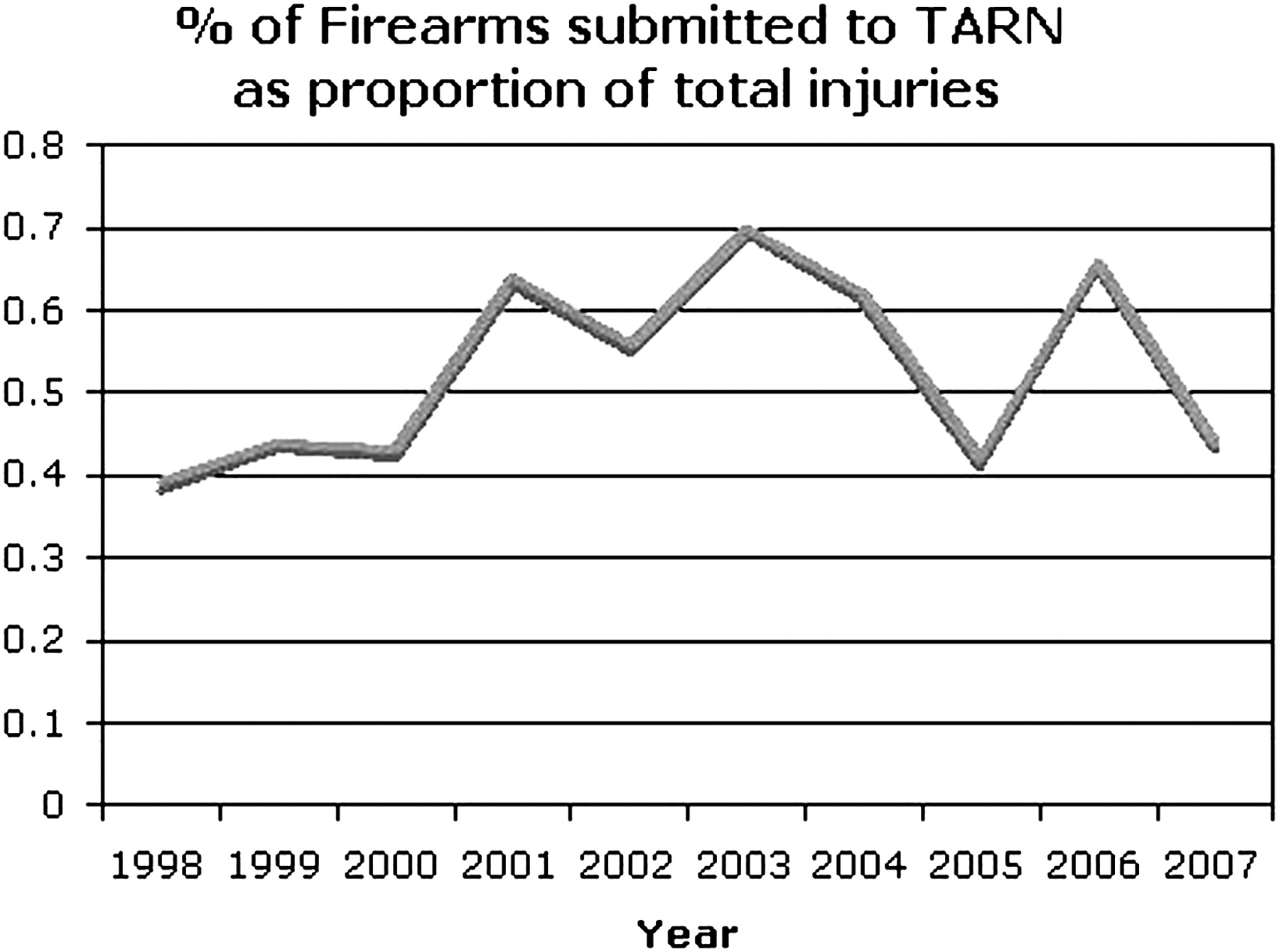
As a proportion of all injuries submitted to TARN, firearm injuries have shown a number of annual peaks and troughs (figure 2). The highest number of cases was reported in 2003 with 73 cases (0.7% of total submissions), while only 32 cases (0.39%) were reported in 1998.

Annual percentage of firearm injuries submitted to the Trauma Audit and Research Network (TARN) as a proportion of total injuries.
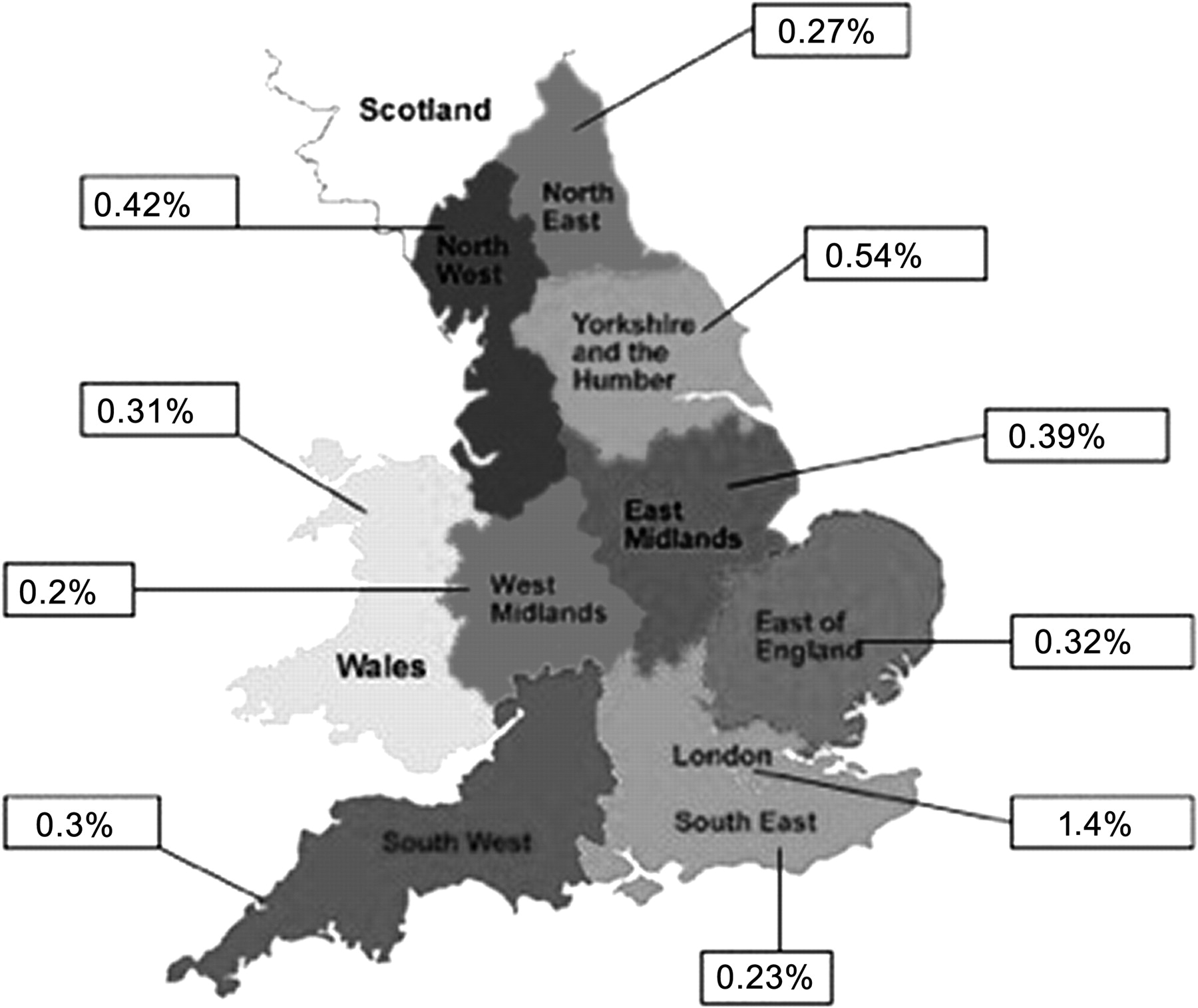
Analysis by region reveals geographical variation as shown in figure 3. The highest prevalence of firearm injuries as a proportion of all injuries was seen from hospitals in the London region followed by the North West. The South East and North East submitted the lowest. Of those injured, over 90.5% resided in urban areas.
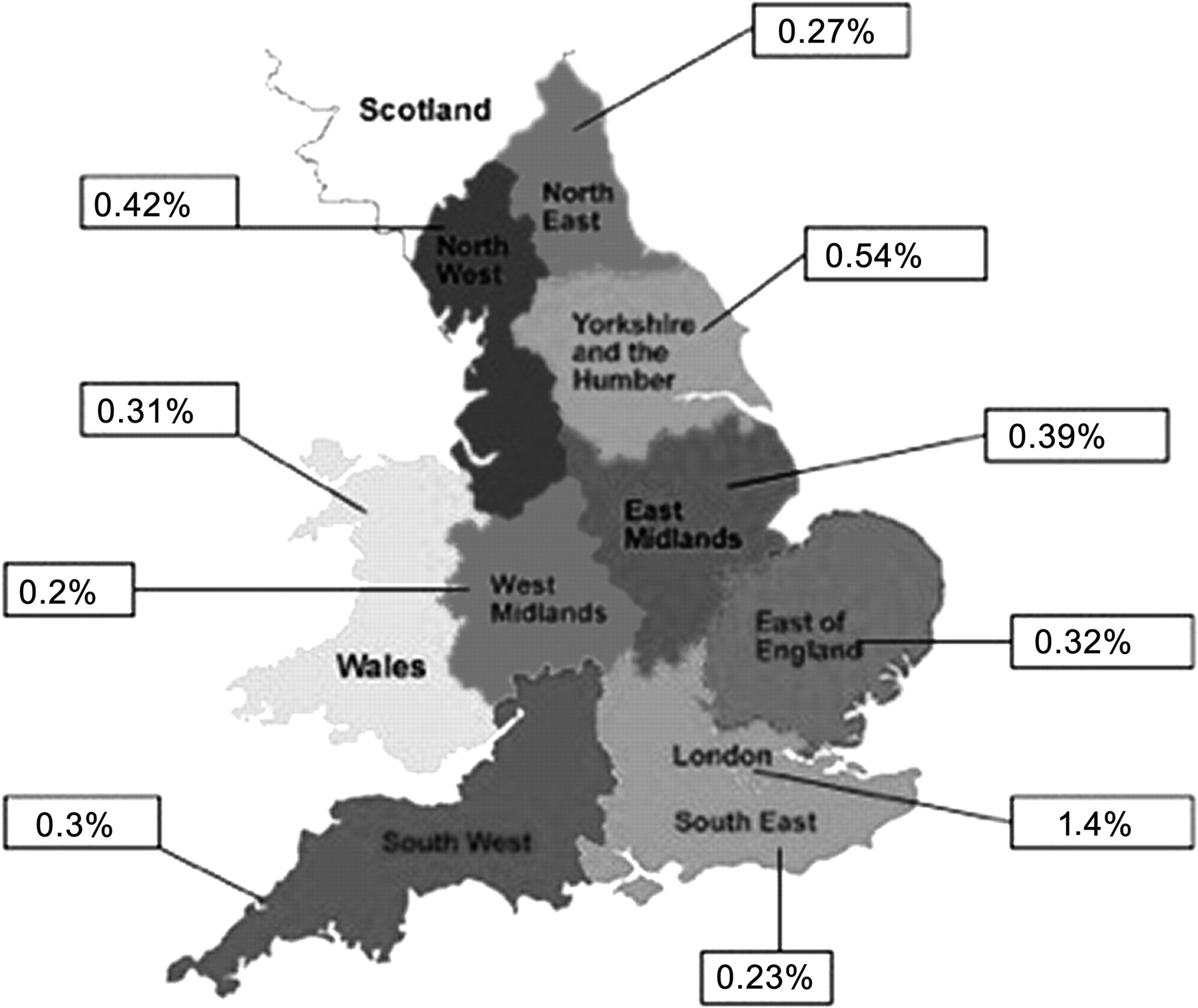
UK regional map representing prevalence of firearm injuries as a percentage of total injuries submitted to the Trauma Audit and Research Network, 1998–2007.
There was no seasonal variation in numbers presenting. In most months an equal (1/12) proportion of patients presented (40–50/month) with June (n=30) and December (n=28) having the lowest attendances and May the highest (n=50). Saturday (n=86), Sunday (n=81) and Monday (n=85) attracted most admissions compared with Tuesday (n=59), Wednesday (n=50), Thursday (n=64) and Friday (n=62). Indeed, 78% of all cases presented to the ED outside ‘normal’ working hours (Monday–Friday 9:00–17:00).
Of 357 cases where injury intent was documented, 90.4% were alleged assault. A further 4.3% were accidental and 2.5% suspected self-harm. This is in contrast to ONS data (table 2) showing that the greatest numbers of deaths from firearm injury were self-inflicted. However, ONS statistics correlate well with TARN data in that London and the North West were shown to have the highest number of firearm injuries and deaths due to assault. The same two regions have the lowest number of deaths through self-inflicted injury, while Wales and the South West have the highest.
Firearm deaths by intent, region and gender (1998–2007) and number of firearms covered by certificate per 100 000 population (data from UK Office of National Statistics)
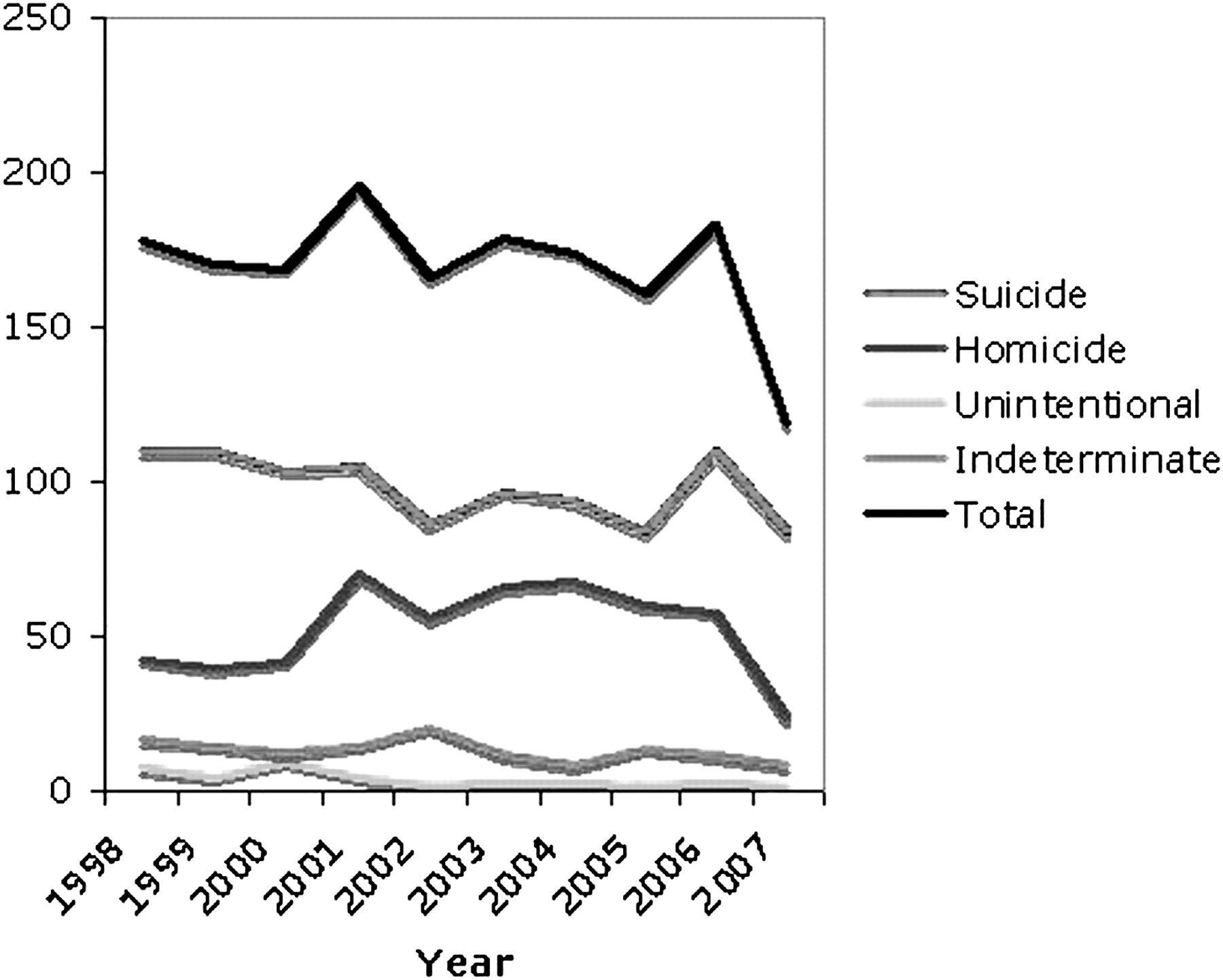
Despite peaks in 2001 and 2006, overall the total number of deaths from firearms as documented by the ONS has remained relatively stable over the 10-year period (figure 4). An increase in homicides occurred from 2000 to 2006, but this has been matched by a fall in the number of suicides from 2001 to 2005. Death from unintentional causes has remained consistently low. A fall in both homicides and suicides in 2007 accounts for the substantial drop in overall deaths seen during this period.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Firearm deaths in England and Wales by year and mode, 1998–2007 (data from UK Office of National Statistics).
Breaking down the ONS data into age group and intent, homicide through the use of firearms affects a young population with those aged 20–29 years being most at risk. Over the 10-year study period the age profile of those killed by homicide has changed. In 1998 only 14% of homicides involved 10–24-year-olds but, by 2006, this had reached a peak of 52%. Suicide, however, mainly affects an older age group, with a peak at 50–59 years before tailing off (figure 4).
Discussion
This is the first national study to analyse the numbers and characteristics of civilians seriously injured and killed by firearms in England and Wales over a 10-year period.
Despite peaks and troughs, the number of firearm injuries submitted to our trauma registry as a proportion of all injuries is low, although it does demonstrate a small upward trend. This is consistent with government statistics and lends support to media concerns that more people are being injured through firearm crime in the UK than previously.
The number of deaths by assault has increased since 2000 but remains relatively stable and has shown a fall in number during 2007. This may reflect the diminishing relative lethality of the firearm stock in England and Wales (so-called ‘junk guns’) or a growing trend of those using them to intentionally maim rather than cause death. The majority of patients on our registry had relatively moderate injuries as defined by NISS, and this may again be due to the use of low energy transfer weapons that have been shown to be mostly used in UK civilian assaults.2
The vast majority of those injured and treated in hospital were young men who resided in urban areas, with London and the North West seeing proportionately more. Over 90% obtained their injuries due to assault. The UK ONS supports these figures by showing a similar correlation. Worldwide, the majority of assaults by guns is an urban phenomenon, thought to have an association with social exclusion, gang culture and illicit drugs.18
Nearly three-quarters of all such injuries presented to the ED outside ‘normal’ hours when senior medical staff are less likely to be immediately available. A single bullet to the chest may well end up intra-abdominally leading to the need for a thoracotomy, laparotomy and repair of diaphragmatic, vascular and bowel injuries. These injuries pose a challenge to experienced military surgeons regularly exposed to the management of such wounds, let alone a surgical trainee in a local acute hospital. It is of concern that over one-third of patients on our registry were managed in the ED by junior doctors whereas a soldier shot in a military environment could expect a full consultant team resident in the hospital 24 h a day and immediately available for their reception.19
The lack of senior medical input into the initial care of trauma patients as a whole was a concern of the 2007 National Confidential Enquiry into Patient Outcome and Death report that found 64.5% of 183 hospitals sampled did not have a consultant trauma team leader in the early hours of a Sunday morning.20 Further work is planned to examine any relationship between time of presentation, seniority of care and outcome, and to consider the role of regionalisation of trauma services in optimising care for these patients.
Interestingly, despite concerns that inner city gun crime is out of control, the ONS data demonstrate that, although 527 people died from firearm injuries between 1998 and 2007 due to assault, nearly double that number (n=984) died from self-inflicted firearm injuries. The majority of these deaths occurred in the more rural geographical areas of Wales and the South West, with London and the North West—despite having the highest number of deaths from assault—having the lowest number of deaths by suicide. Only 2.5% of our registry firearm injuries were due to suspected self-harm, probably reflecting the known extremely high case death of attempted suicide by firearm.21
There have been relatively few studies of suicide by firearm in the UK. These have found that most are men, often aged in their 40s, and the UK ONS data support these findings.21 They are less likely to have current or past mental health problems than people who commit suicide by other means.22 A large US study that analysed urban–rural differences in intentional firearm deaths found that the most rural counties experienced 1.54 times (95% CI 1.29 to 1.83) the adjusted firearm suicide rate of the most urban, and highlighted the issue that firearm deaths are not solely an urban phenomenon.23
The international literature shows a strong association between rates of gun ownership and rates of suicide by firearm.24 This is reflected in our study, with the regions with the highest number of self-inflicted firearm deaths (South West, East of England and Wales) having the highest number of firearms covered by certificate per 100 000/population. Despite London having one of the lowest numbers of firearms covered by certificate and a low level of death by self-inflicted injury, the region has the highest number of deaths by assault and this may be due to the availability of illegal firearms not covered by certificate.
It is of note that, due to our registry's inclusion criteria, the patient population studied here reflects the most seriously injured. For example, many patients who receive minor air gun injuries or bullet wounds to soft tissues or the musculoskeletal system may well be conservatively managed and not admitted to hospital (or not present to hospital at all). Such patients are not taken account of by this study and consequently we may be underestimating the true trend. It is also the case that only around 50% of trauma receiving hospitals in the UK submitted data to our registry during the period of study, with some regions being over-represented (North West) compared with others (South East).
In conclusion, our data suggest that the rate of serious civilian injury and death caused by firearms in England and Wales remains low, although it has shown a slight upward trend over the past decade. It is of concern that those killed by firearms are becoming increasingly younger. The vast majority of cases seen in hospital are due to assaults and are primarily young men in urban areas. This poses significant service and training implications for the NHS of tomorrow, and also questions how we can target violence prevention efforts to appropriate groups as has been done successfully in other countries.
To do this, more research needs to be undertaken as to why young people turn to guns and how they access these weapons despite the UK having some of the tightest gun control laws in the world. Also, there are important gaps in how and where we record the true picture of gun crime and injury.
Notwithstanding the fear and intimidation that gun crime can produce in urban communities through assaults which drives public concern and media attention, this study also highlights a major public health issue that is occurring through the use of guns by self-inflicted injury in older men in England and Wales.
References
Footnotes
Funding MJD's salary was part funded by the National Institute of Health Research (NIHR) who played no further part in the study and the views expressed are those of the researchers, not the NIHR.
Competing interests None.
Ethics approval Permission has been previously granted by the Patient Information and Advisory Group (PIAG) for research on anonymised data held by the Trauma Audit and Research Network (TARN). Further ethical committee approval was not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement A complete dataset of Trauma Audit and Research Network (TARN) data is available on request to all researchers working at hospitals that submit data to TARN. ONS data are available to all (on payment of relevant fee).
Linked Articles
- Primary survey