Article Text

Abstract
Objective Consultant based delivery of emergency service is perceived to add value. This study aims to demonstrate the impact of such a service model based on consultant working in a UK emergency department.
Methods This retrospective study was based on the emergency department of a district general hospital. Activity data was analysed for 2009. Workload and admission rates were compared between consultants, middle grade doctors and senior house officers (SHOs). Admission rates were compared against two similar departments. Data from night shifts allowed consultant activity to be contrasted with middle grades and SHOs. Time spent in the department, admission rates, patients who left without treatment, discharged outright and clinic returns were used for comparison.
Results Consultants often saw more patients than SHOs or middle grade doctors. This was on top of their traditional duties of senior opinion. On comparison of activity at night shifts, they admitted fewer (25.2% vs 30.3%, p=0.026), had fewer leaving without treatment (1.6% vs 5.1%, p<0.001), discharged more outright (59.8% vs 47.5%, p<0.001), referred fewer to clinic (5.7% vs 6.6%, p=0.49) and had a faster turnaround time (p<0.001: Priority 2, 3 and 4) for every triage category. Some of the comparisons were clinically but not statistically significant.
Conclusion A consultant based service delivery offers many advantages. These cannot be matched by either junior or middle grades. This would be in addition to the consultants' supervisory role. Consultant expansion is urgently required to achieve this sustainably. A further study evaluating the cost benefits of this service model is now underway.
- Consultant delivered service
- consultant workload
- senior based service delivery
- 4-h target performance, length of stay
- audit
- emergency care systems
- emergency care systems
- admission aviodance
- emergency care systems
- effieciency
- management
- risk management
Statistics from Altmetric.com
- Consultant delivered service
- consultant workload
- senior based service delivery
- 4-h target performance, length of stay
- audit
- emergency care systems
- emergency care systems
- admission aviodance
- emergency care systems
- effieciency
- management
- risk management
Introduction
The service delivery for emergency medicine (EM) in the UK has traditionally been based on junior doctors. Although the medical staffing has been inadequate, as confirmed by a 2007 survey,1 the junior doctors have outnumbered the consultants and seen the bulk of the patients. The emergency department (ED) consultants have been supervisors and administrators.2
There are inherent weaknesses in this model. The junior doctors struggle with the clinical challenges of EM. The middle grade tier is fast disappearing. The College of Emergency Medicine has been campaigning to recommend a more active role for EM consultants in service delivery.3
Since 1996, the Wrexham ED consultants have delivered the service hands-on. This has been augmented by subsequent consultant appointments. Consequently, the ED workforce now has more seniors than juniors. The consultants engage in service delivery as well as serving their supervisory roles. Since 2008, the consultants have volunteered to work full night shifts on site, a practice unique in the UK. This change in service delivery came in response to near miss events during unsupervised (junior) shifts and a backlog of patients following such shifts. In addition, the juniors have demonstrated an increasing dependence on senior presence, as shown by the rate of senior opinion sought (recorded on our IT system) and their written complaints to the post-graduate deanery about unsupervised shifts.
We present quantifiable evidence of the impacts of a consultant delivered EM service.
Methods
The ED at Wrexham Maelor Hospital serves a catchment population of 300 000 from North and Mid Wales, Cheshire and Shropshire. The ED accepts unrestricted emergencies. In this retrospective study of 2009 activity, the department received 58558 new patients, 3868 unplanned reattenders (6.6%) and 1613 clinic returns (2.7%). The workload consisted of 0.6% Red (triage category 1), 17.1% Orange (category 2), 35.1% Yellow (category 3), 45.4% Green (category 4) and 1.7% Blue (category 5) patients. Of these, there were 22.9% children; 11.2% over the age of 75 years; 22% came by ambulance, and the admission rate was 15.7%.
There are eight junior doctors, five consultants, one specialist registrar (Specialty Training Registrar Year 4 and above) and seven SAS (Staff Associate Specialist) doctors. The juniors work full shifts, while the middle grades work shifts between 0800 and 2400. The five consultants work nine clinical sessions between 0800 and 2200 weekdays, 1000 and 1800 on Saturdays and Sundays, and are subsequently on call. Both middle grades and consultants participate in the night shifts (12:00–08:00) on a one in 13 basis consecutively from Mondays to Wednesdays.
We performed a retrospective analysis of 2009 activity from the clinical IT system (Symphony, Ascribe PLC). The Manchester Triage System has been in use since 1998.4 No special measures have been undertaken by any of the clinicians during this period. Since 2007, comparative data has been available between the three District General Hospitals in North Wales. The merger of these hospitals as part of Betsi Cadwaladr University Health Board has allowed triangulation of the Wrexham data against the other two departments, which are similar but provide largely junior delivered service.
The consultant night shifts in Wrexham started in January 2008 and are shared with the middle grades on a one in 13 basis. Each senior (consultant or middle grade) doctor works three nights between Mondays to Wednesdays and has one senior house officer (SHO) with them each night. The other four nights between Thursdays and Sundays are staffed by two SHOs. This has allowed straight comparison between the sets of nights worked by a consultant or middle grade or SHO, with the other SHO being constant. We summated the activity over 2009 for all Mondays to Wednesdays (consultant/middle grade and one SHO) and Thursdays to Sundays (two SHOs). This was split into three categories of consultant, middle grade and SHO night shift. The SHO nights of Thursdays to Sundays were similar but marginally busier, which therefore could potentially skew the data. So we included raw data and then adjusted the SHO night activity data by removing the busiest nights from the comparison. This ensured even comparison by removing the process impact of high volume night shifts. In contrast to our night activity, analysis of any other shift does not allow this triangulation because these are worked with a pool of consultants, middle grades and SHOs.
Clinical data was collected by the Symphony system and analysed with reference to 2009 duty rosters. The comparative data between the three North Wales departments were available to the Informatics Department. Insufficient data from those departments have precluded any further analysis of activity.
We present attendance trends, medical workforce size and admission rates in Wrexham since 2003. We have also compared the admission trends between the three North Wales hospitals between 2007 and 2009. The night shift analysis is based on 2009 data. We have compared the triage category split, various disposal modes and time spent in ED on three sets of nights. Finally, we have directly compared the above criteria for consultant versus middle grade nights and consultant versus SHO nights. We have used χ2 test for statistical comparison and Kruskal-Wallis H test for analysis of variance with SPSS (Windows, Rel. 11.0. 2004. Chicago: SPSS Inc.) software.
Results
The annual attendances at Wrexham have been increasing year on year, except a dip between 2006 and 2007. Consultant based service delivery started in 2003 and extended with consultant expansion. We have charted our patient numbers, admission rates and (table 1) our medical staffing to show trends in opposite direction.
Yearly attendance and admission rates shown against medical manpower (2003–2009)
Despite seasonal variations of activity and admissions, ED activity fell between 2005 and 2007, while re-attender and clinic attendances have steadily fallen between 2005 and 2009 (figure 1). This represents one impact of consultant working.
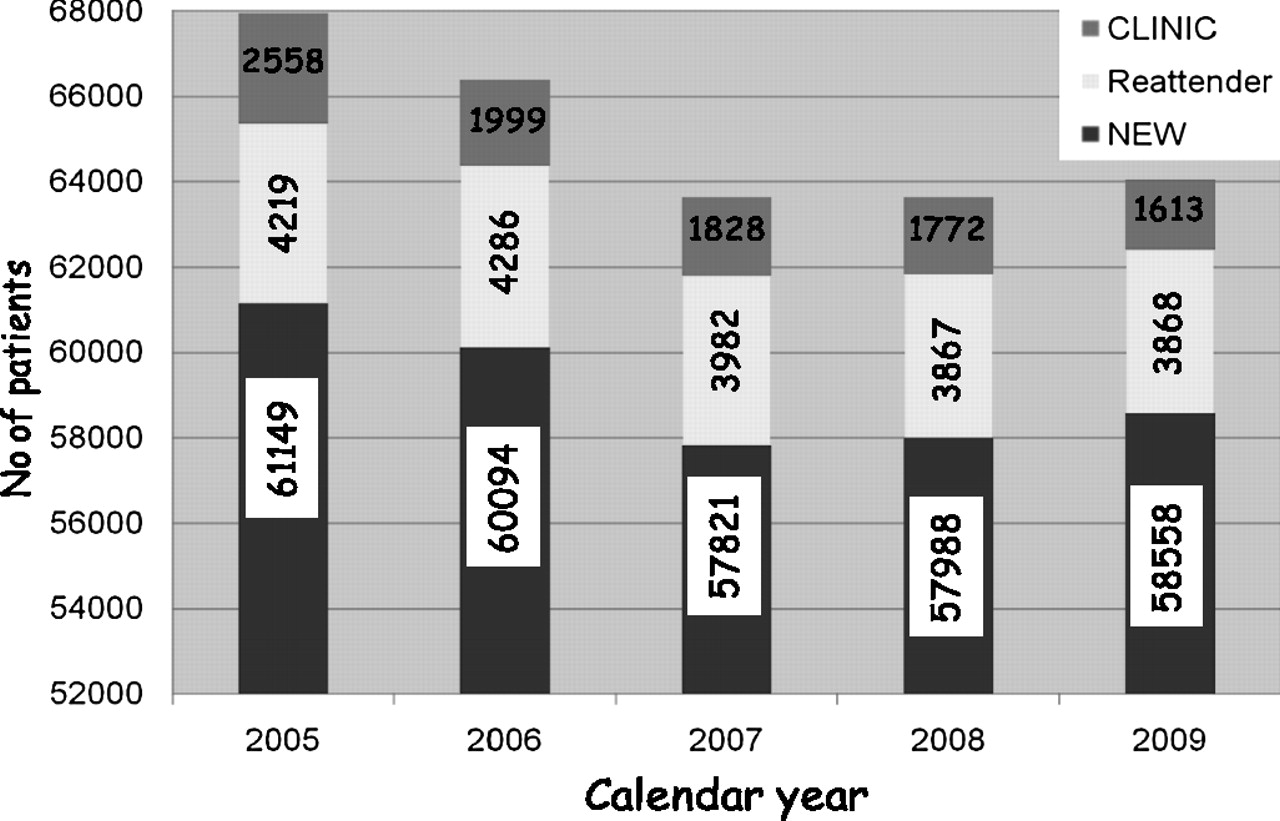
Attendances at Wrexham Maelor ED.
We also compared the patient numbers and admissions between the three North Wales EDs at Bangor, Glan Clwyd and Wrexham between 2007 and 2009 (table 2). These departments are closely matched in the age profile and triage category (dependency). Comparison of 2009 admission rates between Glan Clwyd and Wrexham (χ2=1937.18, df=1, p<0.001) and Bangor and Wrexham (χ2=2495.86, df=1, p<0.001) ED shows significantly lower rates at Wrexham. Due to difficulty with accessing detailed data from those two hospitals, no more in-depth analysis has been possible.
Comparison of ADMISSION PROFILE for 3 North Wales ED under BCUHB (2007–2009)
With established consultant shifts in 2009, it was possible to compare the consultant's workload with that of middle grades and SHOs. We compared five individual consultant's workload and admission rates over 12 months (figures 2 and 3) with six middle grades and three junior doctors. We selected doctors who worked over 12 months (rather than four) to allow consistency. This shows variable consultant workload and admission rates—the former mostly higher than SHO and the latter lower.
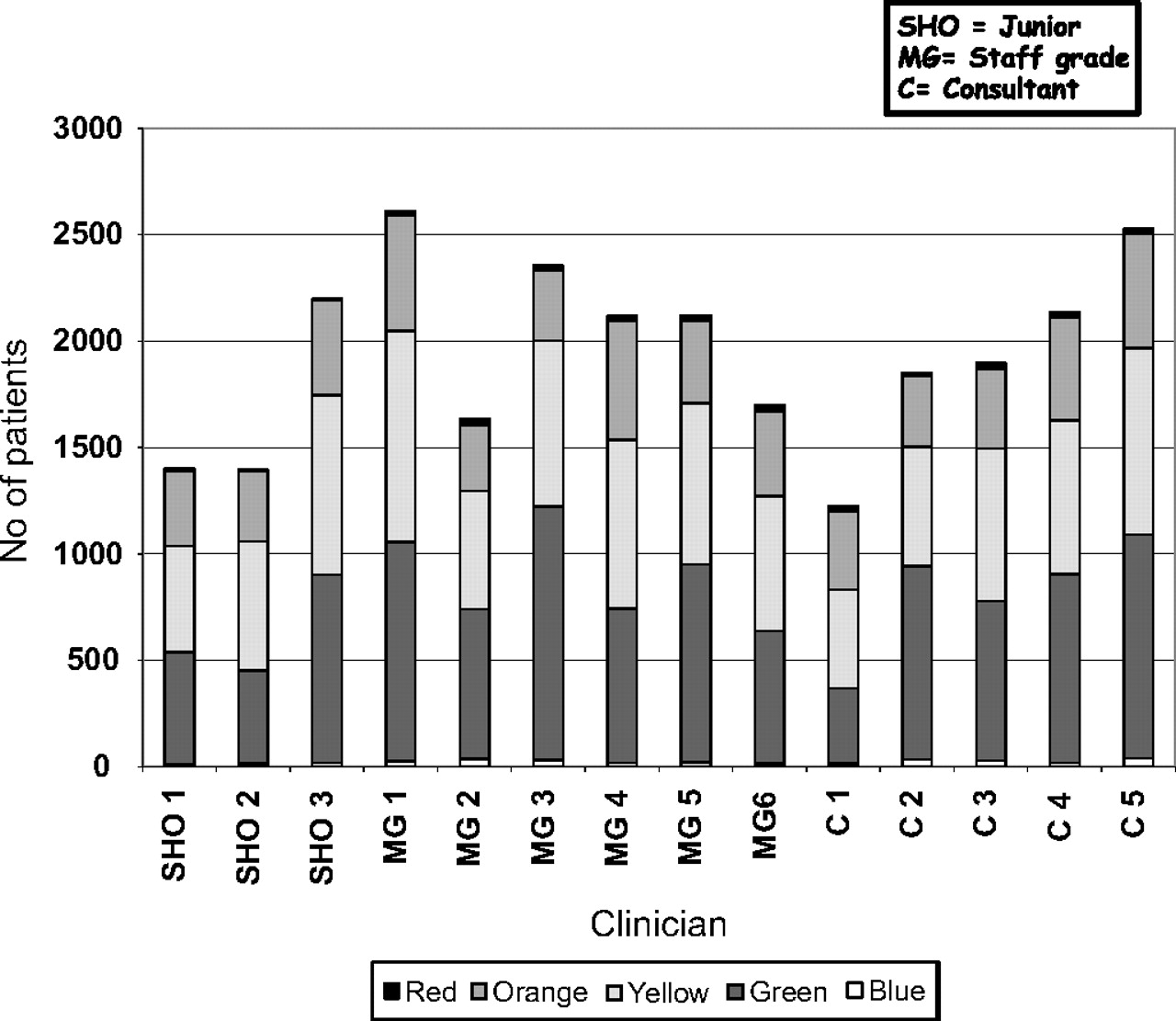
Patients (with triage split) seen by grade of doctor.

Patients admitted (as percentage of patients seen) by grade of doctor.
Night activity shows that the triage profiles of the three types of shifts (consultant, middle grade and SHO) are comparable (table 3) but differ from the overall yearly profile.
Triage profile (percentage) on 3 sets of nights and overall in 2009
We analysed the number of admission, discharge, clinic referral and ‘did not wait’ category patients during the three sets of nights (table 4). This led to a direct comparison of proportions between consultant nights against middle grade and SHO nights (table 5) to show statistically significant difference in favour of consultants against middle grades for ‘did not wait’ category patients (p=0.003) and against SHOs for admission (p=0.026), discharge (p<0.001) and ‘did not wait’ category patients (p<0.001). Although consultants discharged more than middle grades and returned fewer patients to ED clinic than SHO, these were not statistically significant.
Main disposal options for patients on 3 sets of nights
Comparison (χ2) of disposal options between consultant, middle grade and senior house officer (SHO) nights
We also compared the times spent by patients (ED length of stay (LOS)) in the department for each triage category (figure 4). For each comparison, we have shown both the raw and adjusted data for SHO nights. The ED LOS for consultants was shorter than the other two grades for every triage category. This reached statistical significance for Green, Yellow and Orange category patients when compared between consultant versus SHO nights but not for consultant versus middle grade nights (table 6).
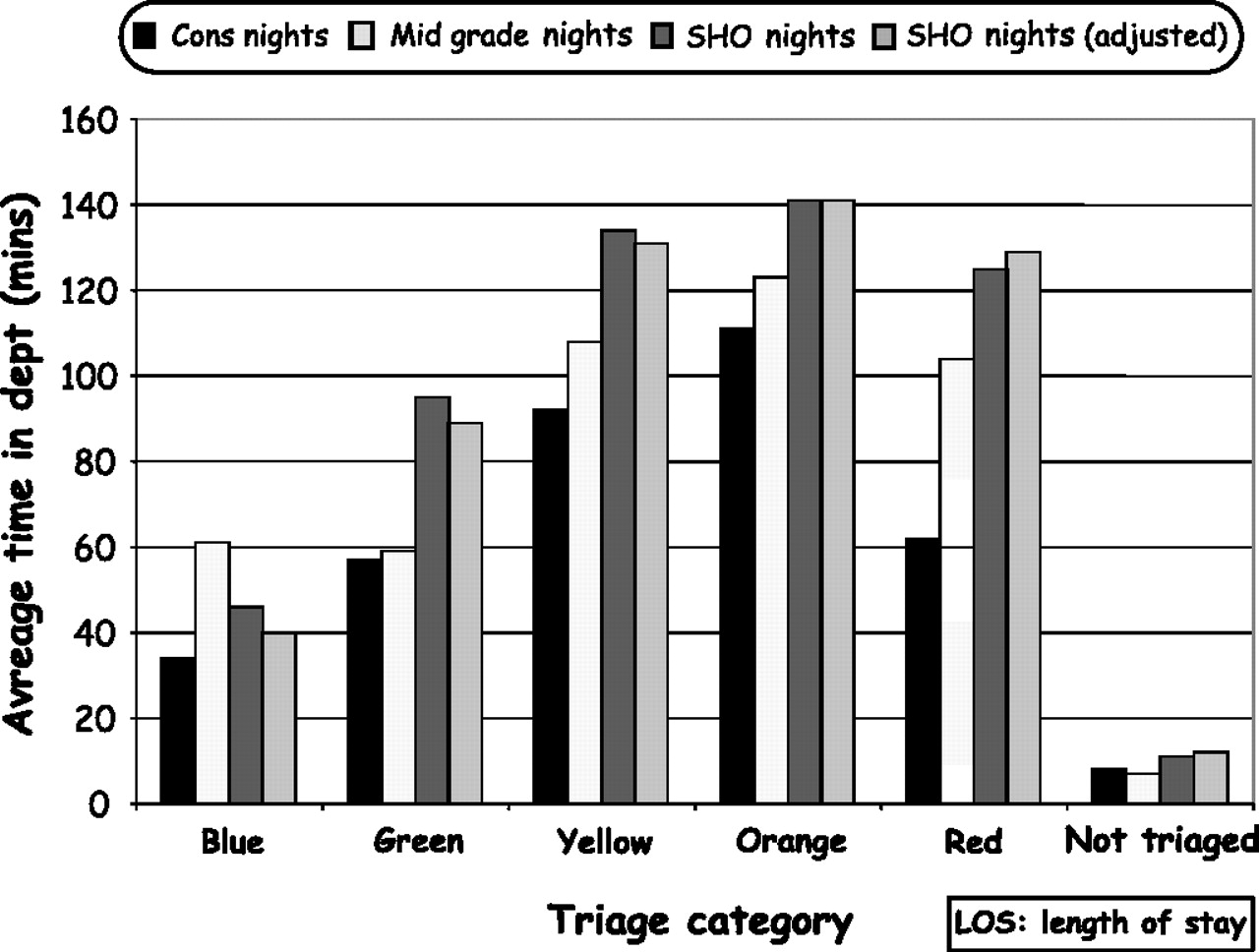
Comparison of mean ED-LOS by triage category.
Comparison of emergency department length of stay for five triage category patients on three sets of nights
The final analysis shows the patient processing times (from registration to departure from ED) on three categories of night shifts in 30 min time bands (figure 5), to show that patients are processed significantly faster during consultant night shifts.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of activity by time band.
Discussion
Wrexham Maelor is a district general hospital, which receives unrestricted emergencies. The ED consultants have engaged in service delivery since 1996. In a clear departure from the traditional supervisory model of consultant activity of that time, we embarked on partial shift (days, evenings and weekends) working since 2003 with a three consultant team. The senior-most consultant (retired in 2008) was not rostered for any unsocial hours work.
The benefits of consultant delivered service do apply equally round the clock. Our current workforce has precluded this 24/7 working. The qualitative impact (safer procedures, better communication and risk reduction) of EM consultant working is perhaps of more value to patients and employing trusts, but is difficult to prove from a retrospective study. This paper provides some evidence of the quantifiable benefits.
As our workload and the clinical needs of our patients have increased, we have shifted the bias towards a senior delivered service (table 1) and increased its efficiency by reduced admissions, clinic returns, re-attender rates and ED LOS (figures 1 and 4). Today, the senior doctors (consultants and middle grades) outnumber the juniors (13 vs eight), in contrast to the 2007 survey1 where most UK departments were junior heavy and perhaps still are. Both grades of seniors carry a workload higher than suggested by the College of Emergency Medicine (1500 patients/year for a consultant and 2000/year for middle grades) for a medium sized ED.3 This is in addition to the usual duties of supervision, vetting decisions, teaching/assessing and administration. The consultants' own workload and admission rates vary (figures 2 and 3), but still result in an overall low admission rate, which has steadily fallen over the last 7 years (table 1). We believe this is due to the overall impact of their presence at extended hours and superior decision making rather than individual workload. In this context, triangulation with the other two North Wales ED provides useful controls (table 2) to show significantly lower admission rates at Wrexham ED (p<0.001). Those two departments continue to depend on a junior delivered service, while their casemix, clinical dependency and patients' age distribution are very similar to Wrexham. Another efficiency benefit of consultant working maybe seen in our department's superior 4-h target performance of average 95.5% (2009), which has helped Wrexham top the Welsh performance table.5 However 4-h performance may be influenced by other variables and cannot be taken as a reliable proof of senior working, while low clinic returns might. Both our ED clinic returns and reattender rates have steadily fallen since 2005 (figure 1). There is paucity of similar data in the UK emergency medicine literature. White et al6 measured the impact of mandatory senior review on junior doctors' decision making to show an 11.9% reduction in admission, 9.4% reduction in inappropriate discharge and a 34.6% rise in outpatient referrals. Presumably, the seniors there make a positive impact on the service delivery by their presence like us. This is in contrast to the past EM consultant working model in UK, which in one study involved 30% clinical contact time (range 15–48%) and the rest distributed among teaching and administration.2 We spend our clinical sessions largely on service delivery and supervision. We restrict our administrative duties to one session. Besides, by being clinically active, we maintain our skills adequately so that we can provide appropriate clinical supervision7 and set the standards needed for patient safety.8
We embarked on night shift working in 2008 in response to many near miss events, ED backlogs and ambulance waits during night shifts manned by two SHOs after midnight. These were not helped by being on-call as consultant presence is superior to opinions. Opinions were not sought promptly or not at all despite an obvious need. This is in contrast to the model of Jaye et al9
The SHO pool was reduced to increase the middle grade tier. This decision was based on our experience, echoed by Armstrong et al,10 of decreasing junior and increasing senior workload, as well as an anticipated quality benefit. This benefit has led to recent consultant expansion. While it is logistically possible to run a 24/7 middle grade rota with eight doctors,3 we felt this was unsustainable. Because, seven of our eight middle grades are permanent SAS doctors (of excellent calibre), who would age at the same rate as us, would soon feel the physical pressures of frequent (one in eight) and long (12 h) night shifts and get disenfranchised. We felt that a shared pool of night rota, with five consultants and eight middle grades working three nights on a one in 13 frequency was the only sustainable solution. Consultant night working is now well established in Wrexham. In fact, the consultants feel that nights are quieter, provide more clinical challenge (table 3) and less distraction. We are soon due to cover four nights (with 3.5 Whole Time Equivalent new consultants); aiming for full shift working once the senior pool size reaches 20. With the current lack of middle grades, this will certainly mean consultant expansion. Consultant numbers in Wrexham, duly costed, should show good service returns for the investment. Our next study may show that savings from low hospital admission rates alone would more than pay for the additional consultants, a principle already accepted by the Betsi Cadwaladr University Health Board.
However, data from the night shifts allowed us to contrast consultant working against the middle grades and SHOs, with another SHO being constant. Our data shows that night shifts are quieter, have less minor/ambulatory patients and more with higher clinical dependency (table 3), which are mostly medical emergencies. Weekend nights (SHO only) are marginally busier but bring no greater clinical challenge.
On comparison (tables 4 and 5), it is clear that while admission rates are slightly lower than SHO nights, consultants discharge more patients without any follow-up, return fewer to ED clinic and have fewer leaving without treatment (patients did not wait). We feel that the narrow difference of admission rates (between three grades) at night shifts is due to inherently more ill patients. Despite our individual variable admission rates (figure 3), overall we certainly impact on the hospital admission rate (table 2), unlike the experiences of Goodacre et al.11 This is generic of consultant working and shop floor presence regardless of individual performances.
The efficiency of consultants' service is stark when time in the department (ED LOS) is compared for patients in each triage category (figure 4). This was shortest for the more critical patients in Priority 1, 2 and 3 (major trauma, airway compromise, sepsis, etc). In this aspect, the consultants out-performed the middle grades—presumably due to superior experience and decision making skills. While the shorter LOS for consultant shifts (in contrast to middle grade and SHO shifts) were clinically very significant in the higher triage categories, this was not statistically significant due to small sample size (table 6). For red (Priority 1) category patients, the mean ED mean LOS was 61.5 min for consultants, 104 min for middle grades and 129 min for SHO shifts. As this was not statistically significant, we did a retrospective power and sample size calculation. In order to show 5% significance (p=0.05) with 80% power to detect, the sample size needs to be 46 Priority 1 patients (actual 14) for SHO and 20 (actual four) for middle grade comparison. Overall, the consultant shifts showed a statistically significant reduction in LOS over the SHO shifts for Priority 2, 3 and 4 patients (table 6). The departmental night diary reflects this effect. A recent Australian study12 has shown similar LOS advantage of ENPs (Emergency Nurse Practitioners) and senior doctors over junior medical staff in their fast track section (ie, UK equivalent of ‘see and treat’) of their ED.
The same data from night shifts, when translated to 4 h performance targets and time bands to process patients completely (figure 5), show why a junior delivered service is unlikely to comply with timeliness of care. In the current climate of ED overcrowding and reducing inpatient beds, this model is not helpful.
This study won't show the ultimate benefits to patient care as consultant service impacts on quality of care and communication, and patient safety. The other beneficiary of consultant presence is our trainees. At night, our juniors and specialty juniors have a consultant to ratify their decisions and assist with interventions—non-invasive ventilation, sedation, and so on. The confidence from these nights has empowered our juniors to work the unsupervised nights with less trepidation.
We provide quantifiable evidence of our conviction that EM service needs to be based on consultants. The quality benefits are equally persuasive. We lament that this practice is not widespread in the UK. The College of Emergency Medicine is now actively promoting this model and lobbying for consultant expansion. We would urge our UK colleagues to engage. We assure them that it is sustainable, given enough numbers. If we practice to our professed clinical standards, we shall enhance the credibility of our specialty. We promise that life on full shift 24/7 is much better than being on call after a busy day.13
Conclusion
Since 2003, the Wrexham ED consultants have delivered service, including night shifts since 2008. We have provided quantifiable evidence of the benefits of this model. Low admission rates compared to other departments offering a junior based service is one of them. On comparing consultant working against SHO and middle grade doctors, there is similar evidence of efficiency. Evidence of quality benefit of this model can be obtained.8
We recommend that this model be adopted widely, including by the emergency care planners, so that necessary consultant expansion is urgently funded to make this sustainable. We would rather be treated by an EM consultant ourselves—our patients deserve no less.
Acknowledgments
We are very grateful to Dr J Turner, PhD Senior Research Fellow, Department of Audit and Research, Wrexham Maelor Hospital (turnerj{at}cardiff.ac.uk) for his help with the statistical analysis of the data. We also thank our department secretaries for collating the medical staff rotas so that the activity could be analysed.
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Primary survey