Article Text

Abstract
Objectives & Background Emergency department (ED) procedural sedation is becoming more common, but associated adverse events have been reported. The Royal Colleges of Anaesthetists and of Emergency Medicine (RCoA and RCEM) have produced guidelines on the sedation of adults in the ED (RCoA and RCEM, 2012).
In other environments checklists have been shown to improve patient safety (WHO, 2016).
We hypothesised that introduction of a checklist would increase compliance with sedation guidelines
Methods In an East London ED, compliance with the RCoA/RCEM sedation guidelines was audited retrospectively from January to December 2015. On 1st June 2015 a sedation checklist was introduced.
98 patients were identified from electronic patient records and data was compared between 3 groups:
▸ Patients sedated before 1st June 2015 (PreCheck): n=44
▸ Patients sedated after 1st June 2015, on whom the checklist was used (PosCheckPos): n=28
▸ Patients sedated after 1st June 2015, on whom the checklist was not used (PosCheckNeg): n=26
Results Demographic data was similar between all the groups with no significant differences in age distribution, procedure, sedating agent, number of drugs used, the grade of the sedationist, discharge destination, or the proportion of sedations done out of hours.
No significant adverse events occurred in any of the groups.
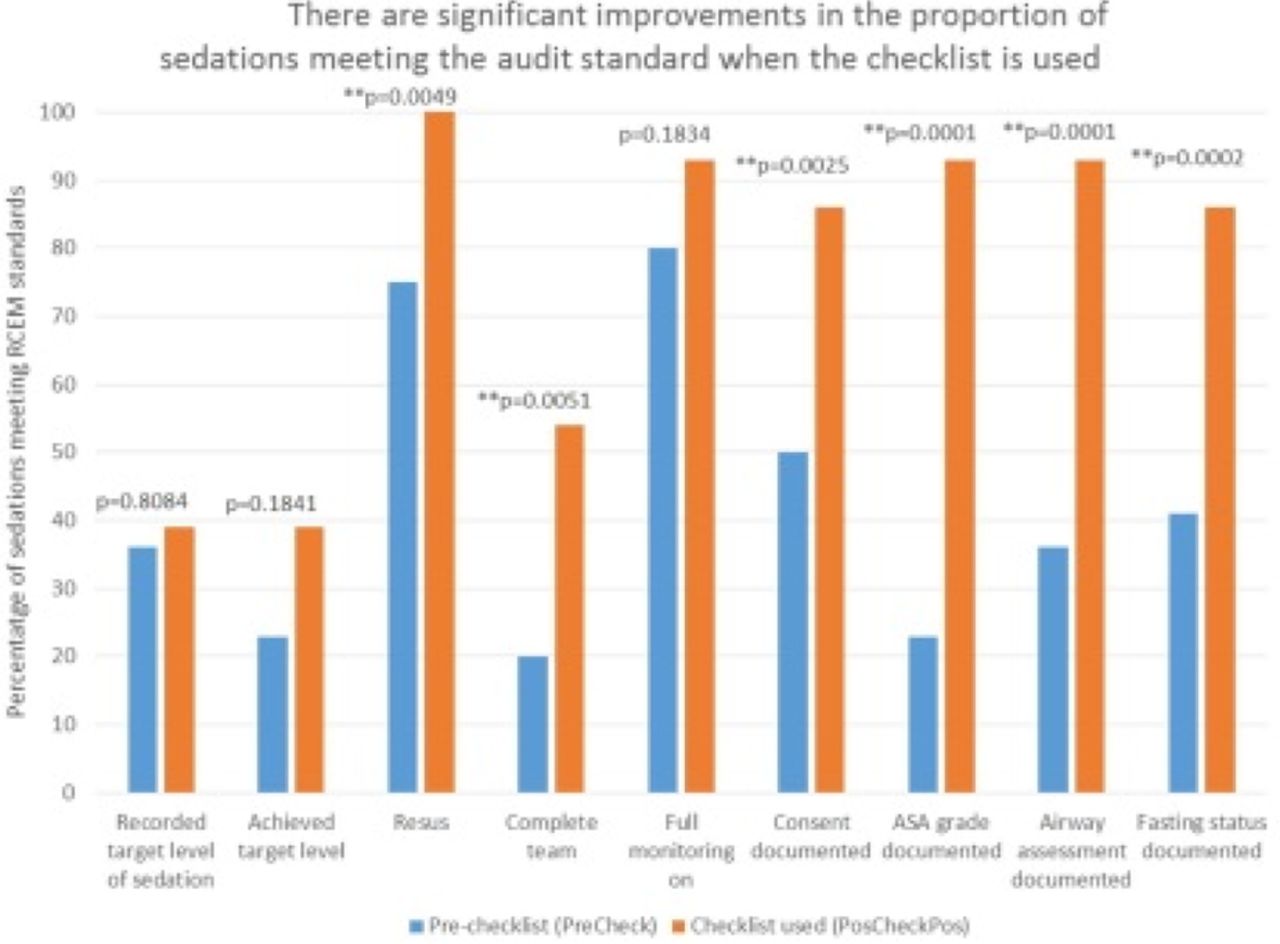
When the checklist was used, 61% of sedations met all of the criteria for a safe sedation (ASA grading; airway assessment; fasting status and consent documented; two doctors and full monitoring). Prior to the checklist, 18% of sedations met all of the criteria.
When the checklist was used (figure 1) there was a significant improvement in the number of cases meeting the audit standard for documentation of: consent, location, staffing, fasting status, ASA grade and airway assessment.
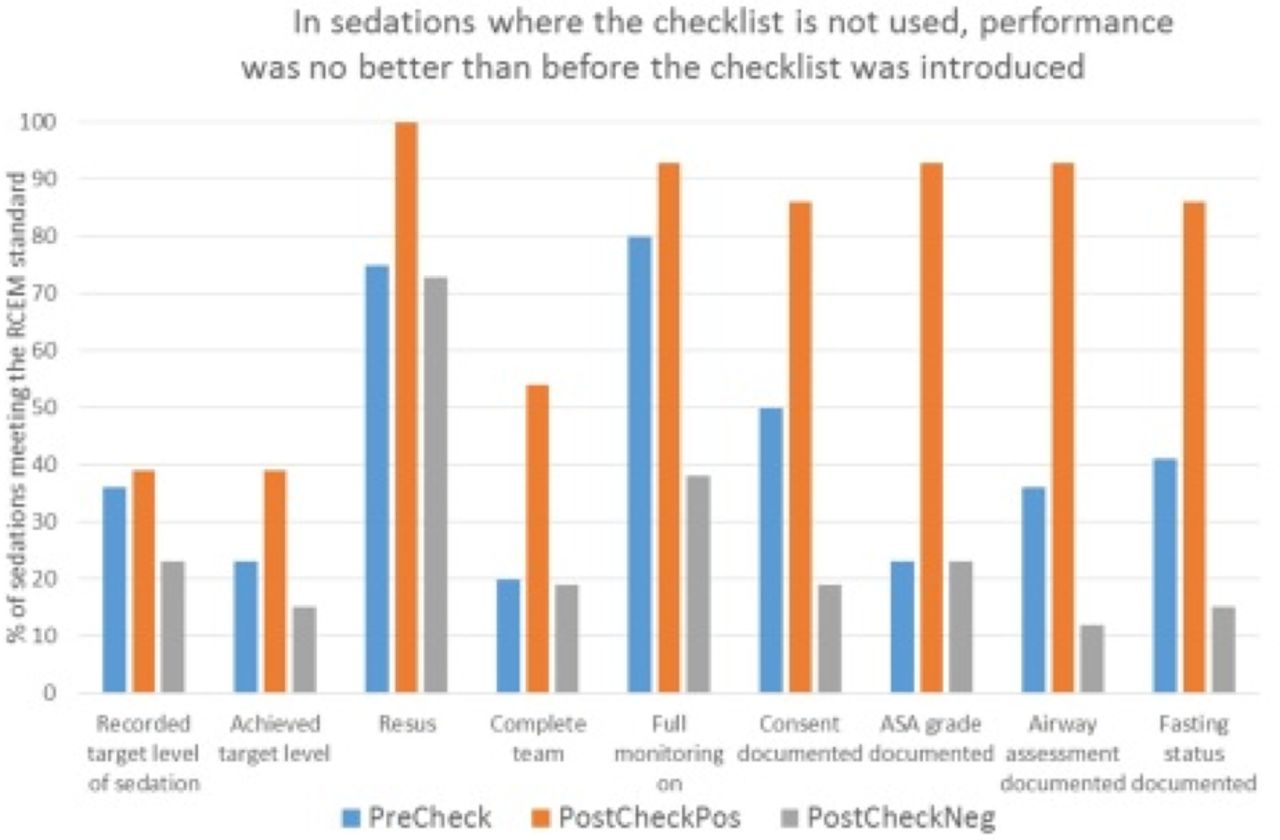
When the checklist was not used despite being available, performance was no better than before the checklist was introduced (figure 2).
Conclusion The sedation checklist improved standards when used, but did not improve the performance of the ED overall because those who forget the existence of the checklist seem prone to forget to document the key steps in safe sedation.
To increase compliance with RCoA and RCEM sedation guidelines the checklist needs to be a compulsory part of the set up for sedation, linked with the dispensing of sedation drugs.⇓ ⇓
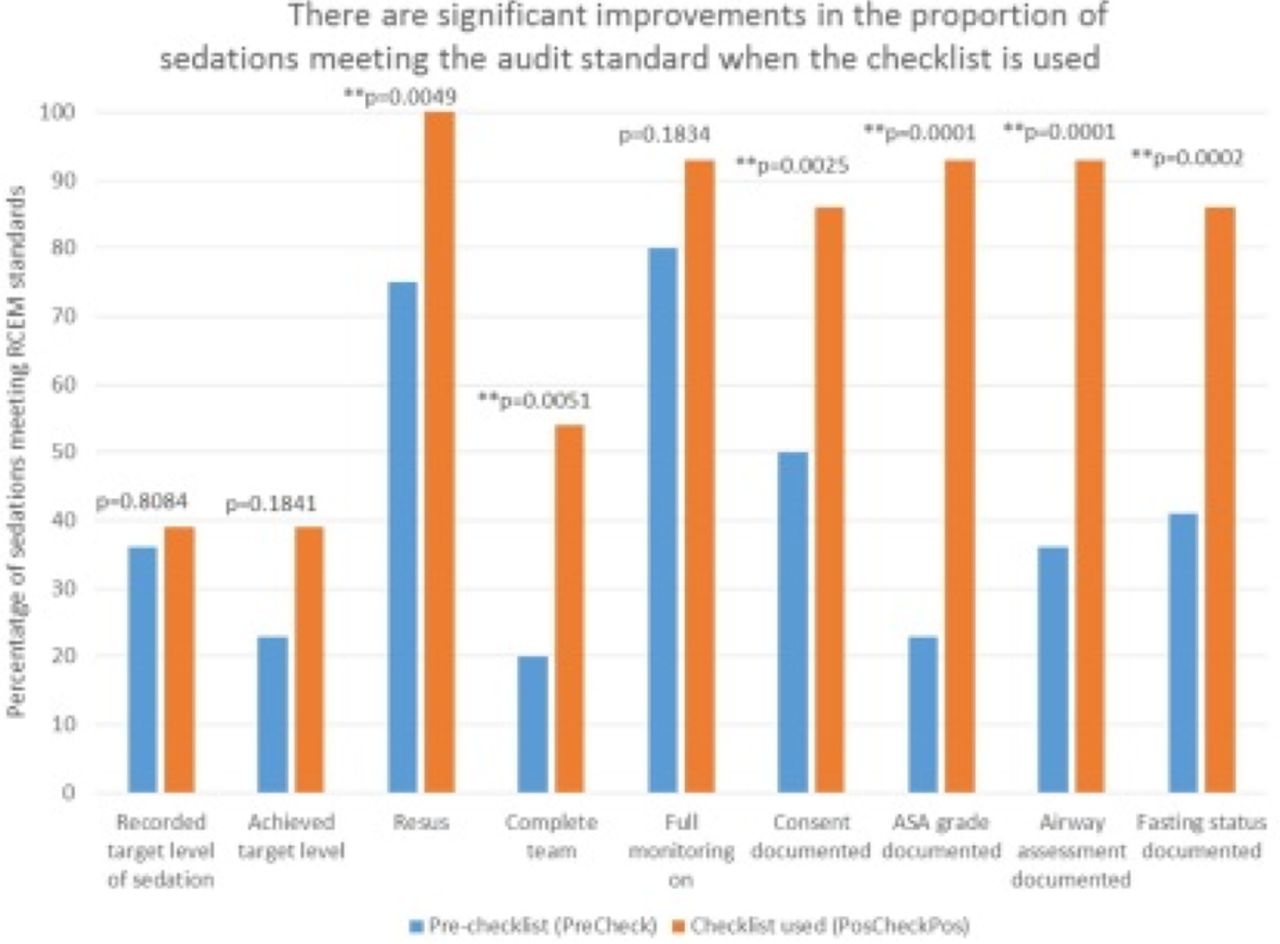
There are significant improvements in the proportion of sedations meeting the audit standards when a checklist is used
{kind=link}
{kind=link}
When the checklist is not used, performance is no better than before it was introduced
- Trauma