Article Text

Abstract
Background Evaluating the quality of life of young adult survivors of out-of-hospital cardiac arrest (OHCA) is important as they are likely to have a longer life expectancy than older patients. The aim of this study was to assess their functional and quality of life outcomes.
Methodology The Victorian Ambulance Cardiac Arrest Registry records were used to identify survivors of OHCA that occurred between 2003 and 2008 in the 18-39 year-old age group. Survivors were administered a telephone questionnaire using Short Form (SF-12), EQ-5D and Glasgow Outcome Scale-Extended. Cerebral Performance Category (CPC) ascertained at hospital discharge from the medical record was recorded for the uncontactable survivors.
Results Of the 106 young adult survivors, five died in the intervening years and 45 were not contactable or refused. CPC scores were obtained for 37 (74%) of those who did not take part in telephone follow-up, and 7 (19%) of these had a CPC ≥3 indicating severe cerebral disability. The median follow-up time was 5 years (range 2.7- 8.6 years) for the 56 (53%) patients included. Of these, 84% were living at home independently, 68% had returned to work, and only 11% reported marked or severe disability. The majority of patients had no problems with mobility (75%), personal care (75%), usual activities (66%) or pain/discomfort (71%). However, 61% of respondents reported either moderate (48%) or severe (13%) anxiety.
Conclusions The majority of survivors have good functional and quality of life outcomes. Telephone follow-up is feasible in the young adult survivors of cardiac arrest; loss to follow-up is common.
- Cardiac arrest
- resuscitation
- quality of life
- outcomes
- EMS
Statistics from Altmetric.com
Introduction
Cardiopulmonary resuscitation has the aim of returning patients to independent living. Therefore, although survival at hospital discharge is a key measure of resuscitation success, intact functional status may be more important. Health-related quality of life refers to the physical, psychological and social aspects of health as seen in domains that are influenced by a person's experiences, beliefs, expectations and perceptions.1 ,2 Previous studies have reported that half of survivors of out-of-hospital cardiac arrest (OHCA) have permanent brain damage of varying degrees.3 ,4 However, a recent systematic review of quality of life after cardiac arrest found studies reported good quality of life after cardiac arrest survival.5
There is remarkable heterogeneity of methodology among studies assessing functional and/or quality of life in cardiac arrest survivors and there is no consensus regarding the preferred tools or the best timing of assessment.5 The Cerebral Performance Category (CPC) score,6 though not well validated, has been recommended as part of the Utstein guidelines for reporting cardiac arrest outcomes7 and is widely used by investigators.6 ,7 It is designed to indicate overall functional status of cardiac arrest survivors but does not measure differences among survivors who have high cerebral function8 or their quality of life. It has the advantage of being simple to use and a score at hospital discharge can usually be ascertained from the hospital records.
Young adults represent a minority of those who suffer an OHCA.9 The functional and quality of life outcomes in this group are particularly important as they are likely to have a longer life expectancy than older patients who sustain OHCA. Also, the aetiology of cardiac arrest may be different in young adults. For example, overdose associated OHCA features are more frequent than ischaemic heart disease as seen in older age groups.9 ,10 On the other hand, there are challenges associated with following up this age group who often change contact details, are more mobile and may be less facilitative of follow-up. Previous publications have not focused on functional and quality of life outcomes in this age group. This paper describes the functional and quality of life outcomes in young adults who survive OHCA.
Methods
Patients
Survivors of all OHCAs aged 18–39 years and attended by Ambulance Victoria in metropolitan Melbourne between 1 January 2003 and 31 December 2008 were included.
Setting
Melbourne is the capital city of the state of Victoria in Australia. At the time of the last census (2006), Melbourne's population was 3.59 million, of whom 1.19 million were aged between 18 and 39 years of age with an equal male to female distribution.11
Emergency medical services
In Melbourne, the Advanced Medical Priority Dispatch System© is used to receive emergency calls and Ambulance Victoria is the sole provider of emergency medical services (EMS). The EMS comprises ambulance paramedics who have some advanced life support skills (laryngeal mask airway, intravenous epinephrine) and mobile intensive care ambulance paramedics who are authorised to perform endotracheal intubation and administer a wider range of cardiac drugs. Mobile intensive care ambulance paramedics are dispatched to patients with critical illness, including patients with cardiac arrest. In addition, fire-fighter first-responders are dispatched to patients with suspected cardiac arrest in the inner two-thirds of Melbourne.12 The prehospital cardiac arrest protocols follow the recommendations of the Australian Resuscitation Council.13 ,14 Ambulance Victoria paramedics are not obliged to commence resuscitation when the presenting features are inconsistent with resuscitation. This includes decapitation, presence of rigour mortis, decomposition or postmortem lividity, where death has been declared by a Medical Officer who is or has been at the scene and where the presenting rhythm was monitored as asystole for >30 s, and there has been >10 min downtime with no evidence of hypothermia, drug overdose or family/bystander objections. Paramedics may discontinue resuscitation in the field if advanced life support has been performed for 30 min without return of spontaneous circulation, the rhythm is not ventricular fibrillation or ventricular tachycardia, there are no signs of life, no gasps or evidence of pupillary reaction and no evidence of hypothermia or drug overdose.13
Victoria Ambulance Cardiac Arrest Registry
The Victoria Ambulance Cardiac Arrest Registry (VACAR) is a population-based registry containing Utstein and additional outcome data for all EMS attended OHCAs occurring in the Australian state of Victoria since 1999.15 Paramedics attending OHCA enter clinical data into a laptop computer at the conclusion of the case. The VACAR data are extracted from this electronic patient record into a purpose built database. Data collection is standardised and quality controlled. Survival to hospital discharge in VACAR is obtained from all treating hospitals (n∼100). Since January 2011, VACAR has prospectively collected functional and quality of life outcomes data at 12-months postarrest.
For the purpose of this study, retrospective QOL data were captured for young adult patients who had OHCA from 2003 to 2008. Hospital investigation results were not recorded in VACAR for the time period involved in this study. EMS response time is the time from emergency call to EMS arrival at scene. VACAR was used to identify young adults aged between 18 through 39 years who had sustained OHCAs between 2003 and 2008 and who had been discharged alive from hospital.
Ethics approval and consent
VACAR has been classified as a quality assurance project by the ethics committee at the Department of Health. The collection of cardiac arrest outcome data by VACAR was approved by the ethics committees of all Victorian hospitals receiving cardiac arrests by ambulance. This study was approved by Monash University's Human Research Ethics Committee. Young adult survivors were sent a letter approximately 1 month in advance of receiving the telephone follow-up in which the reason for the study was explained. An option was offered to opt-out of the study and telephone, email and postal contact details were included.
Instruments
We adopted the functional and quality of life outcomes assessment tools used by the Victorian State Trauma Registry; these are administered by telephone.16 None of the instruments selected require specific qualifications, certification or training by the instrument supplier or by the copyright holder. The full patient interview includes the following data collection:
-
Prearrest demographics, including the highest level of education achieved, occupation and employment status.
-
Work-related disability, including whether the patient returned to the same employer and the same role.
-
Residential or living status and whether additional support services are required.
-
Glasgow Outcome Scale-Extended (GOS-E) which provides a global measure of function on a scale from death to upper good recovery. Important domains such as self-care, mobility in the community, return to work, relationships, social activities and leisure activities are considered.17 ,18 Global measures of disability were recorded in the week before the 5 OHCA and in the week of the telephone interview are recorded.
-
The EQ-5D which is a self-reporting questionnaire validated to measure the quality of life in health-related research19 ,20 has been found to correlate with Short Form 36 (SF-36) and Health Utility Index version 3 scores in a variety of populations.21 ,22 In addition, this may be used to calculate ‘quality adjusted life years’ and has been used in general critical illness survivors23 ,24 and cardiac arrest outcomes reporting.25 ,26
-
The Short Form 12 (SF-12) provides a measure of the physical and mental health status and is used widely in the literature. It can be administered by telephone, is quick to administer and there are Australian population norms for comparison. The SF-12 encompasses eight domains: physical functioning, social functioning, mental health, role limitations due to physical problems, role limitations due to emotional problems, vitality (energy and fatigue), bodily pain and general health perceptions. While the more detailed SF-36 from which the SF-12 has been derived has been used previously in cardiac arrest outcomes reporting27−29 the SF-12 has not. A SF-12 Physical Component Summary Score or Mental Component Summary Score ≤40 represents moderate to severe disability.
-
For cases where it was not possible to apply the telephone questionnaire, a CPC at hospital discharge was derived from the hospital chart. A CPC score of 1 was given if the patient is conscious, alert, able to work, though might have a mild neurological or psychological deficit. CPC 2 is given if there was moderate cerebral disability: the patient is conscious, has sufficient cerebral function for independent activities of daily life and able to work in a sheltered environment. CPC 3 describes severe cerebral disability: the patient is conscious and dependent on others for daily support because of impaired brain function; this ranges from an ambulatory state to severe dementia or paralysis. CPC 4 describes a patient who is comatose without the presence of brain death criteria. CPC 5 describes brain death, apnoea, areflexia, ECG silence, etc.
Mode of administration of telephone interview
For survivors at hospital discharge, the Victorian Registry of Births Deaths and Marriages was cross checked to ascertain whether the patient had died in the interim period. Ambulance accounts records, the Victorian telephone directory and the hospital medical record were used to establish the address and contact details for the patient. Four attempts, at different times of the day, were made to contact patients over a month-long period. The interviewer had clinical experience and could appreciate the clinical scenarios and issues, provide information about services and deal with the distressed or dissatisfied patient. An algorithm for dealing with the distressed participant was required for ethics committee approval. Interviews were performed from a central location, rather than from individual health services ensuring quality control, interviewer trouble shooting and debriefing.
Statistical analysis
All data were entered into an Access database (Version 2003, Microsoft, Redmond, Washington, USA). Statistical calculations were performed on STATA software (V.10.0 Stata Corporation). χ2 Analyses were used for categorical variables. Continuous variables were compared using the t test (normal distribution) or Mann–Whitney. We adjusted SF-12 for Australian norms and present results as mean with SD. Multivariate logistic regression analysis was performed to examine Utstein elements associated with good neurological outcome; a good neurological outcome was defined as CPC 1 or 2 or GOS-E ≥5 and represents independent living.
Results
During the study period, there were 2361 OHCAs in young adults of whom 928 (39%) had an attempted EMS resuscitation, and 106 (9%) were alive at hospital discharge. When linked with the Victorian Registry of Births Deaths and Marriages, it was found that 5 (5%) patients had died in the intervening time since discharge from hospital. Of the remaining 101 patients, 56 (55%) were successfully contacted and undertook the telephone follow-up questionnaire. The family of two patients asked not to be contacted after the receipt of the information letter; however, they did not object to the hospital notes being used to ascertain the CPC. Both had poor functional outcomes. Three patients on being telephoned refused to take part in the telephone survey; they did not object to their CPC being ascertained from the hospital record. The CPC score was ascertained from the hospital records in 37 (37%) patients. The CPC could not be determined from the hospital notes for one patient. Seven patients who could not be contacted also had hospital records that were unable to be examined. The median follow-up time was 5 years (range 2.7–8.6 years).
Table 1 shows the characteristics of young adult survivors and the types of cardiac arrests they sustained. There were 14 patients with a presenting rhythm of asystole who survived to leave hospital; three patients had telephone follow-up, seven patients had their CPC ascertained from the chart and four patients were untraceable. Of these patients, eight were found to have a good outcome defined as CPC 1 or 2 or GOS-E ≥5.
Characteristics of the 106 young adult OHCA survivors (18–39 years of age) in metropolitan Melbourne between 1 January 2003 and 31 December 2008
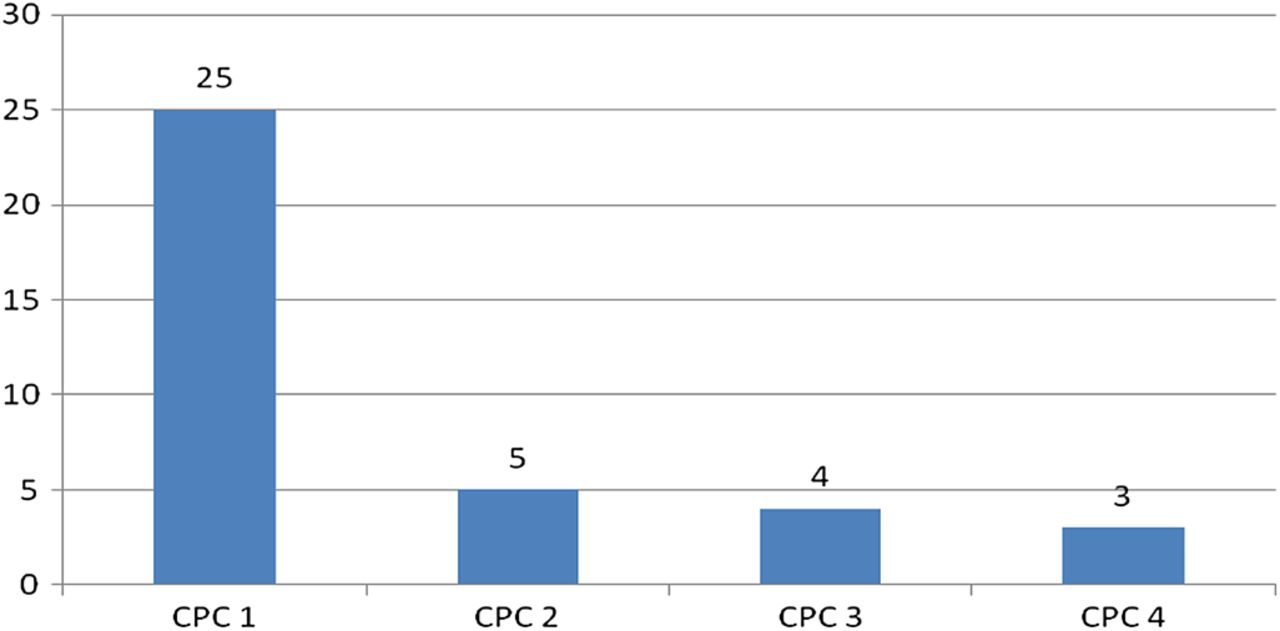
Figures 1 and 2 display the Global Outcome Assessment and Global Outcome Score-Extended for patients who underwent telephone follow-up. Figure 3 shows the CPC results for those patients not contactable by telephone. Overall, six of 56 (11%) patients in the telephone follow-up group had a marked or severe disability while 7 (19%) of the non-contactable group (n=37) had a CPC >3 on leaving hospital.
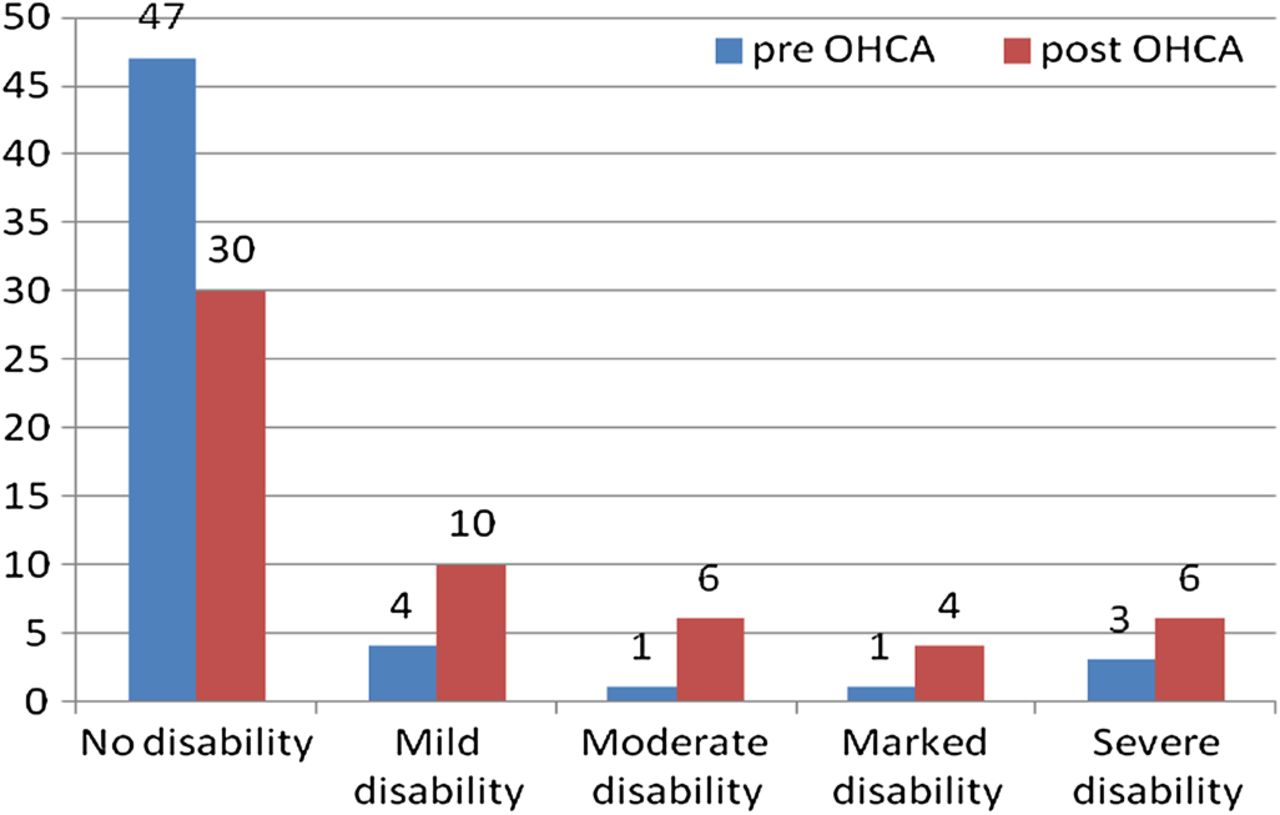
Global Outcome Assessment (n=56). OHCA, out-of-hospital cardiac arrest.

Global Outcome Score-Extended (n=56).

{kind=link}
{kind=link}
{kind=link}
Cerebral Performance Category (CPC) score on patients not contactable by telephone (n=37).
Table 2 details the demographics GOS-E and the EQ-5D results of the 56 patients who received telephone follow-up. Prior to their cardiac arrest, 47 (84%) were working or studying; 32 (68%) returned to work after their cardiac arrest, with 22 (47%) to the same role. The majority of survivors (84%) were living independently at the time of follow-up. The majority of patients reported having no problems with mobility (75%), personal care (75%) and pain or discomfort (71%). However, a third of patients reported problems with usual activities, and 61% reported either moderate (48%) or severe (13%) anxiety post-OHCA.
Telephone follow-up successful (n=56); demographics, Glasgow Outcome Score-Extended and EQ-5D results
The SF-12 was completed by 46 patients (table 3). The majority (78%) of these patients described their health as good or better, with 52% answering that their physical health did not limit them in their physical activities. Only 28% described having a lot of energy either ‘a little of the time’ or ‘none of the time’ and 41% described feeling down hearted and blue at least some of the time. In this study, the mean (SD) physical score was 46.5 (10) and the mean (SD) mental score was 38 (14.5) adjusted for Australian norms.
Short Form (SF) 12 results (46 patients completed this questionnaire)
Table 4 details the multivariable logistic regression analysis examining factors associated with a good functional outcome. Ventricular fibrillation was shown to be associated with a good functional outcome in this group of survivors; however, the numbers in this study were small.
ORs for the association between selected Utstein elements and good survival outcome defined as CPC 1–2 or GOS-E ≥5 (n=93)*
Discussion
This is the first OHCA study to specifically focus on functional and quality of life outcomes in young adults who survive cardiac arrest. Given their potential for longer life expectancy, these patients would be expected to have additional healthcare costs, in particular if there are poor functional outcomes. This study shows that in fact most young adult patients who survive to leave hospital have a good outcome with 96% living at home at the time of follow-up and 84% living independently.
Comparing with other studies of older age groups, a prospective substudy of the Ontario Pre-hospital Advanced Life Support Study interviewed 305 survivors of OHCA at 12 months for CPC Score and Health Utilities Index score.8 The mean age of survivors was 63.9 years; 88% had a CPC score of 1, 8% a CPC score of 2 and 4% a CPC of 3. The median (IQR) for health utilities index was 0.84 (0.61–0.97). Therefore, most patients with cardiac arrest who survived to hospital discharge had a good quality of life and functional status.
In this study, the mean (SD) physical score was 45.6 (9.45) and the mean (SD) mental score was 38 (14.5) adjusted for Australian norms. An SF-12 Physical Component Summary Score or Mental Component Summary Score ≤40 represents moderate to severe disability.
There are multiple tools used to measure quality of life and functional outcomes after survival from OHCA5; one systematic review found over 50 functional and quality of life outcome measurement tools highlighting the lack of consensus in this area.5 Factors affecting use of any assessment tool include the tool's proven validity, the availability of national norms data for that tool, whether timing of follow-up using the tool introduces variability and whether precardiac arrest health is accounted or adjusted for in postcardiac arrest outcomes assessment. Also relevant is the cost of the tool including training of interviewers, the time required to administer the tool as well as the license fee. Elliott et al 5 in their systematic review of quality of life and other patient-centred outcomes after cardiac arrest survival make specific reference to the Health Utilities Index 3 as being reliable, reproducible and valid in a variety of populations as well as to the advantages of the SF 36 and the EQ-5D. They recommend urgent attention be given to developing a consensus on methods to measure OHCA outcomes in the following areas: health-related quality of life, affective and post-traumatic stress symptoms, cognitive dysfunction and health economics.5 They highlight the need for standardisation of the follow-up and assessment intervals and the need for an appropriate comparator group to contextualise the findings.
The CPC is notable for its simplicity and ease of use being ascertainable from the hospital record but it is a blunt instrument and does not determine major issues such as whether that patient was able to return to work or longer term outcomes. Accurate data are important in this area as it informs treatment decisions and prognostication. It is also important to measure the impact of changes in resuscitation algorithms, therapeutic hypothermia, interventional cardiology and antiarrhythmia interventions, the impact of which may not be captured by survival alone.30
Limitations
This study has a number of limitations. Memory disturbance in survivors of OHCA has been reported in 62%31 in one study and 74%32 in another. However, this is difficult to determine using a telephone interview. The Neurobehavioural Cognitive Status Examination33 used in previous studies is not amenable to being performed by telephone, may take 45 min to perform at the bedside and has a license fee. None of the tools used in our study directly measure memory though some patients did mention it as an issue.
We were only able to complete telephone follow-up on 56 patients (53%). Young adults are a difficult group to follow-up owing to their high likelihood of moving location, particularly given that the follow-up for this study ranged from 2.7 to 8.6 years. Drug overdose and attempted suicide are over-represented in this patient group10 many of whom may be reluctant to discuss the incident later. In some instances, the contact details in the hospital chart were incomplete; this may be because accurate identification of unconscious OHCA patients at the point of entry to the hospital may be uncertain. Also, the SF-12 Health Survey is recommended for large group epidemiological studies (>n=200) where information on the SF-36 Health Survey Summary Scores is required; it cannot be answered by proxy. Nevertheless, because of our staff familiarity with this tool, and the ease of telephone administration, this tool was used notwithstanding the limitations of its use in a smaller study.
Because inhospital data were not collected, the impact of postadmission treatments was not measured in this study.
Conclusions
The majority of young adults who survive cardiac arrest have good functional and quality of life outcomes. While telephone follow-up is feasible in the young adult survivors of cardiac arrest, loss to follow-up is common. The major determinant of good long-term functional recovery was ventricular fibrillation as the initial cardiac rhythm.
Acknowledgments
Marian Lodder, Vanessa Barnes and VACAR staff. Ambulance Victoria paramedics. Paul Jennings, Belinda Gabbe, Ann Sutherland, Ceridwyn Freeman, Department of Epidemiology and Preventive Medicine. Monash University.
References
Footnotes
-
Funding Dr C Deasy was supported by a Monash University overseas PhD student scholarship during this project.
-
Competing interests None.
-
Ethics approval Ethics approval was provided by the Monash University Human Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.