Article Text

Statistics from Altmetric.com
Clinical introduction
A 36-year-old woman with Down's syndrome and spleen hypoplasia presented with a fever of 40°C lasting for 12 h. She had taken 1 mg prednisolone/day for mild graft-versus-host disease after allogeneic stem cell transplantation 4 years previously. Her BP was 91/44 mm Hg, HR 110 beats/min and RR 30 breaths/min. Her heart sound, lung sound and skin appearance were unremarkable. Laboratory findings showed leucocytosis (13.12×109/L) and normal platelet count (269×109/L). She was discharged home, but 16 h after fever onset, experienced cardiopulmonary arrest.
Question
What does the image show?
Henoch−Schönlein purpura
Steroid purpura
Postmortem lividity
Purpura fulminans
Answer: D
DIAGNOSIS: acute infectious purpura fluminans (PF) caused by Streptococcus pneumoniae.
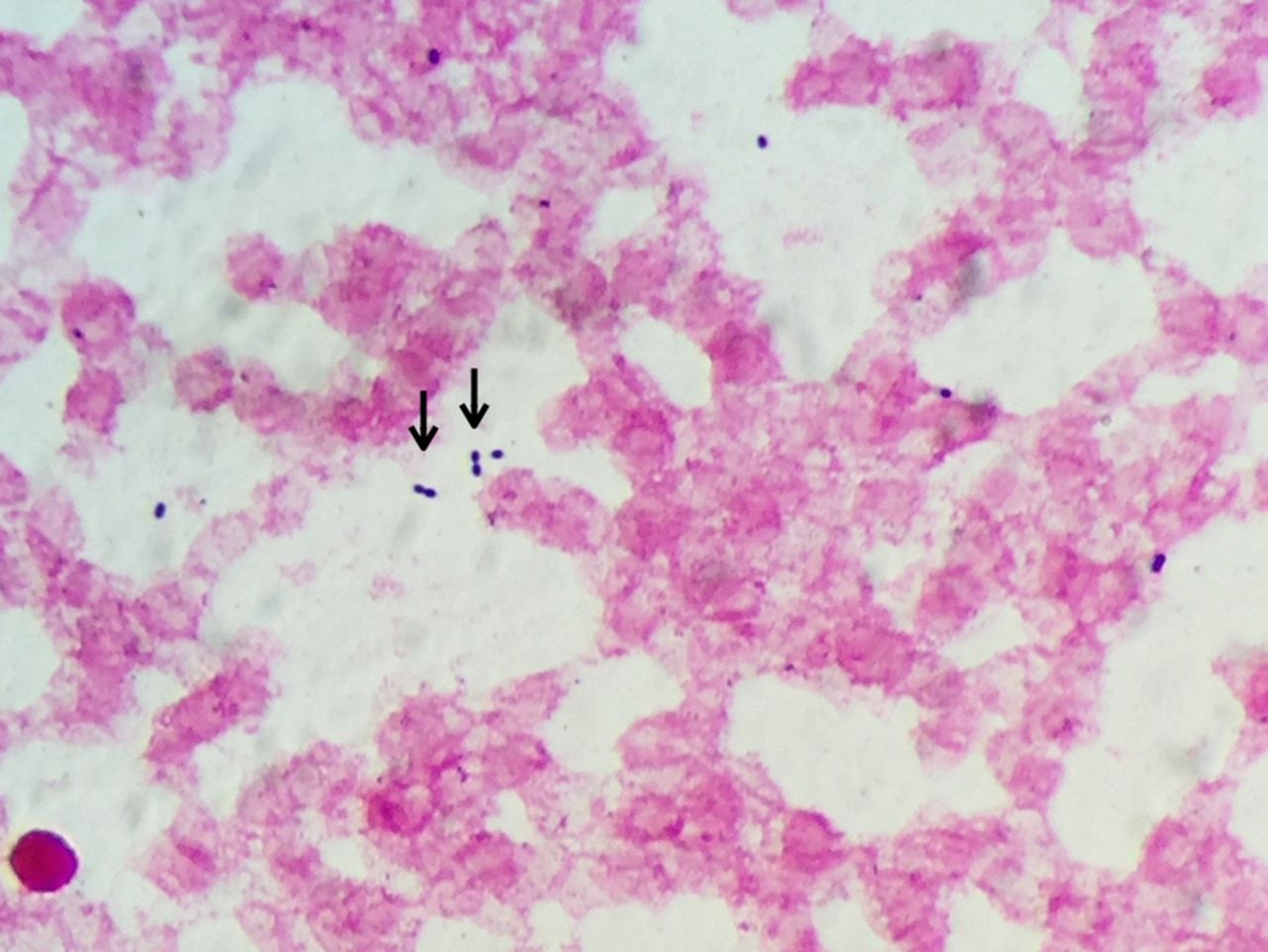
Figure 1 shows systemic impalpable purpura that rapidly emerged on the patient's truncus gravity-independently. Gram staining of her peripheral blood revealed gram-positive diplococci (figure 2, arrows), indicative of acute infectious PF caused by S. pneumoniae. Despite strenuous resuscitation and broad-spectrum antibiotic administration, she died. Her blood culture results subsequently tested positive for S. pneumoniae.

The patient's appearance on readmission.

{kind=link}
{kind=link}
Gram-stained sample of the patient's peripheral blood. The arrows suggest typical gram positive diplococci.
PF is a rare, fatal syndrome accompanied by skin necrosis and disseminated intravascular coagulation, caused by protein C-deficiency or overwhelming sepsis,1 typically caused by Neisseria meningitidis and S. pneumoniae.2 This patient had hyposplenia, a risk factor for invasive N. meningitidis and S. pneumoniae infection.3 Systemic purpura and a rapid, progressive clinical course is indicative of PF, but obtaining blood culture results to confirm infection requires several days. Gram staining of a peripheral blood sample may be useful for identifying causative bacteria, guiding an early decision to use empirical antibiotics.
Henoch–Schönlein purpura is rare and usually benign in adults, and is typically characterised by elevated palpable purpura and abdominal pain. Long-term corticosteroid administration causes steroid purpura, but never causes cardiopulmonary arrest (CPA). Postmortem lividity generally appears 15 h after death; this patient was immediately taken to the hospital upon CPA; therefore, postmortem lividity was not a consideration.
Footnotes
Contributors RT and MO wrote this paper. YT supervised it.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; internally peer reviewed.