Article Text

Abstract
Emergency Medicine requires a highly skilled workforce who are passionate about delivering excellent patient care. Shift patterns linked with the ever increasing numbers of patients who attend Emergency Departments puts strain on educating the workforce and fostering team togetherness.
Our objective in devising and instigating the ‘Mini Sim’ programme was to embed regular in-situ simulation training to enhance the learning of all staff within our Emergency Department team, building a highly trained workforce to deliver excellent care within the remit of our busy department. The whole team is involved including junior nurses, senior nurses and all tiers of junior doctors including foundation, general practice and senior ED trainees (including Grid).
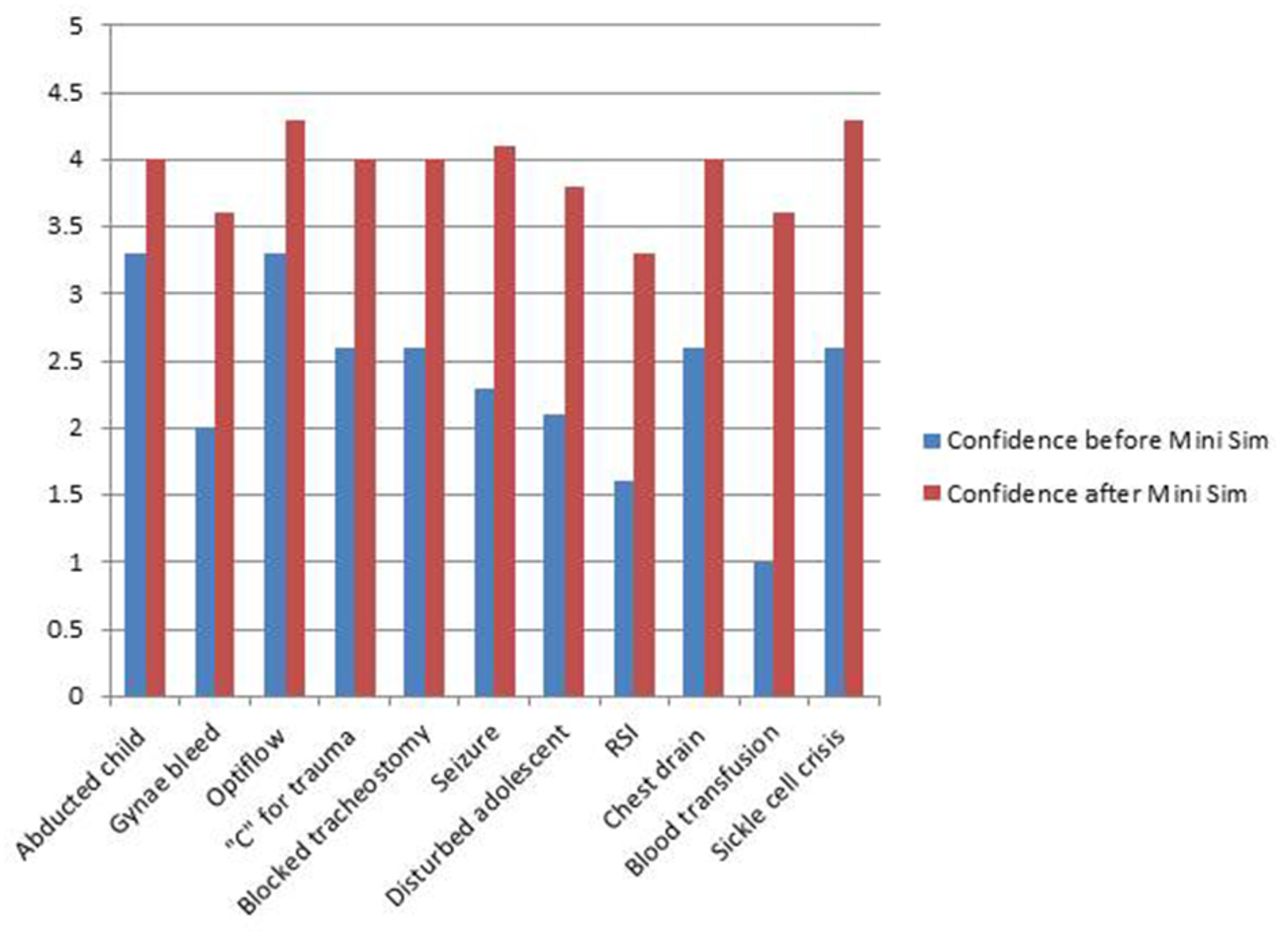
‘Mini Sim’ takes place on a weekly basis, every Tuesday morning from 0930–1000. This timing is to ensure maximum participation from all staff. The setup is a fifteen minute simulation (one nurse, one junior doctor, one senior doctor) followed by fifteen minutes of debrief. The format includes an assessment of the participants confidence prior to ‘Mini Sim’ in the subject being practiced. This is rated on a numerical scale from 1 (being not confident at all) to 5 (being completely confident). The topics chosen are based on feedback from trainees and nurses on clinical skills they feel under confident in, (e.g., pelvic binder application, rapid sequence induction, sickle cell crisis), clinical incidents which have occurred around the Trust (e.g., seizures and access to benzodiazepines), National Patient Safety Alerts (e.g., phenytoin toxicity), protocols (e.g., abducted child, rapid tranquilisation for the acutely disturbed adolescent) , governance issues (e.g., blocked tracheostomy, resuscitation room rebuild) and competencies linked to RCEM objectives. The ‘Mini Sim’ then takes place in situ within the ED resus, ED main department or our short stay observation ward which is under the auspices of the Children’s Emergency Department using real equipment and drugs. After the simulation a debrief is held and any additional teaching is carried out to embed learning. Each medical participant is then offered the opportunity to complete a work place based assessment on the ‘Mini Sim’ for their e-portfolio.

Evaluation of impact of ‘mini sim’
The work flow of the department has been unaffected and we have received excellent written feedback from participants about the educational quality of the programme which has also shown improvements in staff confidence in dealing with a variety of emergency situations. We would suggest this model could be used in other departments for similar gain.

{kind=link}
{kind=link}