Article Text

Abstract
Objectives: To (a) quantify the lethality of suicide methods used in Australia in the period 1 July 1993 to 30 June 2003, (b) examine method-specific case fatality by age and sex, and (c) identify changes in case fatality during the study period.
Methods: Two sources of data on episodes of self-harm in Australia were used, mortality and hospital separation data. Double counting of cases recorded in both sources was controlled by omitting fatal hospital cases from estimates of episodes of self-harm.
Results: Overall case fatality was 12%. For each suicide method, case fatality was higher in males and older age groups. Firearms were the most lethal suicide means (90%) followed by hanging (83%). Rates of suicide involving firearms declined over time, and those involving hanging rose. Case fatality for firearm cases changed little over time, but declined for self-harm by hanging/suffocation, poisoning, sharp objects, and crashing a motor vehicle.
Conclusions: This study (Australia) and two others (USA) show differences in method-specific lethality by gender and age. This study adds the finding of changes in lethality over time. Understanding of suicidality in populations, on which prevention efforts depend, requires explanation of these findings.
Statistics from Altmetric.com
Suicide is a major public health problem in Australia1 and globally.2 Over 20 years, nearly 50 000 lives were lost by suicide in Australia.3 Differences and similarities in suicide occur between countries, population segments, and periods. For example, suicide methods differ sharply between countries and by gender, age, and other factors. National analyses provide a basis for understanding these. Numerous factors have been found to influence the occurrence of suicide.4–10 Causes of suicide and suicidal behavior are multifactorial, and this is reflected in responses to the problem.11
Prevention has much potential, although establishing the effectiveness of preventive interventions is challenging.12 Several prominent approaches have emerged, focusing on mental health,13 provision of services for people in crisis,14 development of national suicide prevention programs,15 and limiting access to lethal suicide means.16
Choice of suicide means probably depends largely on availability and acceptability, although evidence on reasons for choice is quite limited.17 Availability of suicide means can influence suicide occurrence.18–25 Restricting availability of certain means has been associated with decreased method-specific suicide rates, and may decrease overall suicide rates.161926–29
Although many studies have analysed the effects of availability, acceptability, and restriction of suicide means, nearly all limit analysis to deaths, which are only part of the burden of intentional self-harm. Only a few studies have examined the lethality of suicide means.30–33
Published data are lacking on case fatality in Australia34 and most other countries. The few studies on lethality of suicide methods have not examined whether case fatality varies over time. Examining case fatality by sex, age, and time will improve understanding of suicidal behavior and might aid prevention. For example, the much higher suicide rates for males than for females in Australia and elsewhere have been attributed to different choices of means,35 but it is not clear what underlies the different choices, whether different means entirely explain the gender differential in rates, nor what factors might prompt change in means used, perhaps to more lethal ones. Method-specific lethality might change over time, due to preventive efforts, or for other reasons. For example, environmental controls are tending to reduce the toxicity of motor vehicle exhaust gas; is this reflected in lethality? Retrieval and treatment has potential to influence survival, probably more so for some methods (eg, overdoses) than others.
The objectives of this study are to use Australian data for 10 years to 30 June 2003 to: (1) quantify the lethality of suicide methods by calculating method-specific case fatality; (2) examine the relationship of sex and age to method-specific case fatality in Australia; (3) quantify changes over time in method-specific case fatality.
METHODS
Data on “completed suicides” (deaths) were obtained from national mortality files, compiled and coded by the Australian Bureau of Statistics (ABS). Data on cases resulting in hospitalization due to intentional self-harm were obtained from Australia’s National Hospital Morbidity Database, compiled by the Australian Institute of Health and Welfare (AIHW). Records included are for deaths and hospital discharges from 1 July 1993 to 30 June 2003, reported in terms of years ending 30 June (ie 1993–94 to 2002–03).
The data were coded according to the International Classification of Diseases (ICD). The ninth revision (ICD-9) was used for deaths registered by the end of 1998,36 and the tenth (ICD-10) for deaths registered since then.37 Hospital data were coded according to clinical modifications of the ICD. Versions of the ICD-9 clinical modification (ICD-9-CM) were used until the late 1990s,38 after which the Australian modification of ICD-10 was used (ICD-10-AM).39 ICD-10-AM was used for separations from 1 July 1998 in four Australian jurisdictions (NSW; Victoria; Northern Territory; Australian Capital Territory) and from 1 July 1999 in the remaining jurisdictions.
We specified 10 types of method of self-harm in terms of ICD-9 and ICD-10, selected so as to minimize any effects of the change in versions. Previous work shows that the version changes had minimal effect on suicide mortality data,40 and internal evidence suggests that the same is so for the ranges of the hospital cases used here. We included death records in which ICD codes corresponding to any of these types appears as the underlying cause of death and hospital records where any is the first external cause code, and the principal diagnosis code is in a range corresponding to injury and poisoning (ICD-9-CM, 800–904 or 910–995; ICD-10-AM, S00 to T79). Cases attributed to late effects of self-harm were not included. ICD codes and labels for the 10 types are: firearms (ICD-9 E955.0 to E955.4; ICD-10 X72 to X74); hanging, strangulation and suffocation (“hanging/suffocation” E953; X70); poisoning by gases and vapors (“Gases/vapors” E951, E952; X66, X67); poisoning by and exposure to solid or liquid substances (“drugs/poisons” E950; X60 to X65, X68, X69); drowning and submersion (E954; X71); jumping from a height (E957; X80); cutting and piercing by sharp objects (“sharp objects” E956; X78); lying or jumping before a moving object (E958.0; X81); crashing a motor vehicle (E958.5; X82); other and unspecified (E955.5, E955.9, E958.1 to E958.4, E958.6, E958.9; X75, X76, X77, X79, X83, X84).
The hospital data (AIHW) were classified as survived and died, according to the mode of separation data item. Those who died in hospital were excluded from our analysis to avoid double counting, on the assumption that these deaths are among the suicide deaths included in the mortality data from the ABS. Records of hospital episodes that ended with transfer to another hospital and statistical separations within a hospital were omitted to reduce multiple counting of cases involving multiple episodes in hospital. In this paper, “fatal episodes” of self-harm means completed suicides (ABS mortality data; n = 24 194), and “non-fatal episodes” of self-harm means cases recorded as being due to intentional self-harm which, based on the available data, were survived (NHMD hospital data; n = 177 967) (table 1). “Total episodes” were estimated as the sum of these. Case lethality for each method was estimated by dividing suicide deaths for that method by total episodes involving the same suicide method. Analysis was performed by sex, age, and year. Population data from the ABS were used to calculate rates. Rates were age-adjusted by the direct method, using the Australian population in 2001 as the standard. Microsoft Excel (MS Office 2003), SPSS (V12), and Stata (V9.2) packages were used to perform analyses. Confidence intervals assume a Poisson distribution of cases. Trends in case lethality were analysed by Poisson regression. Group-specific case fatality is not normally distributed, hence we used non-parametric tests, taking p<0.05 to indicate statistical significance. The Wilcoxon-Mann-Whitney test was used for sex, and the Kruskal-Wallis test for age groups.
RESULTS
Firearms and hanging accounted for about half of all suicide deaths in Australia in the decade to 30 June 2003 (table 1). Trends for these differed noticeably: the rate of suicide by firearms fell from 2.5 in 1993–94 to 1.0 in 2002–03 per 100 000 population, and the rate of hanging rose from 3.5 in 1993–94 to 5.2 in 2002–03 per 100 000 population. Rates of suicide by other means changed less.
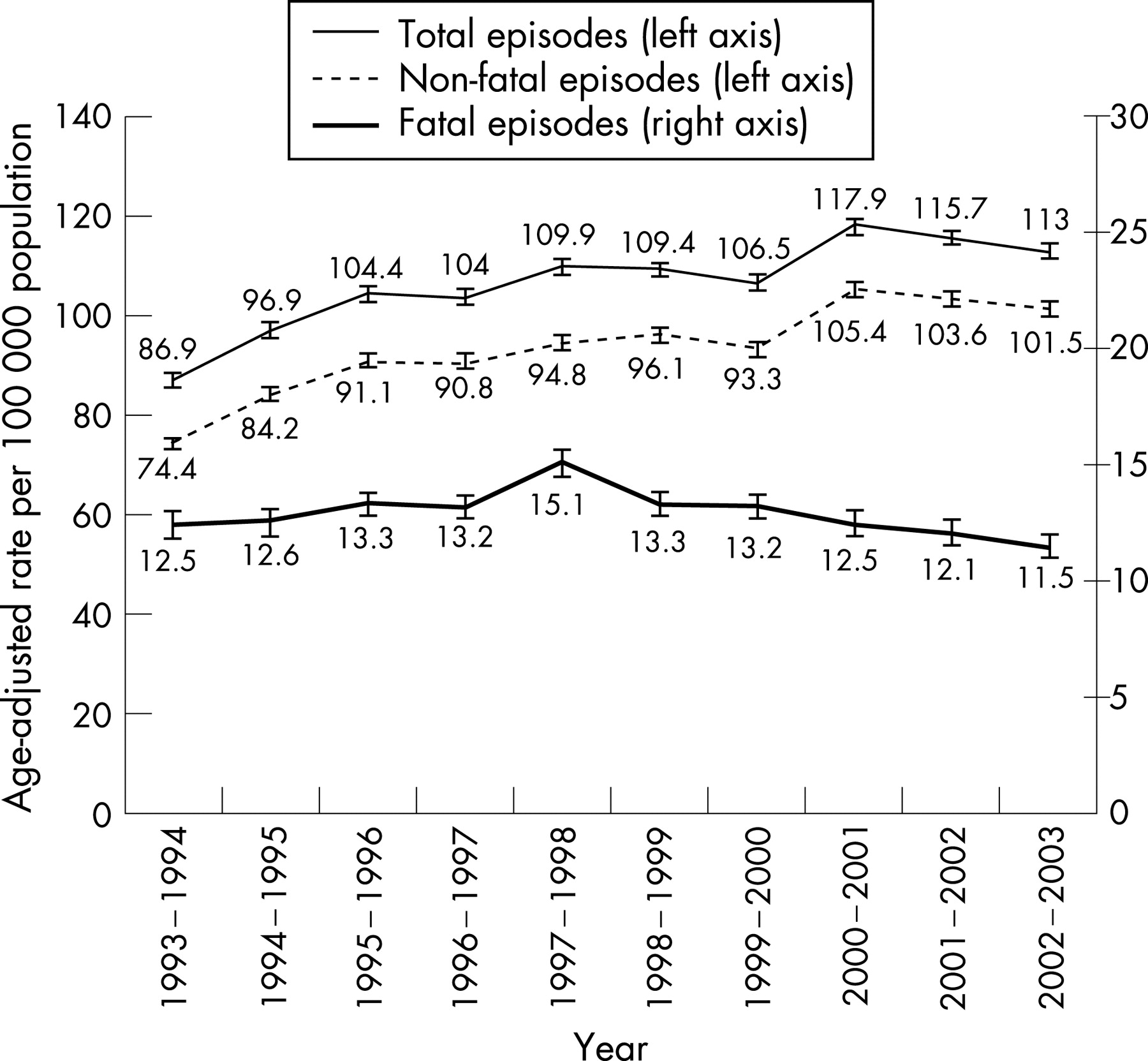
Total episodes of intentional self-harm (fatal and hospitalized non-fatal) rose from 87 in 1993–94 to 113 in 2002–03 per 100 000 population (fig 1). Fatal episodes (suicide deaths) increased from 12.5 per 100 000 in 1993–94 to 15.1 per 100 000 in 1997–98 then decreased to 11.5 per 100 000 in 2002–03. Non-fatal episodes increased from 74 in 1993–94 to 101 in 2002–03 per 100 000. Overall, of the total episodes (n = 202 161), 12% resulted in death (24 194). Of those admitted to hospital (n = 179 738), only 1% died and 99% were discharged alive.
Males accounted for 45% of total episodes and 80% of fatal episodes. Non-fatal episodes involved a female in 60% of cases. People aged 30 years and older accounted for 57% of total episodes and 71% of fatal episodes. Overall case fatality was much higher in males (21%) than females (4%), and increased with age group.
The most lethal suicide method was firearms (90% case fatality), followed by hanging, strangulation and suffocation (83%), which was the most common means of completed suicide in the study period (table 2). Case fatality for poisoning with gases was 61%, and the lowest observed case fatality was for drugs and other poisons (2%). Other suicide methods with high lethality (eg, drowning) were less common. Cutting or piercing with sharp objects was rare among fatal cases and had a low case fatality proportion.
Case fatality varied between methods in much the same way for males and females, but the proportion of fatal cases was lower for females for every method studied (fig 2). The differences between sexes are significant (Wilcoxon-Mann-Whitney test p<0.05) for each method except jumping before a moving object.

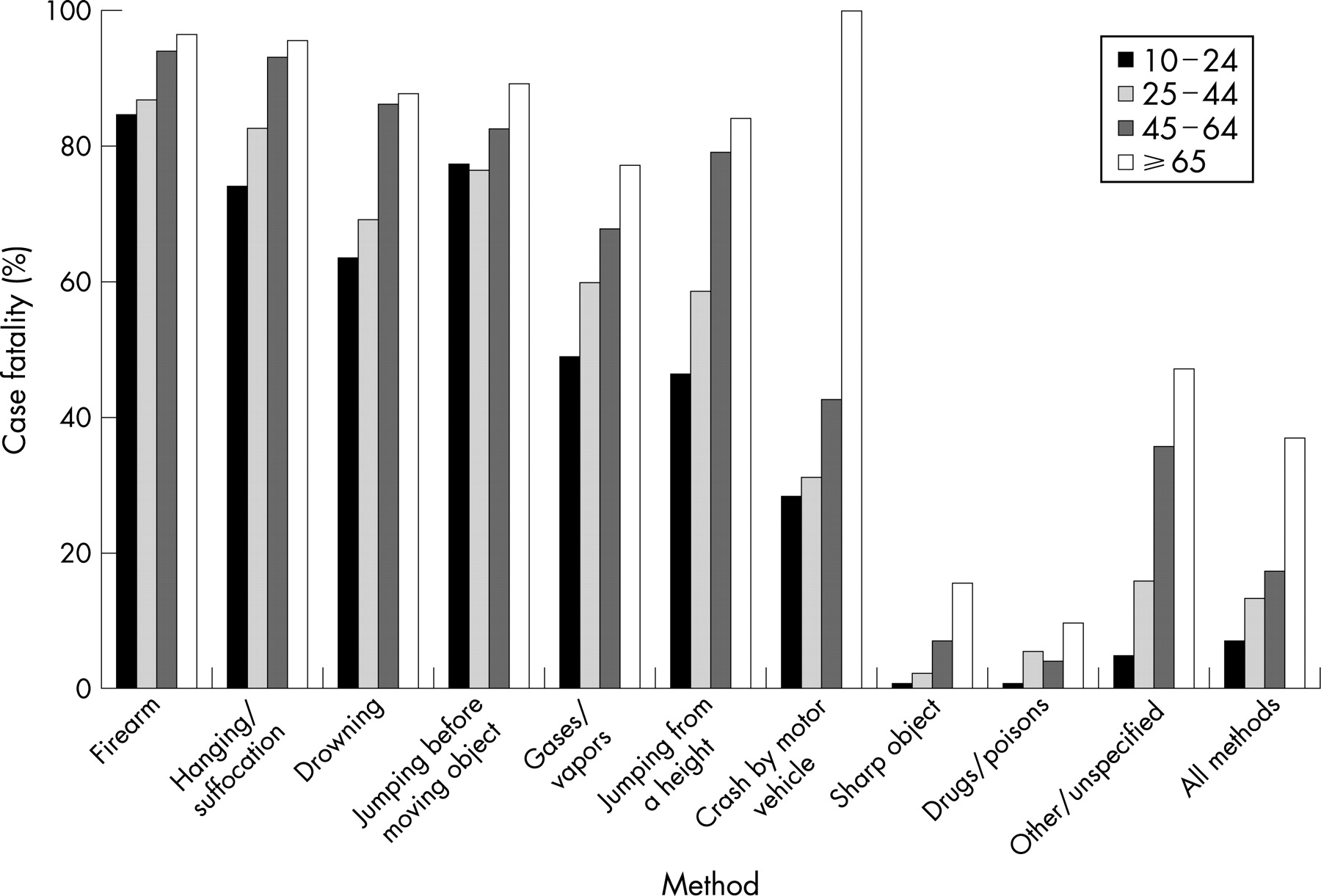
Case fatality rose with age for most methods, although this pattern was less marked for some methods (eg, firearms) than others (eg, poisoning by gas; jumping from a height) (fig 3). Case fatality variation between age groups is significant for each method (Kruskal-Wallis test p<0.05).

Several methods show distinctive profiles. Firearms accounted for 20% of suicide deaths in 1993–94, but this proportion had declined to 9% by 2002–03. Total episodes and fatal episodes by this means were much higher in older age groups and for males; 17% of episodes resulted in admission to hospital, and 59% of people were discharged alive.
For hanging, strangulation, and suffocation, total episodes and fatal episodes gradually increased to a peak in 1997–98, then decreased. In contrast, non-fatal episodes increased throughout the decade. Hanging accounted for 28% of all suicide deaths in the first year of the study period, increasing to 45% in 2002–03. In 18% of the recorded cases of intentional self-harm by hanging, strangulation, and suffocation, the person was admitted to hospital; 86% of these people were discharged alive. Fatal episodes and total episodes involving hanging increased with age group to a peak at ages 30–34 years, then decreased with increasing age. Non-fatal episodes of hanging increased from 0.5 per 100 000 population in 1993–94 to 1.4 per 100 000 in 2002–03.
The percentage of suicide deaths due to poisoning by gas changed little between 1993–94 (20%) and 2002–03 (18%). Poisoning by drugs showed a similar small decline from 16% of suicide deaths in 1993–94 to 14% in 2002–03. In contrast, total episodes of poisoning by drugs increased from 66.6 per 100 000 in 1993–94 to 86.1 per 100 000 in 2003 and accounted for 77% of overall total episodes. In 98% of recorded cases of self-harm by poisoning with drugs, the person was admitted to hospital; 99% of these survived to discharge. Total drug poisoning episodes in females increased from 7497 cases in 1993–94 to 11 047 cases in 2002–03, and, in males, from 4642 to 5913 cases. Despite the large excess of female episodes involving drug poisoning, males outnumbered females among fatal cases involving this method.
Considering all methods of self-harm together, overall case fatality decreased from 14% in 1993–94 to 10% in 2002–03. Changes in method-specific case fatality show marked differences (fig 4). Firearms showed no significant trend. Case fatality for most other methods showed generally downward trends. An almost 10% decrease in case fatality occurred for hanging (p = 0.001) and poisoning by gas (p<0.001). Downward trends were also statistically significant for drugs/poisons (p<0.001), sharp objects (p = 0.002), and crashing a motor vehicle (p = 0.001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
Previous studies have described completed suicides in Australia.193441 We broaden the view by using both hospital data (non-fatal episodes) and death data (fatal episodes). During the period of the study, non-fatal episodes had a different profile and trend from completed suicides. The rate of non-fatal episodes increased through the period, whereas the rate of fatal episodes rose until 1997–98, then fell. This pattern might be explained by changed methods of self-harm (with an overall decrease in case fatality), changes in retrieval or treatment (increase in survival from some types of self-harm), or changes in information (eg, changes in case ascertainment).
The methods for which use changed most were hanging and firearms, which together accounted for about half of all suicide deaths. Was the rise in suicide by hanging causally related to the decline in suicide by firearms? The relationship between the increase in suicides by hanging and the decrease in firearm-related suicides is ambiguous.41 Substitution between methods has been postulated in several studies,162642 although, as Kreitman26 argued, substantiating its occurrence requires more than observing opposing trends.
Hanging rose dramatically, from 28% to 45% of fatal episodes and even more for non-fatal episodes. Most of these episodes were at young ages (15–39 years), which accounted for 79% of non-fatal episodes and 60% of fatal episodes. Males outnumbered females by 5:1 for fatal episodes and 4:1 for non-fatal episodes. Case fatality showed a steady decline during the study period, the decline being more prominent at younger ages than at older ages. The reasons for this profile are not clear, and limitations of the data have so far restricted further investigation. One possible explanation is that the category “hanging, strangulation, and suffocation” includes sub-types of cases with different lethality and that the mixture of types has changed over time. Other possible explanations are that hospital admission practices have changed in a way that increases the proportion of such cases that are admitted (including less lethal types), or that under-ascertainment of fatal cases has increased.
Firearms more than halved as a means of suicide during the decade. Fatal and non-fatal case numbers declined to a similar extent, and so case fatality showed no significant change over time. Hence, the decline in mortality from this cause appears to be due to a decline in use of this means. (Had we seen only a decline in fatal cases, other explanations would be more plausible, such as a change in the weapons used—for example, less lethal weapons—or in the location of the wound, or increased survival because of better retrieval or treatment.) The decline in fatal cases began before the study period, case numbers peaking in the mid-1980s. The authors of an evaluation of all firearm-related deaths in the Australian state of Victoria for a period overlapping with our study period found strong associations between declining firearm-related suicide and indicators of reduced availability of firearms and firearm regulatory changes.43
Hanging and firearms were favored methods for different population segments. Age-specific rates for hanging peaked at about 30 years of age, then declined with age, whereas rates for firearm cases rose with age. Hanging was less gender-specific than shooting: the ratio of male to female cases was 5:1 for hanging and 15:1 for shooting, and hanging was the most common fatal means for both genders. The decline in rates of suicide by firearms was most marked for older men, and the increase in hanging was most marked for younger males, and was less evident for young females. Case fatality decreased over time for hanging (especially at younger ages) and showed no significant change for firearms. These and other differences between cases involving hanging and firearms in terms of sex, age, timing of changes, and case lethality lead us to doubt whether the concept of substitution has much to contribute to understanding the broadly opposite trends observed for fatal cases of self-harm involving these means.
Poisoning by gases, the second most common method for fatal cases, showed a decline in lethality during the study period. Suicidal poisoning by gases mainly involves motor vehicle exhaust. Lester16 has pointed out that emission controls have tended to decrease the toxicity of exhaust gas, which may have contributed to the observed decline in lethality.
The “gender paradox” of suicide is that females tend to exhibit more suicidality than males, but male rates of fatal self-harm are generally higher than female rates.35 This is evident in the overall rates of fatal and non-fatal episodes that we have observed, 60% of non-fatal episodes involving females and 80% of fatal episodes involving males. This gender-specific difference largely, but not wholly, reflects the use by females of less lethal means, particularly poisoning by pharmaceutical drugs. However, we found that the lethality of each of the methods that we examined was lower for females than males (fig 2). Intriguingly, this was so even for firearms, although female case numbers for this means were low. The present study does not explain these differences, but prompts questions for future work.
Case fatality generally increased with age, although with different patterns for each suicide method (fig 3). The decline with age of physiological robustness probably accounts for part of this effect but, as with gender, it might also reflect age-specific differences in means of self-harm within the broad types that we were able to distinguish.
Method-specific case fatality in our national study of Australia concurs with findings for two regions in the USA.3133 Our finding of changes in lethality over time is novel.
Key points
Suicide data describe only part of the consequences of suicidality in a population. Hospital data can be used to describe another part.
Case distribution by age, gender, means of self-harm, and trends over time differ between these two data sources.
Means-specific case fatality of self-harm increased with age, was higher for males than females, and tended to decline over time for most means, but not for shooting.
Our study has limitations. Suicidal acts that did not result in hospital admission or death were not included, because of lack of data. Hospital data included only cases that were complicated or serious enough to result in admission. The data sources used are nominally complete collections of registered deaths and admitted hospital cases. The hospital data have been reported to be nearly complete,44 although misclassification of cause may occur. The social sensitivity that surrounds suicidal acts and uncertainty concerning intent in some cases suggest that the risk of under-counting is greater than the risk of over-counting. Observed changes in mechanism-specific case numbers coded as intentional self-harm could be affected by changes in the proportion of cases with a given mechanism that were coded as having this intent. The most likely alternative codes are “unintentional” and “undetermined intent” categories that refer to the same mechanism. Comparison of mechanism-specific groups for each of these three intent groups can provide suggestive evidence on the presence of such effects—for example, the presence of trends of similar size and shape, but with opposing direction. We applied this approach, and conclude that it is not plausible to explain the trends observed for intentional self-harm in terms of counter-trends in unintentional or undetermined intent categories. In the main, undetermined intent categories had too few cases to influence results to an important extent. We note, however, that data system changes during the study period complicated the assessment, particularly for cases in the poisoning/drugs mechanism group. Recent reports have indicated that suicide may be under-enumerated in recent death data.45–47 Hence, these sources might underestimate the number of suicides and suicide attempts.4849 Transition from ICD-9 to ICD-10 and from ICD-9-CM to ICD-10-AM appears to have had little impact on comparability of self-harm over time.4050 We examined the lethality of suicide means but were not able to examine the factors that influence the choice of suicide means. These limitations are similar to those of other studies of the topic. A strength of our study is that case fatality has been examined over time and in an entire national population.
Our work has raised questions warranting further study.
Would inclusion of non-fatal episodes of self-harm that are not admitted to hospital result in markedly different findings? Can survey data be used for this purpose?
To what extent are the observed differences in means-specific lethality between males and females, age groups, and time periods due to heterogeneity of methods included in the categories available in the ICD?
Intentional self-harm, as defined in ICD, is not restricted to acts with suicidal intent. Can suicidal and non-suicidal self-harm be distinguished in administrative data, and with what effect on analyses of lethality?
IMPLICATIONS FOR PREVENTION
Suicidality encompasses more than completed suicides, and understanding is deepened by considering non-fatal as well as fatal cases. For example, availability of morbidity data reveals that the decline in completed suicide by firearms in Australia is better explained by a reduced incidence of attempts than by reduced case fatality.
Study of outcomes of suicidal behavior in terms of methods of self-harm reveals demographic and temporal patterns, which can usefully inform planning for prevention and interpretation of trends in suicide.
Suicide death rates depend on case fatality as well as on the incidence of episodes of self-harm. Overall case fatality depends on the profile of methods of self-harm in a population, which can vary a lot. However, determinants of the pattern of methods used are poorly understood, limiting options for prevention.
Acknowledgments
Analysis in this paper is based on data provided by the Australian Institute of Health and Welfare (hospital data) and the Australian Bureau of Statistics (deaths data). The authors, and not these agencies, are responsible for the results and interpretations presented.
REFERENCES
Footnotes
Competing interests: None.