Article Text

Abstract
Background Decreasing Injuries from ALcohol (DIAL) is a randomised control trial of a telephone brief intervention (BI) with injured emergency department (ED) patients with high-risk alcohol use. Here the authors examine 12-month outcomes of the intervention's effect on alcohol use, alcohol-related injuries and alcohol-related negative consequences.
Methods ED research assistants recruited adult injured patients who screened positive for high-risk alcohol use and were to be discharged home. After discharge, all participants received by telephone an assessment of their alcohol use, alcohol-related injuries, and alcohol-related negative consequences and then were randomised to treatment or standard care. Treatment consisted of two telephone sessions of BI focusing on risky alcohol use. Both groups were reassessed after 12 months.
Results At 12 months, 249 (89%) participants completed follow-up assessments. After using a log transformation, the difference in alcohol-related injuries between baseline and 12-month follow-up was greater in the BI group than the standard care group (p=0.04); this is an effect size of Cohen's d=0.21. No difference between groups was found when comparing change in alcohol consumption and other alcohol-related negative consequences at 12 months.
Conclusions These findings suggest that a telephone BI with injured ED patients may decrease alcohol-related injuries. Identifying patients with risky alcohol use in the ED and then subsequently delivering the intervention by telephone after discharge has promise as a model for BI and deserves further study.
- Drowning
- alcohol/drugs
- MVTC
Statistics from Altmetric.com
Alcohol use is a risk factor for many types of injury.1 ,2 Although the evidence is somewhat mixed,3 brief interventions (BIs) for alcohol have demonstrated some success when delivered to patients in emergency departments (EDs) across varying outcomes.4–6A few studies have demonstrated that ED staff can be trained to perform alcohol screening and BI7 ,8 but barriers to adoption and implementation of ED screening and interventions exist including time constraints, and not having the skills or additional resources to address alcohol use problems.9 One approach to address these barriers is to deliver the BI portion, which requires more time and skill, separate from the ED visit.
We have previously described an alternative model for screening and BI for ED patients that utilises the ED as an opportunistic setting to screen patients but delivers the BI by telephone after discharge from the ED.10 The rational for this model is that the ‘teachable moment’ perhaps exists while the patient is in the ED and may extend to a time period beyond the initial ED visit.11 In addition, patients may be more receptive to the intervention when they are in less pain, out of the chaotic environment of the ED, and in a more comfortable setting. Using a randomised control study design, previously we have demonstrated that ED patients who screened positive for high risk alcohol use and received a telephone delivered BI after discharge had decreased impaired driving at 3 months compared with those receiving ED standard care (SC).10
Goal of this investigation
While telephone BI has been demonstrated to change a high-risk behaviour (impaired driving), we now seek to test whether it is also effective at a more distal time point in decreasing injury occurrence. The primary aim of the present study is to test the effect of BI given by telephone soon after the patient's ED visit on the frequency of alcohol-related injuries and other alcohol-related negative consequences at 12-month follow-up.
Materials and methods
Study design and setting
Decreasing Injuries from ALcohol (DIAL) was a randomised clinical trial funded by CDC's National Center for Injury Prevention and Control from 2003 to 2006 at a large, urban academic level trauma centre and two smaller community hospital EDs in nearby suburban settings. Eligible participants were injured ED patients with risky alcohol use who were randomised to one of two groups. The BI group received (1) routine ED SC, (2) assessment of alcohol use, alcohol-related behaviours and injuries, (3) a BI by telephone and (4) a follow-up booster telephone intervention. The SC group received only (1) routine ED SC and (2) assessment of alcohol use, alcohol-related behaviours and injuries. All protocols were reviewed and approved by the Institutional Review Boards at the study institutions and registered with clinicaltrials.gov (NCT00457548).
Selection of participants
Research assistants during preselected times representing all shifts and days of the week screened all non-critically injured adult ED patients (≥18-year-olds) using a health behaviours survey that included questions on smoking, exercise, stress and amount of alcohol use. Those using alcohol at risky levels defined as exceeding the National Institute on Alcohol Abuse and Alcoholism quantity frequency guidelines at that time (either ≥14 drinks/week for male subjects, ≥7 drinks/week for female subjects or ≥5 drinks/occasion for male subjects, ≥4 drinks/occasion for female subjects)12 were eligible for the study. Additional eligibility requirements included being discharged from the ED to home, having a phone, English speaking, not suicidal and not in police custody. In the first year of the study, we only recruited motor vehicle crash (MVC) patients and then for the remainder of the study all injured patients were screened for eligibility.
In the ED, a research assistant met with eligible patients to explain the purpose of the study and schedule telephone contact for enrolment, randomisation and research assessments. Furthermore, it was explained that if randomised into the BI group the participant would be invited at that time and during a subsequent call 2 weeks later to engage with a trained interventionist in a brief conversation about risky alcohol use. All participants were compensated for their time completing baseline and follow-up assessments for a total of $70.
All participants received an assessment of their alcohol use, impaired driving, alcohol-related injuries and alcohol-related negative consequences during the initial telephone call. After assessment, participants were randomised to either BI or SC group by research staff opening an envelope that contained allocation assignment. The BI group received a BI that was approximately 30 min in duration during that initial call and received an additional approximately 15-min BI booster session during a second call 2 weeks later. The telephone BI was delivered by Master or PhD level research staff. The BI was based on the principles of motivational interviewing13 and utilised the participant's own resources to bring about changes needed to reduce alcohol-related risky behaviours. The participant defined these changes during the BI telephone calls. Change could involve overall alcohol consumption but also, using a ‘harm reduction’ model, change could also be reflected in the decrease of specific risky behaviours such as driving after drinking. The counsellor's role was to be reflective, to provide an atmosphere that would support and enhance the participant's motivation for change, and lead the participant to initiate and persist in behavioural change efforts.13 A licensed clinical psychologist, with experience in BI, monitored maintenance to intervention fidelity through weekly clinical supervision sessions with the counsellors. During these sessions, counsellors' notes were reviewed and discussed to assure protocol adherence as well discuss any difficult participants.
The SC group received only routine ED care and the same assessment instruments at baseline and follow-up. At the time of the study, the EDs where recruitment occurred had no protocols in place for universal alcohol screening for ED patients. All alcohol screening, any interventions and any referrals to outside treatment facilities were at the discretion of the treating ED clinician.
Sample size was calculated using the effect size (d=0.34) of a previous randomised clinical trial at our institution using face-to-face BI delivered in the ED for reducing alcohol-related injuries of those who had been injured by an MVC.11 Using Cohen's procedure for calculating sample size, with a power of 0.80 and an α of 0.05, we needed to recruit 114 participants per treatment condition to evaluate differences in outcomes. With an estimated attrition rate of 20%, we determined 143 participants per treatment condition to be necessary.
Methods of measurement and data collection
Both the BI and SC groups received the same assessments by telephone at baseline prior to randomisation. All 12-month data were collected by a research assistant blinded to treatment condition. Alcohol use was measured by the 10-item alcohol use disorders identification test (AUDIT)14 at baseline and AUDIT-C, an abbreviated version that only utilises its three consumption questions (1 through 3), at 12 months.
Alcohol-related injuries using the Injury Behaviour Checklist (IBC)4 and alcohol-related negative consequences were measured at baseline and 12-month follow-up. The IBC asks participants about how often each of the 17 injuries had occurred in the past 12 months. If a participant affirms that an injury had happened, a subsequent question about the use of alcohol prior to injury occurrence is asked. Previous research4 has suggested that alcohol-related injuries are most sensitive to change from a BI delivered to injured ED patients who report patterns of harmful or hazardous drinking. Therefore, the IBC total number of alcohol-related injuries was used as the outcome variable. Alcohol-related negative consequences were measured using the Drinker's Inventory of Consequences (DrInC),15 a 45-item questionnaire that asks participants about the frequency of a broad array of alcohol-related events over the past 12 months. The total sum of the frequency of report of the 45 items was used as the outcome variable.
Data were collected on paper and then using a double data entry system transferred to an electronic database (Illume 2.2, DatStat, Seattle, Washington, USA). The database was electronically checked for inconsistent entries and then electronically transferred to SAS V.9.1 (SAS Institute, Inc.) for analysis.
Outcome measures
DIAL's primary outcome measures at 12 months were change in alcohol use (AUDIT-C), change in alcohol-related injuries (IBC) and change in alcohol-related negative consequences (DrInC) between baseline and 12-month follow-up assessment.
Primary data analysis
Using an intention to treat analysis for all participants randomised, descriptive analysis of demographic and baseline measures was done by comparing BI and SC groups. To test the study hypotheses of the superiority of BI versus SC for all 12-month study outcomes one-tailed analyses were done. All data were examined to identify the appropriate distribution of the variables. When a non-normal distribution was identified, the appropriate transformation was applied prior to the analysis of the data and is noted in the results section.
Results
Characteristics of study participants
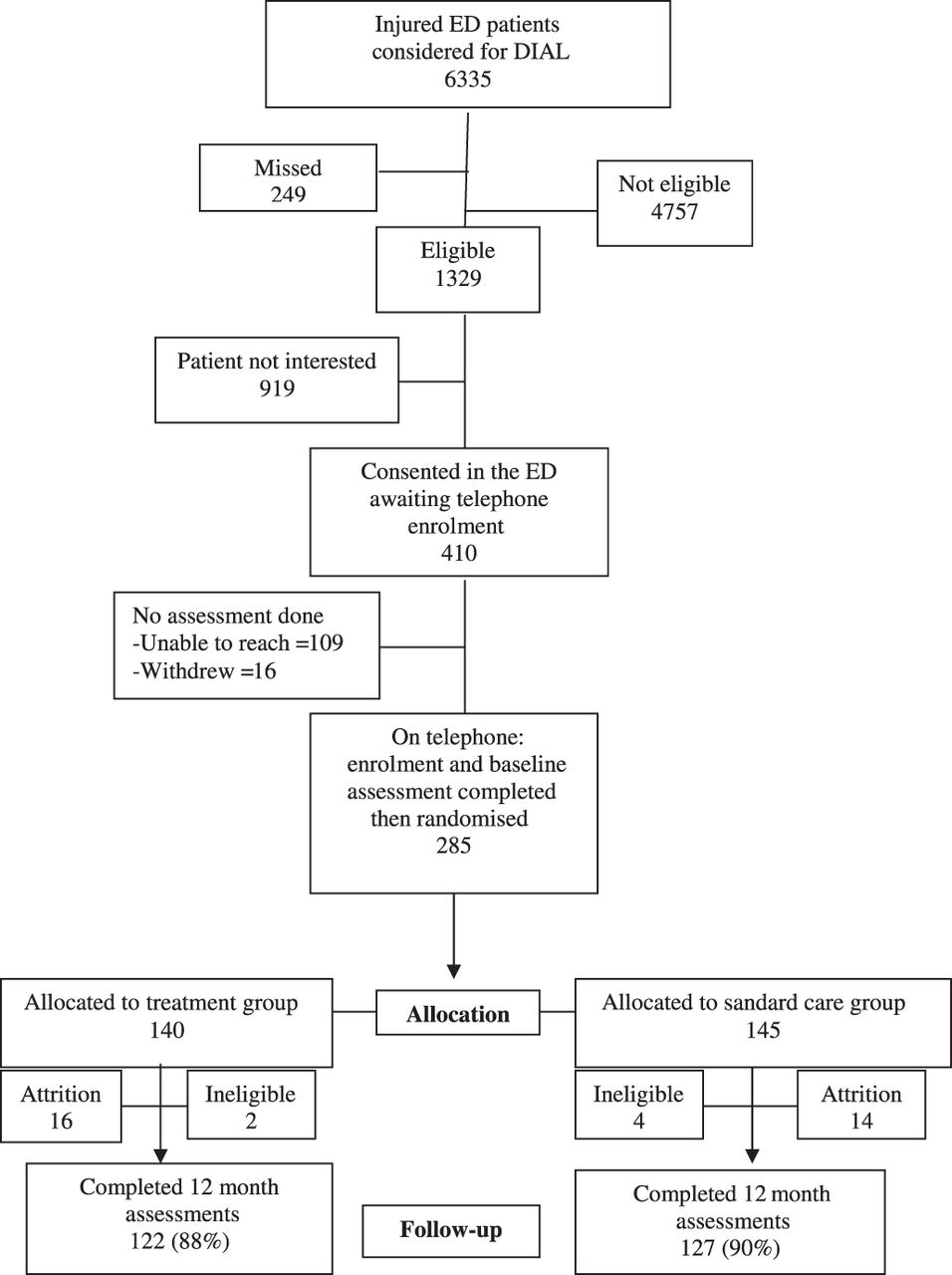
During the recruitment period, research assistants were present in the EDs when 6335 injured ED patients were being treated and could be screened to see if they met protocol eligibility. Research assistants did not screen 249 patients in this group because the patient refused screening, were discharged prior to screening or were otherwise unable to be located. Of the 1329 patients that met protocol eligibility criteria, 410 consented in the ED to receive a telephone call in the days following discharge for enrolment, assessment and randomisation. Of that group, 125 were not enrolled because we were unable to contact them or they voluntarily withdrew. Those patients who were eligible but not enrolled did not differ from those participating in the study by age, gender, ethnicity, injury type (MVC or other) or baseline alcohol use.10 The study sample initially consisted of 285 participants contacted by telephone who completed the baseline assessment, and were randomised into BI (n=140) or SC (n=145) groups (see figure 1).
{kind=link}
DIAL subject recruitment and disposition. DIAL, Decreasing Injuries from ALcohol; ED, emergency department.
After ED discharge, the average time until telephone assessment and randomisation was 5 days (range 1–28 days; median =4 days). Half of participants were contacted on the first telephone attempt and 90% were contacted by the third attempt. During that same phone call, 92% of participants in the BI group completed the BI immediately after completing the baseline assessment. The other 8% were recontacted later by phone, on average 9 days after randomisation, to receive the BI. The BI session averaged 31.2 min (SD=13.4; range 10–77 min; median=30 min). The subsequent booster BI session 2 weeks later averaged 18.8 min (SD=9.28; range 5–50 min; median=15 min) and was received by 69% (n=97) of participants in the BI group.
During data analysis it was found that six participants did not meet baseline alcohol eligibility requirements and were removed from the final analysis. Of the 279 eligible participants whose data were analysed, 138 were randomised to receive the BI condition and 141 were randomised to the SC condition (see figure 1). Of those randomised, 249 completed the 12-month assessment (89%), with 122 (88%) completed by the BI group and 127 (90%) by the SC group. This is the sample that is being reported on in these analyses. As can be seen from table 1, the SC and BI groups did not significantly differ by any demographic variables except age (the SC group having a higher mean age than the BI group).
Demographic characteristics by treatment group
Main results
Alcohol-related injuries (IBC) that participants had received in the 12 months before and after randomisation into the study were analysed. The examination of the distribution of the IBC data demonstrated that it was non-normal and therefore log and square root transformations were conducted. A log+1 transformation of alcohol-related injuries yielded the most appropriate results for these data. Table 2 shows the baseline, 12-month and difference between baseline and the 12-month assessment of alcohol-related injuries for each treatment condition. As can be seen in table 2, the BI group did decrease the mean number of alcohol-related injuries between baseline and 12-month follow-up significantly more than the SC group (t (247)=1.71; p=0.04). The effect size of the difference in the decrease of alcohol-related injuries between the BI and SC groups was calculated using Cohen's d as an effect size estimate. The effects size calculated (d=0.21) is a small effect size.
Alcohol-related injuries at baseline and 12 months
Analysis of the distribution of alcohol-related negative consequences (DrInC) summary score demonstrated that a square root transformation was appropriate. As can be seen in table 3, both groups had a decrease in alcohol-related negative consequences at 12 months. There was no group-wise difference between baseline and 12-month DrInC scores. AUDIT-C as a measure of alcohol consumption also decreased in both groups from 12-month pretreatment to 12-month post-treatment, but there was no significant difference between the BI and SC groups (table 4).
Differences in alcohol-related negative consequences (DrInC)
Difference in alcohol consumption variables (AUDIT-C)
As age was significantly different between the groups, age was entered into a regression analysis with the difference between the baseline and 12-month injuries as the dependent variables. Age was not predictive of the difference between the baseline and 12-month alcohol-related injuries (ß=0.10; t=−1.63; p=0.10). Analysis examining the effects of cause of injury (MVC or other injury cause) on difference in BI effect for binge drinking, IBC or DrInC was also conducted and no differences were found.
Limitations
The most important caveat in interpreting our findings is that we studied a very specific segment of the ED population, non-critically injured patients who were to be discharged from the ED. Of the 17 234 patients that were in the ED while our research assistants were present, 10 899 were not eligible mostly due to being evaluated for a medical illness rather than an injury or being injured but admitted to the hospital. Future research will need to establish if ED patients being treated for a medical illness will respond to a telephone BI regarding alcohol use. Another limitation is that not all patients in the BI group received the booster session and this may have impacted our findings. Our inclusion of participants who did not utilise the second booster session would most likely result in a diminution of the BI effect and therefore should not change the direction of our findings related to alcohol-related injuries.
Discussion
BI for alcohol with ED patients that was delivered while the patient was in the ED has demonstrated variable efficacy.3 ,6 DIAL expands on this by continuing to utilise the ED as a unique opportunity to identify ED patients using alcohol in a risky manner but now delivering the intervention by telephone after discharge. We delivered the intervention during a time period following the ED visit (a week) when patients were hypothesised to be receptive to BI and in a mode (telephone) that was convenient to the patient and devoid of the turbulence present in the ED. We earlier found that DIAL decreased impaired driving at 3 months and here we suggest that alcohol-related injuries, a more distal outcome, may also be reduced for the group receiving telephone BI compared with the SC group.
We did not find a difference between the BI and SC groups in the overall decrease in alcohol-related negative consequences at 12 months; both BI and SC improved. This suggests that our assessment alone, the injury itself or ED SC may have some effect on future alcohol-related negative consequences.
Despite our previous finding of a decrease in impaired driving at 3 months and a decrease in alcohol-related injuries at 12 months, DIAL did not find a difference in alcohol consumption between BI and SC groups at either of these time points. In a recent meta-analysis of studies on ED BIs for alcohol problems, it was found that although alcohol consumption amounts were not significantly changed, there was a significant decrease in alcohol-related injuries.5 An explanation may be that the BI focused on injury prevention and high risk behaviours such as impaired driving, not on reducing alcohol consumption as an end in itself. Thus, it could be that the amount of alcohol consumption might not change but the activities encompassing its use might change, yielding a decline in alcohol-related injury occurrence. An alternative explanation is that the AUDIT-C is not sufficiently sensitive to detect small differences that might have occurred over this time period.
While demonstrating that telephone BI may have both a proximal effect in reducing impaired driving behaviour and a more distal effect on reduced alcohol-related injuries, several matters continue to be unclear. Most importantly, which ED patients benefit from a telephone BI? Research efforts need to continue to ascertain a profile of ED patients (eg, reason for the ED visit, degree of alcohol misuse, prior negative consequences from alcohol use, readiness to consider making a change, age, gender, ethnicity) that BI benefits to assist in concentrating resources to that group.3 Furthermore, the dose of the intervention needs further delineation. The effect we found is very modest and perhaps an increased dosage of the intervention might increase the effect. Further research is need to determine if two calls are sufficient or is there benefit gained from additional calls, and what is the cost to benefit ratio of any additional calls?
In summary, our findings suggest that a telephone BI for alcohol may decrease alcohol-related injuries though not other negative alcohol-related consequences or alcohol use. Identifying these high-risk patients in the ED and then subsequently delivering the intervention by telephone after discharge demonstrates the potential as a model for intervention and deserves more investigation of its efficacy.
What is already known on the subject
Alcohol screening and brief interventions have been shown to be effective at reducing alcohol use and alcohol-related negative consequences. It has been difficult to implement this within emergency department clinical care because of the time constraints inherent in this busy environment.
What this study adds
It is feasible to screen emergency department patients for alcohol misuse in the emergency department and then contact by telephone those screening positive in the days following their emergency department visit to deliver a brief intervention on alcohol. These brief interventions may decrease subsequent alcohol-related injuries.
References
Footnotes
Presented in part at the 2008 American College of Emergency Physicians Research Forum, 28 October 2008, Chicago, Illinois, USA.
-
Funding This work was supported by CDC's National Center for Injury Prevention and Control (R49/CCR1232280; Mello-PI). The contents of this publication are solely the responsibility of the authors and do not necessary represent the official views of the CDC.
-
Competing interests None.
-
Ethics approval The ethics approval was provided by the Rhode Island Hospital IRB.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement A deidentified dataset of study data utilised in this manuscript is available by contacting the corresponding author.