Article Text

Abstract
Background: Small volume nebulisers (SVNs) with masks commonly provide aerosol therapy for infants with lung diseases. However, infants and toddlers are often disturbed by and thus reject masks.
Aims: To compare the lung deposition efficiency of the “usual” SVN aerosol mask and a prototype hood attached to an SVN. The advantage of the hood is that no mask is needed and medication can readily be administered during sleep.
Methods:99mTc salbutamol solution was administered at random by SVN plus mask or hood to 14 wheezy infants (mean age 8 (SD 5) months). The dose and distribution of salbutamol were evaluated using gamma scintigraphy. Clinical response, tolerability by the infants, and parent preference were also compared.
Results: Mean total lung deposition was 2.6% with the hood and 2.4% with the mask (p > 0.05). Variability with the mask was greater than with the hood (coefficient of variation (CoV) 54% v 39%). Both treatments provided similar clinical benefit and side effects as reflected in improved oxygen saturation, reduced respiratory frequency, and increased heart rate. Infants accepted the hood better than the mask and there was a positive correlation between poor acceptance and upper airways and stomach deposition for both treatment modalities. Parents preferred the hood treatments.
Conclusions: Aerosol therapy by hood is as efficient as by mask but provides a better therapeutic index. It is much better tolerated by infants and preferred by parents. Hood nebulisation is a simple and patient friendly mode of aerosol therapy in wheezy infants.
- aerosol
- infant
- nebuliser
- deposition
- inhalation therapy
- hood
- mask
- CoV, coefficient of variation
- GIT, gastrointestinal tract
- HR, heart rate
- LDE, lower respiratory tract delivery efficiency
- LRT, lower respiratory tract
- MDI, metered dose inhaler
- MMAD, mass median aerodynamic diameter
- ROI, region of interest
- RR, respiratory rate
- SatO2, oxygen saturation
- SVN, small volume nebuliser
- URT, upper respiratory tract
- VHC, valved holding chamber
Statistics from Altmetric.com
- CoV, coefficient of variation
- GIT, gastrointestinal tract
- HR, heart rate
- LDE, lower respiratory tract delivery efficiency
- LRT, lower respiratory tract
- MDI, metered dose inhaler
- MMAD, mass median aerodynamic diameter
- ROI, region of interest
- RR, respiratory rate
- SatO2, oxygen saturation
- SVN, small volume nebuliser
- URT, upper respiratory tract
- VHC, valved holding chamber
A erosol medications have long been used in infants for the treatment of various respiratory disorders.1–3 Most devices for administering aerosol medications to infants are derived from those developed initially for delivery of asthma medications to adults and older children. Most of these devices were modified for use by infants simply by adding a small face mask covering the mouth and nose, which provides the interface between the aerosol generator and the patient. For optimum therapy, the edge of the mask must seal to the infant’s face during treatment. It has been shown that even a 1 cm gap between the mask and the face reduces the dose delivered by 50%.4 Achieving a good mask–face seal may be difficult in many infants because of squirming and crying.5 Although there is a tendency to move away from nebulisers towards smaller pressurised metered dose inhalers (MDIs) with holding chambers, these also use a face–mask interface, with all the problems noted above. Nebuliser treatments take about 15 minutes and since this is longer than most infants will tolerate, they become impatient and obstreperous, thus greatly reducing the drug delivery efficiency to their lungs.6,7 There is clearly a need to develop more acceptable and patient friendly interfaces for improving aerosol delivery to infants.2
The use of alternative interfaces which do not touch the infant’s face, has recently been suggested by Lotufo and colleagues,8 who treated young (2–5 years old) children with asthma using a tent covering the child’s head. Similarly, in an attempt to minimise environmental contamination, Wahlin and colleagues9 used a hood to deliver aerosolised ribavirin to infants with respiratory syncytial virus bronchiolitis. Indeed, head canopies, or hoods, have long been used for delivery of oxygen and saline aerosols (for example, mist tents) in neonates and infants. As no face mask is required and nothing touches the face, a hood interface should provide a logical and compelling, child friendly alternative means of delivering nebulised drugs to infants.
The clinical efficacy of bronchodilator or anti-inflammatory and antiallergic aerosols depends primarily on deposition in the pulmonary airways. The most direct way to study the relative efficiencies of two aerosol delivery systems is to quantify the dose and distribution of an inhaled drug using identical radiolabelled aerosols. No other clinical, pharmacological, or in vitro techniques are as well suited for this purpose.10
This pilot study utilised gamma scintigraphy to compare the nebulised salbutamol lung dose and distribution between the “standard” mask treatment versus a hood which replaced the mask as the interface between the nebuliser and the infant. Clinical variables, acceptance by infants, and parents’ preference were also evaluated.
SUBJECTS AND METHODS
Design
The study was a prospective, open, randomised crossover clinical trial comparing lung dose and distribution and clinical outcome following administration of bronchodilator by the two aerosol inhalation modes.
Using computer generated randomisation, infants with acute wheezing were assigned to receive the first study treatment either by a jet nebuliser (Micromist, Hudson Respiratory Care Inc., CA, USA) with a face mask or by the same nebuliser and hood (fig 1). Six hours later the patient was given the alternate treatment. This interval was chosen as a compromise between the need to minimise pathophysiological changes in airway calibre over time and with the need to reduce interference from residual lung radioactivity following the first treatment by decreasing the radioactivity by one half life.11

Infant undergoing hood nebuliser treatment.
Patients
Fourteen (five females, and nine males aged 1–19 months (mean 8 (SD 5) months) spontaneously breathing, hospitalised, wheezy infants, who required frequent inhaled β agonist bronchodilator treatments, as judged by the attending physician,14 were enrolled in the study.
Sample size calculations for the primary outcome were based on previous lung deposition data in infants receiving bronchodilator treatment via conventional nebulisers.12,13 Based on these data we estimated that there would be a more than 80% chance of detecting a 50% difference in deposition between the groups (alpha = 0.05) when sample size (n) is 14 patients for each treatment group.
Inclusion criteria included: acute episodes of wheezing for less than 48 hours; age >4 weeks and <2 years; oxygen saturation >92% on admission; admitted for longer than 12 hours; bronchodilators needed at least once every three hours; and on inhaled β agonist treatment only.
Subjects were excluded if they had cardiopulmonary disease such as bronchopulmonary dysplasia, congenital heart disease, immunodeficiency, or cystic fibrosis.
Written informed consent was obtained from the parents or guardians of each patient. The study protocol was approved by the Sieff Hospital Ethics Committee and the Israeli Ministry of Health.
Treatments
General
Study treatments were administered during two regularly scheduled inhalation treatments on the second day in hospital—that is, 12–24 hours post admission. All efforts were made to mimic as closely as possible the actual conditions of treatment on the ward. In particular, care was taken to ensure that the second study treatment was administered at the same time interval following a bronchodilator treatment as the first study treatment.
Hood
A single custom made prototype clear perspex hood was used for all studies (fig 1). The hood consisted of a circular dome of diameter 30 cm and height 25 cm. It had two (3 cm diameter) side openings to allow extra venting. The nebuliser outlet was attached to the hood through a 22 mm internal diameter adapter
Mask
For the face mask treatment, infants were held by the caregiver in a seated position with the neck slightly extended. The mask was held firmly against the infant’s face.
Medication
For each of the study treatments, the nebuliser was charged with 0.5 ml of 0.5% salbutamol respirator solution (Glaxo Wellcome, Ware, UK) diluted to a total of 3 ml with 0.9% saline. Medication was labelled with technetium-99m DTPA (99mTc) solution. The dose of 99mTc to be given to each patient was assessed before the inhalation procedure was performed, so that none would receive a total dose exceeding 2 mega becquerels (MBq). Addition of 99mTc has no physical effect on aerosol characteristics.15–18
The nebuliser was driven by an oxygen cylinder at a flow rate of 8 l/min for exactly six minutes. Under these conditions, the Hudson nebuliser has a mass output of 0.26 ml/min, and produces particles with a mass median aerodynamic diameter (MMAD) of 4.2 μm and geometric standard deviation 1.8.19
Outcome measures
The primary outcome measure was lung aerosol deposition measured scintigraphically by means of a technique detailed previously.20 In short, scintigraphic scans of 60 seconds duration were obtained after each treatment. Gamma camera counts (corrected for decay and tissue attenuation) were measured in the following regions of interest (ROIs): (1) head; (2) trachea, oesophageal, and gastric areas (upper respiratory tract (URT) and gastrointestinal tract (GIT)); and (3) lung: total lung counts were obtained for both lungs. For regional lung aerosol distribution only the right lung was assessed to avoid corruption of the data by activity in the lower oesophagus and stomach behind and adjacent to the left lung.21 Aerosol deposition in each of the areas defined above was expressed as a percentage of the amount of radioactivity delivered from the nebuliser.
Secondary outcome measures
-
Clinical observations: (a) oxygen saturation (SatO2) by pulse oximetry; (b) respiratory rate (RR); and (c) heart rate (HR) (all recorded before and 20 minutes after completion of each of the two treatment modes).
-
Behavioural assessment: infants were observed every minute during the study treatment. One point was scored for every minute that the infant either cried or resisted the treatment for more than 20 seconds; a behavioural index of 6 represented maximal distress whereas 0 represented no distress.
-
Parent preference: parents were asked to state if they had a preference, or no preference, for either delivery method.
Precautions
Patients received the treatment in a special room within the nuclear medicine department, used only for this purpose. No person other than the patient and a physician were allowed in the room at any time. Radioactivity protection monitoring was carried out regularly and following each study, to ensure that no excess radioactivity was present in the room following treatments.
To avoid contamination of the infant’s chest during treatment, thus interfering with lung gamma camera counting, the infant’s body was enclosed in a special nylon cover, which was removed immediately after completion of the inhalation treatment. Caregivers were gowned and wore a head covering which were later appropriately discarded. Non-rebreathing valves attached to absolute filters were used at the mask and hood openings. The absorbed total body radiation dose of 99mTc aerosol used in this study was calculated according to the Medical Internal Radiation Dose Committee.11 It is equivalent to the radiation received during a 12 hour flight, or that received as background radiation over a period of about three weeks,10 and is much lower than the doses used in diagnostic imaging procedures. 99mTc is a pure gamma emitter and has a short (6 hours) physical half life.11
Pilot experiments with five infants receiving unlabelled inhaled treatments through the hood identified no increase in percentage CO2 within the hood.
Statistics
Statistical tests were two sided conducted at the 0.05 level. Paired t tests were used to compare the two treatments. Deposition, clinical response, and behavioural indices were related by simple regression. Parental preference was analysed by Fisher’s exact test.
RESULTS
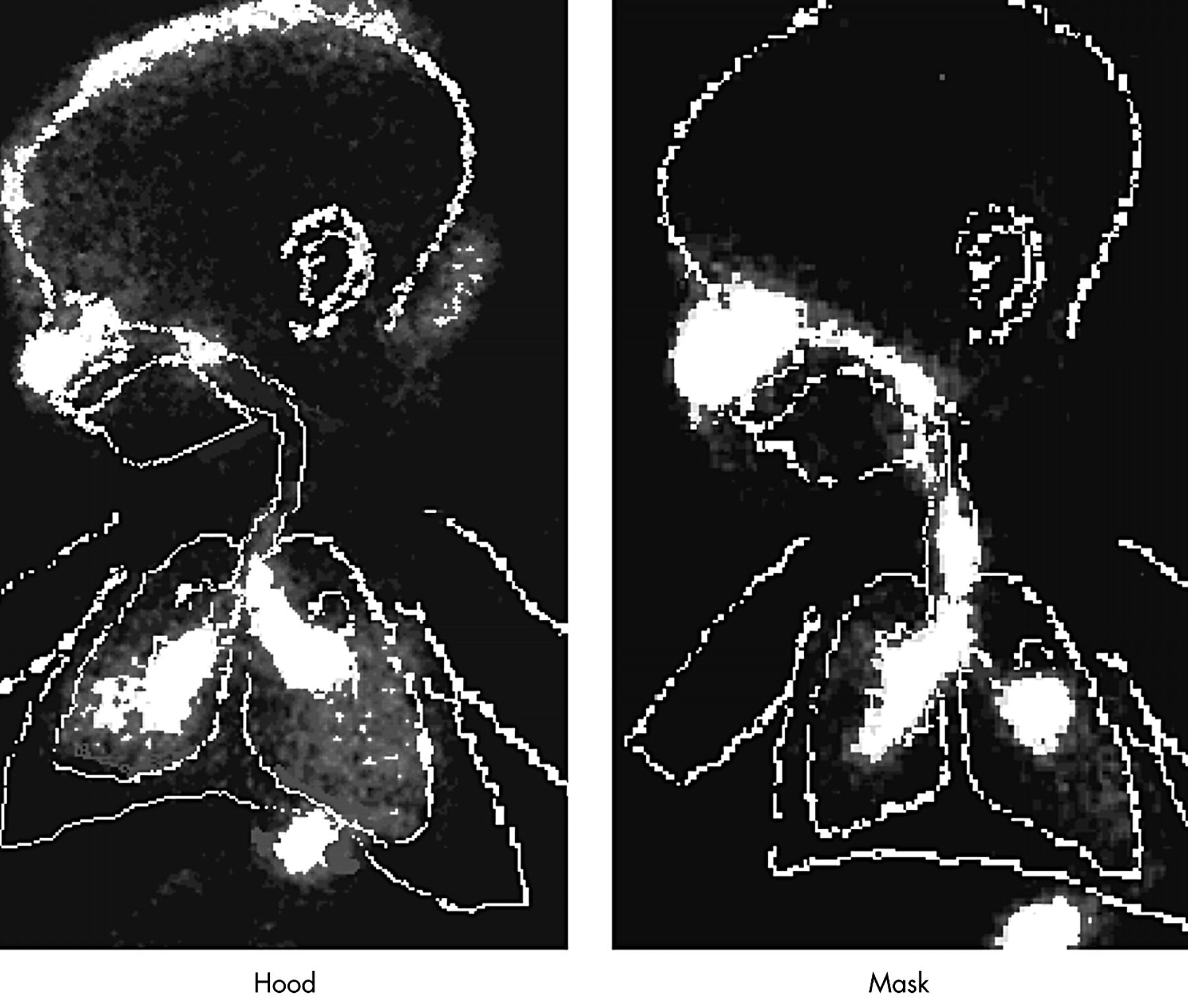
There was no significant difference between the average output of the nebulisers (49% of the initial charge for the hood treatments and 46% for the face mask treatments). Figure 2 shows typical scans of one of the patients where the lung and body markers are superimposed. The mean group values for deposition in the right lung with the hood system (1.32% (SD 0.52%)) were no different than the values with the mask system (1.18% (SD 0.64%, p = 0.4; table 1). Similar values were obtained for the total left lung. Thus the total lung deposition fraction was 2.6% with the hood and 2.4% with the mask. Approximately half of the total lung dose penetrated to the peripheral lung region. There was no significant difference in total or regional lung deposition between face mask and hood, although the intersubject variability in lung deposition for the mask (CoV = 54%) was much greater than for the hood (CoV = 39%, p < 0.001). Both aerosol delivery systems were associated with significant combined URT and GIT deposition (8.4% with the mask and 7.6% with the hood, p = 0.57). About 10–12% of the delivered dose remained on the head with both treatments. The remainder was found in the hood, on the bed where the infant’s head lay, within the face mask, and on the exhalation filters.
Individual deposition data (%) for the whole right lung (total), for the central region of the right lung (central), and for the URT and GIT during both treatments modalities

Scans of one of the patients obtained during hood and mask treatments. Body and lung markings are superimposed for clarity. Note the considerable deposition in the URT and GIT during the mask treatment.
Table 2 shows the clinical response data. Both aerosol delivery systems resulted in statistically significant and clinically relevant benefit as reflected in improved oxygen saturation and reduced respiratory rate. Both were associated with an increase in the heart rate.
Clinical outcomes before (pre) and after (post) treatments in both groups
Neither total nor regional distribution (with either delivery system) was related to the infant’s age, height, or body surface area, nor to any of the clinical variables.
With regard to behavioural and parental assessment, the hood was associated with significantly less patient distress (mean behavioural index of 1.3 during hood v 3.4 during mask treatments, p = 0.01) and significantly greater parental preference compared to the face mask (hood preferred by 12 parents (86%, p < 0.01), mask by one, and no preference by one). While there was no significant correlation between behaviour index and lung deposition, the former was highly correlated with the URT–stomach deposition for both aerosol delivery systems (r = 0.80, p < 0.01 for the hood and r = 0.56, p < 0.05 for the mask; fig 3). The greater the infant’s distress, the greater the URT and GIT deposition.

{kind=link}
{kind=link}
{kind=link}
Comparison of scintigraphic URT and GIT deposition data and behaviour index during hood and mask treatments.
DISCUSSION
The present study shows that in infants, the lung deposition fraction, aerosol distribution, and clinical response to hood nebulisation are as good as the conventional mode of treatment using a nebuliser with face mask. Acceptability to infants and parents’ preference markedly and significantly favoured the hood treatments.
Nebulisers with face masks are commonly used to administer aerosol medications to infants.22,23 However, use of the face mask is associated with many difficulties mostly related to poor acceptance of the mask, which must greatly decrease the efficiency and clinical efficacy of the treatment.2,3 It is a common complaint of most parents that they find it very difficult to keep a mask tightly fitted to their infant’s face for more than a few seconds at a time. Noble and colleagues24 found that about 30% of their patients did not accept the mask while awake, and 17% did not accept it even when asleep and had to be withdrawn from a clinical study. Recently, we and others have reported the likelihood of poor aerosol delivery to infants using face masks, primarily because of an inadequate face mask seal.5,25 Persisting with a screaming infant as parents often do, is not a good solution as it has been shown that little aerosol medication is deposited in the lungs,6,7 and using force may make subsequent aerosol treatments more difficult.
In contrast to the face mask, the transparent hood provides similarly efficient aerosol delivery without facial contact. Little cooperation on the part of the infant is required, aerosol delivery is entirely passive, parents are relaxed, and the baby comfortably inhales the medication while tidal breathing, awake or asleep. Even when awake, the presence of the caregiver, and the absence of the unfamiliar and obtrusive face mask and perhaps also the cool, moist stream of air appeared to be much less upsetting to the infants. Comparing the babies’ behaviour between the two modalities for aerosol delivery, clearly showed the advantages of the hood. All patients achieved better adherence with the hood and parents significantly favoured the hood treatments.
Only anecdotal information is available regarding the relation between behaviour of the infant during inhalation treatment and respiratory tract deposition. Tal and colleagues6 reported that lung deposition during crying in two of their patients who inhaled MDI generated salbutamol from a valved holding chamber (Aerochamber, Trudell Medical International, London, ON, Canada) with mask was only about 0.35%, in contrast to a mean of 2.5% when breathing quietly. Murakami and colleagues7 also reported that lung deposition in crying infants using a nebuliser and mask was negligible (scintigraphic data were provided for one patient). Wildhaber and collegues26 recently described their experience with one crying child whose lung deposition was markedly reduced compared to his non-crying peers. Moreover, gastrointestinal deposition in this patient was 50% higher than in the rest of the group with a sevenfold increase in the ratio of gastrointestinal (from swallowed aerosol medication) to lung deposition. Our study showed for the first time, in a well powered series of patients, that while there was no relation between infants’ behaviour and total lung deposition during aerosol therapy, there was a clear relation between infants’ behaviour and deposition of aerosol in the URT that was subsequently swallowed and detected in the gastrointestinal tract. The more distressed the infants were, the more aerosol was deposited extrathoracically. This is probably related to the fact that crying or screaming is associated with greatly prolonged expiration followed by short, high inspiratory flow velocity gasps leading to greater aerosol impaction in the throat27 and frequent swallowing. While increased bronchodilator deposition in the URT and GIT may not be of great clinical significance in infants with asthma, this observation may be of greater concern during nebuliser treatments with corticosteroids22 because of increased systemic absorption and a greater risk of side effects. This study shows the need to, and provides a simple solution for, improving adherence with respect to aerosol administration in infants by maximising their comfort. Because of improved and more consistent pulmonary drug targeting, a better therapeutic ratio should result. The nebuliser hood system is an inexpensive and appealing alternative to nebulisers and masks. Furthermore, even with nebulisers and a face mask interface, treatment of poorly cooperative infants should, if possible, be attempted while they are in deep sleep, thus avoiding as much as possible crying and agitation.28
Both aerosol delivery systems have a low lower respiratory tract (LRT) delivery efficiency (LDE) with less than 3% of the nebulised salbutamol actually reaching the LRT. Since in the present study all efforts were made to avoid leakage from the mask, deposition, during face mask treatment under “real life” conditions, where infants commonly do not achieve a tight seal with their mask,5 may be much less.2 Furthermore, only about half of the total dose reached the lung periphery, with no difference between the two aerosol delivery systems. In adults, LDE with most commonly used nebulisers is fourfold greater, reaching 10–12%.29 Despite the poor LDE in infants, there was similar clinical benefit with both aerosol delivery systems. It is thus apparent that even when relatively minute amounts of bronchodilator reach the β receptors in the airways, the response in infants is likely to be similar to that achievable by a fourfold or greater multiple adult dose because of their proportionally much smaller airway surface area.30
Hood nebulisation also minimises dispersal of potentially sensitising or toxic drug aerosol into the room. This may be particularly important with drugs such as corticosteroids, ribavirin, or antibiotics.31 The hood also reduces the potentially irritating compressor noise (50–70 dB) which may further contribute to reduced acceptance of nebulisers by infants and their caregivers.32
There is a convincing body of evidence showing that MDI with valved holding chambers (VHC) are as good as nebulisers for delivering aerosol medications to children.33 Nevertheless, a face mask is still the only available interface between the VHC and the child. It would be of interest to determine if the hood could also replace the VHC–face mask combination.
Based on this study, the hood has become our standard of care in the paediatric department for all babies who require nebuliser treatment. The method has gained widespread acceptance from parents, nurses, and colleagues. This aerosol delivery interface has not only improved acceptance by infants but has also reduced personnel time, simplified treatment schedules, and pleased caregivers.