Article Text

Abstract
Objective: There are no systematic methods for toxicovigilance of non-medicinal products in the UK. This is particularly relevant for pesticides, where there is significant public concern about potential adverse effects. This study describes a prospective toxicovigilance scheme based on follow-up of enquiries to the National Poisons Information Service (NPIS) through its online poisons information system TOXBASE. These enquiries reflect acute exposures and the patterns of acute illness that result.
Results: A total of 10 061 pesticide-related enquiries were identified. After follow-up, data were gathered on 2364 suspected exposures, of which 1162 involved children. After exclusions, 1147 exposures are reported here. No deaths were reported and only 37 children were admitted to hospital. The majority were considered to have either minimal or no features (925, 80.6%). Symptoms for 38 children were unknown. Symptoms reported in the other 184 children included nausea or vomiting (58), eye irritation, pain or conjunctivitis (29), skin irritation (28), abdominal pain (24), mouth or throat irritation (18) and diarrhoea (15). Where age was recorded, 60.5% (680) of children involved in suspected pesticide exposures were aged 2 years or less. The most common scenario for acute accidental exposure to pesticide in children was exposure after application (329, 28.7%) or due to poor storage (228, 19.9%).
Conclusions: Areas of potential concern identified included storage, access of young children to “laid” baits and pesticides, and exposures as a result of medication errors, with liquid head lice preparations being confused with other medicines. Use of NPIS systems provides a potentially useful method of toxicovigilance.
Statistics from Altmetric.com
There are at present no formal toxicovigilance structures in the UK for monitoring the effects of exposures to pesticides. These continue to cause anxiety among members of the public.1–4 Management of these cases presents a challenge to health professionals, particularly in childhood, where there is relatively little information on acute outcomes from these exposures. For most pesticides, acute effects reflect the extent of exposure. This information is of relevance to licensing, improved safety in use and advice on treatment.
We therefore conducted a longitudinal study, the first of this type reported in the UK, to examine the health effects of pesticide exposures using National Poisons Information Service (NPIS) systems.5 6 Here we report findings in exposures of children (⩽12 years old) to pesticides about which enquiries were made to TOXBASE between 1 April 2004 and 31 March 2007.
What this study adds
This first longitudinal study of its type to be performed in the UK provides information on the nature and range of exposures.
It provides significant reassurance that pesticide products currently available do not present a generalised acute health hazard after accidental exposure.
It also demonstrates that toxicovigilance studies such as this can gather potentially valuable exposure information.
METHODS
TOXBASE is the internet database of the NPIS.7 A list of pesticides of specific interest was agreed between the Pesticides Safety Directorate of the UK Health and Safety Executive and NPIS Edinburgh in 2004, and monographs for these pesticides were identified on TOXBASE. By March 2007, 324 TOXBASE entries for products and specific agents were being tracked. Users accessing these pesticides for a patient-related enquiry were requested to complete an online form. If they did not, a postal questionnaire based on that of Leverton and colleagues8 was sent, with a covering letter and prepaid return envelope. No postal questionnaires were sent to NHS Direct or NHS 24, because of the difficulties of identifying case details in their systems. Responses about the same exposure were combined.
All telephone enquiries to NPIS Edinburgh (>90% from Scotland) about pesticides received during the period were followed up. Thus the total number of questionnaires comes from three sources: electronic questionnaires, follow-up of TOXBASE users who did not complete an electronic questionnaire and follow-up of telephone calls to NPIS Edinburgh.
The severity of acute poisoning in children was assessed in two ways. First, respondents were asked to grade the exposure (“not at all serious”, “minor”, “moderate”, “major”, “uncertain”). Second, experienced poisons information staff in Edinburgh used the poisoning severity score (PSS): (“fatal”, 4; “severe”, 3; “moderate”, 2; “minor”, 1; “none”, 0; or “uncertain”), to grade the symptoms reported.9
RESULTS
Between 1 April 2004 and 31 March 2007, a total of 10 061 patient-related pesticide enquiries were identified.
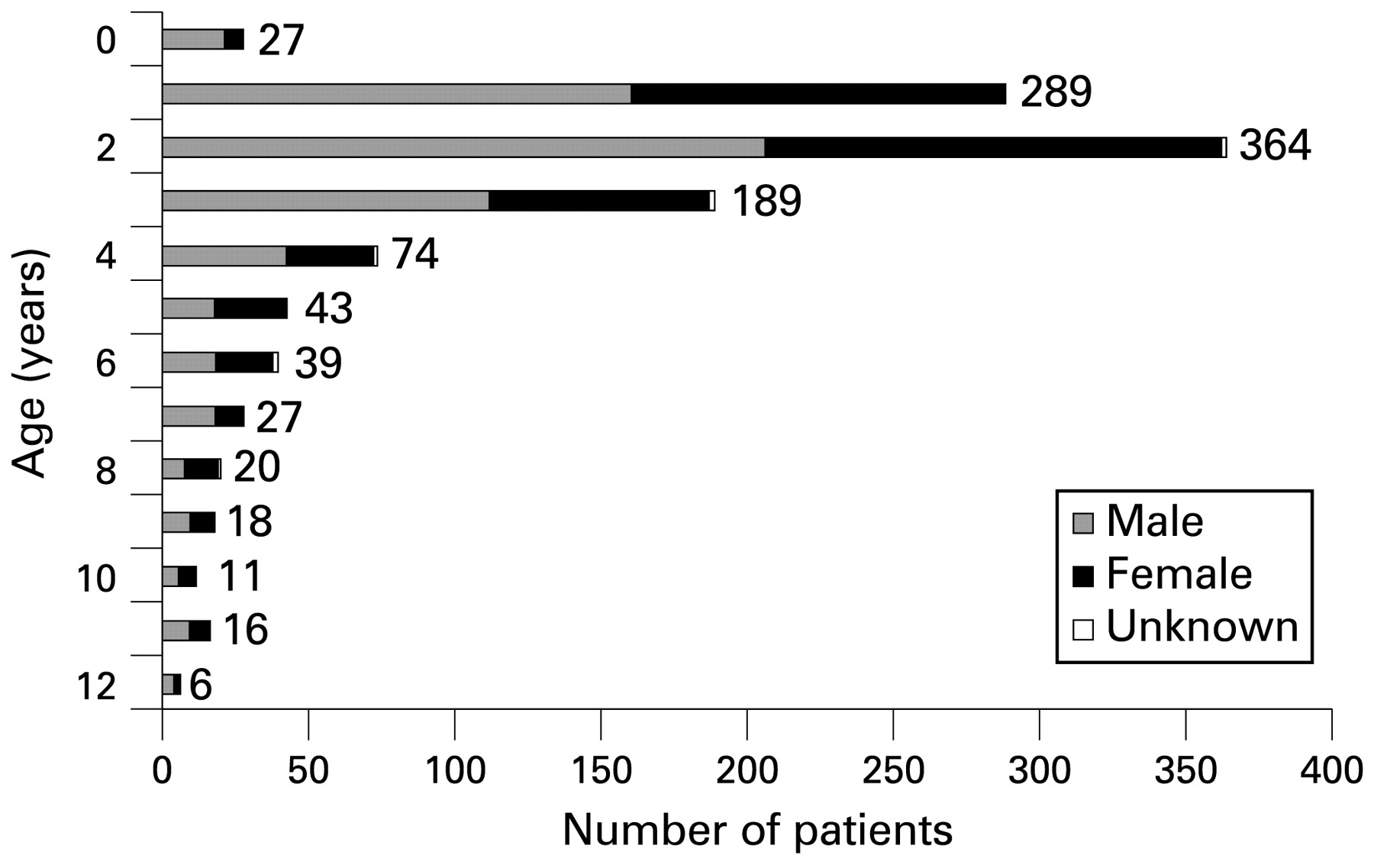
Data on 2364 patient exposures were subsequently gathered, of which 1162 concerned exposures of children. Nine children were excluded from the analysis because their symptoms were thought not to be related to the exposure (eg, timings of exposure and symptoms; other illness deemed responsible). Other reasons for exclusion were deliberate self-harm (1), exposures reported as chronic (3) and exposures where the nature of the putative exposure was not identified (2). Of the 1147 acute accidental exposures of children reported, 1123 had a specific age recorded; 680 of these children were aged 2 years or less (fig 1). Only 295 (45.5%) of 649 responders reported the patient as “definitely” exposed.
{kind=link}
Age distribution of 1123 children involved in acute accidental exposures whose specific age was recorded.
Overall, 56.6% (642) of the children were boys, as were 77.7% (21) of those <1 year old (fig 1). There was no gender difference in older children (table 1).
The vast majority of children (1106, 96.4%) were not admitted to hospital or were discharged on the same day. Thirty-seven required admission for one day, 24 having no symptoms and 11 minor symptoms only. The severity of childhood exposures was considered “minor” or “not at all serious” by the responder in 76.1% (431) of 566 cases. PSS scores indicated low toxicity, with no cases graded PSS 3 or 4; 12 graded PSS 2; 166, PSS 1; 925, PSS 0; and 44, “uncertain”.
There were 403 (35.0%) exposures involving insecticides: 215 pyrethroids (1 sheep dip), 18 organophosphorus insecticides (2 sheep dips), 52 carbamates and 119 others, of which 90 were boric acid. Among exposures to insecticide (239), 20.8% involved ant killers. Other major categories were herbicides (110, 9.6%), rodenticides (259, 22.5%), slug killers (139,12.1%), head lice treatment (178, 15.5%), wood preservatives (36, 3.1%) and fungicides (8, 0.7%).
The active ingredients most frequently identified in these exposures of children were permethrin (insecticide), malathion (head lice treatment) and metaldehyde (slug killer) (table 2). Most exposures (94.4%) were to products for non-professional use in the home or garden.
The most common scenario for acute accidental exposure in children was that they were exposed as a consequence of use but not during application (329, 28.7%). These were often to bait-type products, or were due to unsatisfactory storage (228, 19.9%). Of the 329 cases where the exposure occurred after application, 119 (36.2%) involved rodenticides; 96 (29.2%), ant killers; and 53 (16.1%), slug killers. The most frequent route of exposure was ingestion (778, 69.1%). Multiple routes of exposure were found for 17.9% (201) of children.
Symptoms were absent in 925 (80.6%); for 38 the question was answered “unknown” or was not recorded; in the 184 children who had symptoms, these included nausea or vomiting (58), eye irritation (29), skin irritation (28), abdominal pain (24), mouth or throat irritation (18) and diarrhoea (15).
Of exposure to head lice treatments, therapeutic error accounted for 29 (16.3%) of 178, these products being mistaken for an oral medication (41.4% for paracetamol). Seven (24.1%) patients exposed because of therapeutic error had symptoms, similar to the prevalence of symptoms in head lice exposures overall (43, or 24.4%).
Of 259 patients exposed to rodenticides, 44 respondents recorded measuring the INR (international normalised ratio) or prothrombin time, although most (26) did not report the result. Of the 18 who did record the outcome, 16 found normal and only two prolonged prothrombin time.
Specific treatment was reported as not required in 86.5% (608) of the 703 cases. In the 29 cases where a specific treatment was recorded, it involved eye irrigation (13), oral activated charcoal (5), skin decontamination (5), topical antibiotics to the eye (4), oral fluids (2), analgesia (2), gastric lavage (1), intravenous fluid (1), oral antihistamines (1), oral antibiotics (1) or topical emollient (1), in line with the advice provided on TOXBASE. No children were admitted to intensive care, required ventilation or were reported to have significant complications or longer-term effects from the exposure. There were no deaths reported in our study group, and the national data sets on mortality are not product specific10 and so do not assist further analysis in this regard.
DISCUSSION
In contrast to the situation for drugs, there is at present no formal system for toxicovigilance for other products in the UK.11–14 The importance of post-marketing surveillance has been recently emphasised in connection with adverse effects in respect of waterproofing sprays15 and toys.16
TOXBASE product entries were accessed more than 1 000 000 times in 2007. Since pesticide accesses are a small proportion of the total database use, intensive monitoring of the type described is possible. There was a disappointingly low response rate (7.8%) to online use of a questionnaire and this may reflect the way in which TOXBASE is used in front-line clinical situations. Follow-up rates were far higher for telephone enquiries (53.6%) and postal questionnaires (23.6%). It is not possible to say whether symptoms may positively bias the return of reports, but as the children in 80.6% of cases reported were asymptomatic, this seems unlikely.
The distribution of patient age and gender reported in this study reflects many of the patterns that have been found in previous epidemiological studies of general poisoning and suggests that the data collected reflect the overall pattern of exposure.17–25 These similarities support the concept that the surveillance approach we have used is likely to reflect overall patient exposure patterns, and while it is possible that this low response rate might bias the results, these similarities make it less likely.
It is unlikely that all patients were exposed to pesticide if exposures reflect other experience in childhood poisoning where laboratory confirmation was conducted.26 Confirmation of exposure to pesticides is challenging in routine practice, as assays are not widely available. In this series, exposures to anticoagulants and organophosphates (cholinesterase inhibitors) are best suited to this approach. Thus, of 18 children exposed to anticoagulants, the results of clotting studies were abnormal in only two. No assays were reported in relation to organophosphates, but assays are clinically indicated only in patients with symptoms.
Most exposures (84.0%) occurred in children under the age of 5 years, with children aged 2 the most frequently exposed (fig 1). These findings concur with those of previous studies on childhood poisoning.18–22 25 27–30 Most of the exposures reported either occurred after the pesticide, usually a bait-type compound, had been applied (28.7%) or were due to unsatisfactory storage (19.9%). Exposures through ingestion were common (in 69.1%), with rodenticides (22.5%), ant killers (20.8%) and slug killers (12.1%) being prominent.
Despite the large number of children presenting to healthcare professionals, most exposures did not produce symptoms (80.6% asymptomatic) and were considered of “minor” severity (76.2%) by the healthcare professional involved. Most of the children exposed (96.4%) either were not admitted to hospital or were discharged on the same day. No patients were reported as being admitted for more than 2 days. The cases in which an admission of 2 days was recorded followed exposure to rodenticides.
Head lice treatments accounted for 15.5% of exposures. There is potential to reduce therapeutic error through education, repackaging or improved storage. These products were either mistaken by children themselves or by carers as an oral pharmaceutical.
CONCLUSIONS
The effects of potentially toxic pesticides on health can be monitored using NPIS resources. Most suspected pesticide exposures of children resulted in no clear acute adverse health outcome and were considered of minor severity. No children were reported to have died or to have been admitted to intensive care. Nevertheless, issues such as safety of storage and care after application of bait-style products were highlighted. There would appear to be potential for reducing such exposures through health education and improved packaging and labeling.
Acknowledgments
This study was conceived by Professor DN Bateman and planned by Professor DN Bateman and Mrs Alison Good. Mr RD Adams and Mr D Lupton collected and analysed the data. Mr RD Adams drafted the manuscript and all authors contributed to the final version.
REFERENCES
Footnotes
Mr Richard D Adams, Mr David Lupton, Mrs Alison M Good and Professor David Nicholas Bateman are all based at NPIS Edinburgh in the Royal Infirmary of Edinburgh, Scotland.
Funding: The UK Health and Safety Executive and the Pesticide Safety Directorate funded this study. The funding sponsor had no role in the design of the study other than to request a range of pesticides about which they were specifically interested in gathering exposure data. The study sponsor played no role in the collection, analysis or interpretation of data. The study sponsor also played no role in writing the report or the decision to submit the paper for publication.
Competing interests: None.