Article Text

Abstract
Objectives—To assess and improve deployment of a brief test for alcohol misuse: the Paddington Alcohol Test (PAT).
Design—Prospective study of the effects of audit feedback.
Setting—An urban accident and emergency department.
Subjects—Senior house officers (SHO) (n = 13).
Outcome measurements—PAT use and categorisation of patients for each SHO; observational analysis of presenting complaints according to PAT.
Results—1062 of 1737 patients (61.1%) were defined as PAT possible—that is, presented with ≥ one complaint listed on the PAT test proforma. In month 1, PAT uptake was poor. PAT use improved significantly when feedback was instituted (p<0.0001). The response to audit and feedback showed marked inter-SHO variation. When feedback was withdrawn (month 4), there was a significant reduction in PAT use (p=0.003). Three other indices of detection followed this trend: (a) number of PAT positive patients identified, (b) proportion of PAT possible patients identified as PAT positive, and (c) number of PAT positive patients referred to the alcoholic health worker. The 10 most common PAT positive categories, accounting for 77% of all PAT positive complaints were: fall > collapse (including “fit”, “blackout”) > head injury (including “facial injury”) > assault (including “domestic violence” and `other') > non-specific gastrointestinal problem > “unwell” > psychiatric (including “depression”, “overdose”, “confusion”) > cardiac (including “chest pain” and “palpitations”) > self neglect > repeat attendance.
Conclusions—Ongoing audit with feedback improves both PAT use and detection of alcohol misuse. The PAT is now simpler including only 10 conditions, which should further aid its use.
- alcohol misuse
- alcohol health worker
- Paddington Alcohol Test
Statistics from Altmetric.com
Alcohol misuse is a major cause of mortality and morbidity throughout the UK,1, 2 whether this be directly (pathophysiological, for example: intoxication, hypertension, cirrhosis, cancers) or indirectly (via social harm, for example: road accidents, drownings, child abuse, murders, other assaults, deaths by fire).3–11 The problem is exacerbated by the alcohol accepting culture of the Western world, stigmatisation of the alcoholic and apathy or lack of skills on the part of the doctor,12–14 compounded by denial on the part of the patient.
There are few opportunities for alcohol detection,15 but the accident and emergency department (A&E) is in a potentially pivotal position to detect and refer patients who misuse alcohol.11, 16–18 More patients attend A&E than outpatient departments.19 Attendance at A&E is often for a crisis when patients are more willing to accept help.20 Many of these patients also suffer from the effects of acute or chronic alcohol misuse, or both.21–23 In our area of London (Kensington, Chelsea and Westminster) it has been estimated that 22.2% of people drink in excess of recommended values, compared with 10% nationally.24
In the USA the subject of patients with alcohol problems in A&E has been extensively reviewed,25, 26 the conclusions being very similar to those in the UK: “the ED is an excellent site for brief intervention with problem drinkers; patients are often more receptive to education in the moment of crisis”. However, compared with the Paddington Alcohol Test (PAT) (three questions), the questionnaires used in the USA are either more comprehensive—thus taking longer to complete—for example, TWEAK, AUDIT, Brief MAST, or if as short, such as the four question CAGE, detect only those who are, or who are becoming, dependent on alcohol and not those who are intermittent binge drinkers—that is, hazardous drinkers.
The effectiveness of brief motivational interventions in the treatment of alcohol misuse in patients admitted with an injury was confirmed in a prospective randomised study carried out in a US trauma centre.27 A total of 2524 patients were screened of whom 1153 (46%) met the criteria for alcohol misuse—a figure close to that found in UK studies.28, 29 Of these, 396 were allocated to the control group, and 366 to the intervention group. Of the 391 not entered in the trial, the refusal rate was only 18.6% (215 patients); the other 176 screened positive but were discharged over the weekend (study staff were not available to enter patients into the programme). In the intervention group, alcohol consumption and trauma recurrence were both significantly reduced. As alcohol misuse is the leading risk factor for injury, this study provides further evidence for the efficacy of an A&E based alcohol screening and referral system such as that based on the PAT.
Cherpitel (1993) reviewed international emergency room studies concerning the relationship between alcohol and injuries, and concluded that further research was needed about patients reattending with alcohol related accidents.30 A recent UK survey of A&E departments31 showed that the general attitude of doctors and nurses towards improving the response to alcohol related attendances was positive. The association with alcohol misuse is well documented for some frequent A&E presentations, for example, assault and head injury—especially facial injury.6, 32 Despite this, few A&E doctors routinely inquire about or record alcohol consumption.31, 33
Earlier work in this department has shown that A&E is an appropriate place to consider alcohol misuse, with 46% of detected and referred patients reattending for further help.20 An effective screening questionnaire was developed: the one minute PAT.34 It was designed with respect to ease of use, speed of administration and the identification of patients at an early stage of alcohol misuse. We have shown previously that once detected, using the PAT, and referred to an alcohol health worker (AHW), 65% of the 60% patients who reattended for subsequent counselling reported drinking less at six months, indicating the effectiveness of intervention by an AHW.35 In addition, the earlier alcohol misuse is detected the greater is the success of brief intervention. Young patients are often intermittent binge drinkers,36 that is, hazardous drinkers as compared with dependent drinkers, whose habits are unrecognised by their general practitioners or other agencies (for example, employers). The potential for A&E to detect young hazardous drinkers has recently been confirmed.37 Studies in other environments corroborate the effectiveness of alcohol screening and early intervention.38, 39
At the start of this study, 26 presenting conditions were listed at the top of the PAT proforma. These had been identified previously34 as the most common presentations associated with alcohol misuse and formulated into an easily administered PAT questionnaire (appendix 1). However, the detection rate of alcohol misuse remained low, with a discrepancy between expected and actual AHW referral rates.40 This was disappointing given the success rate for ensuing counselling,20, 35 and the spectre of possible medicolegal consequences if alcohol is not considered as a root cause of A&E.40, 41 We therefore decided to investigate whether audit/feedback increases PAT use, and whether this has an effect on the numbers of patients referred. The effectiveness of audit in improving the detection of excessive drinkers has been documented previously.42 A secondary aim was to establish the numbers of each PAT possible complaint presenting to the department with a view to making the PAT a more efficient tool in the hands of junior medical staff.
Methods
DEFINITIONS AND TERMINOLOGY
(1) The PAT (appendix 1) was used as described previously.34, 35 (2) A patient was described as presenting with a PAT possible condition if (a) a history could be obtained, and (b) a presenting complaint was one listed in the PAT (appendix 1). A patient for whom no history was available (for example, comatose with collateral history not available) or who presented with complaints other than those given in the PAT was deemed non-PAT possible. (3) The minimal criteria for a patient to be coded PAT positive were if (a) they drank more than eight units/day (male) or six units/day (female) on at least one day per week, or (b) the current attendance was related to alcohol. A patient was PAT negative if they replied in the negative to the question concerning units/day and further denied that the current attendance was related to alcohol. A PAT negative coding was derived from the notes if either “PAT negative” was ringed at the top of the clerking proforma or there was documented evidence of an alcohol history being taken, but no indication of an excessive drinking pattern. Thus, in this audit, a PAT possible patient had three possible coded outcomes—(a) PAT not done (= PAT missed) if there was no documentation re alcohol in the notes, (b) PAT negative, or (c) PAT positive.
STUDY DESIGN
The study period (September to December 1998, when an unchanging team of 13 SHOs was employed) was divided into four × four week time periods. Each month contained seven “audit days” at four day intervals. During the first (month 1), no feedback was given, nor were the SHOs aware of the audit. During the second and third months, all SHOs were made aware of the audit and received feedback in two forms: (a) individual feedback (to each SHO) concerning all patients in whom a PAT possible condition was identified but no PAT given (that is, PAT missed), and (b) overall feedback at weekly teaching meetings (attended by all SHOs), as to the predominant missed conditions. During the fourth month, only two of the 13 SHOs (CB and JSH) were aware of the audit. These two SHOs performed the audit categorising each patient who fulfilled the inclusion criteria ((1) address (or NFA) in our area, (2) at least 16 years of age, and (3) seen by A&E SHO) seen in a designated 24 hour period, according to a standard form detailing patient seen, presenting complaints (maximum of three), postcode, PAT possible (Y/N), PAT positivity/negativity/missed, and referral to AHW. Each patient coded PAT positive could have up to three PAT possible conditions.
DEFINITION OF STANDARD ACCEPTABLE
Given the possibility of medicolegal consequences raised by Touquet et al,41 the defined standard, at least for the purposes of this study, was PAT use of 100% for PAT possible complaints. Coupled with the feedback for two months this component of the study fulfilled the criteria for a full audit,43 with closure of the audit loop. Given that the PAT represents a formalised approach to obtaining an alcohol history, it was accepted that phrases such as “EtOH—occ.” in the notes were coded as PAT negative as, though inadequate in terms of PAT phraseology/completeness of an alcohol history, there was at least written evidence of questioning re alcohol use.
STATISTICS
Conventional χ2 testing was used to compare variables expressed as proportions of PAT possible patients.
Results
PAT AUDIT
Over the 16 week study, 1761 patients fulfilled the inclusion criteria for the study (address in our area, at least 16 years of age, seen by A&E SHO in designated 24 hour period). The notes for 1737 (98.6%) of these were found and analysed. In 15 (0.9%) it was not possible to perform a PAT (whether or not alcohol misuse was suspected). The majority of patients (1062; 61.1%) presented with at least one condition defined as PAT possible (appendix 1). Table 1 summarises the data by month.
In month 1, PAT uptake was poor with 61.5% of PAT possible patients having no documentation of alcohol (mis)use in their notes (that is, = PAT missed (ND)). However, when feedback was instituted, uptake was significantly increased (p<0.0001), with the proportion missed (PAT-ND) decreasing in months 2 and 3 successively (fig 1). There was a significant reversal of this effect when feedback was discontinued during month 4 (PAT-ND = 32.6%; p=0.003). The proportions of PAT possible patients identified as PAT positive and PAT negative also increased with feedback. Of PAT possible patients, 35% were identified as PAT negative in month 1 compared with 50.8%, 64.0% and 59.2% in months 2, 3 and 4, respectively. Only 3.4% were identified as PAT positive in month 1, compared with 9.6%, 14.3% and 8.2% in months 2, 3 and 4 (table 1).
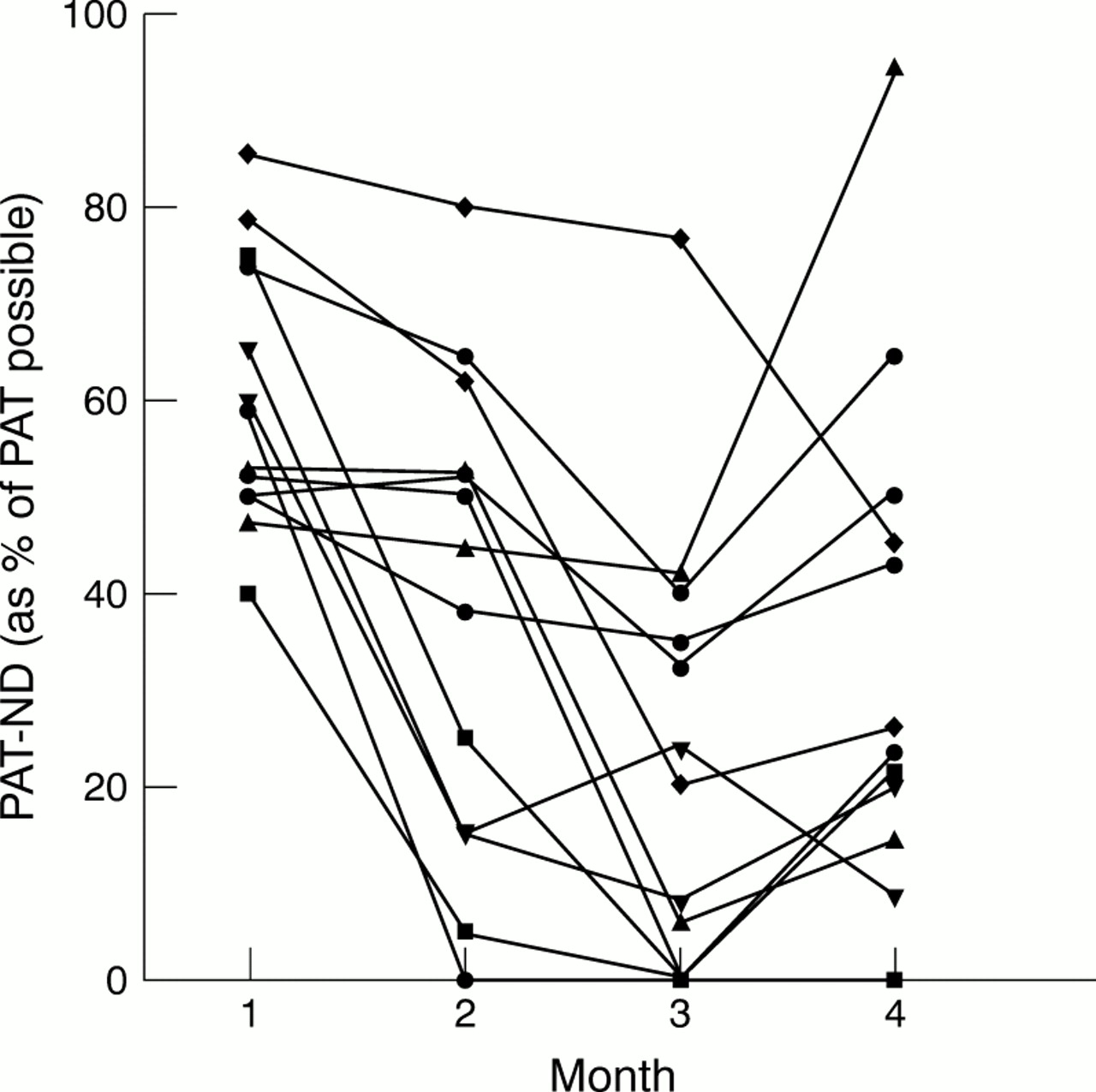
Data concerning %PAT missed for each SHO are given in figure 2. Though audit and feedback improved SHO performance, there was nevertheless marked SHO variability. Therefore on any given day, results are likely to be influenced not only by case mix but also by “SHO mix”.
Figure 3 shows the increase in number of patients identified as PAT positive when analysis was augmented by feedback, and the reversal of this trend when feedback was withdrawn. It also shows the increasing numbers of these patients referred (black bars).
PREVALENCE OF PAT POSSIBLE COMPLAINTS
The most common PAT possible conditions were: fall > non-specific gastrointestinal problem > chest pain > head injury > “unwell” = other (non-domestic) assault. These six complaints accounted for 63.6% of all the PAT possible conditions. Despite re-iteration at feedback of the importance of these PAT possible conditions, they continued to form the bulk of all classes of PAT possible patients, including the PAT missed group.
One weakness of the original PAT (appendix 1) was the large number (26) of PAT possible complaints. It was judged that these could be regrouped into a smaller number of sections. Of the 139 PAT positive patients identified during the study, 77.0% (107) were accounted for by these “top 10” complaints/groupings arranged as follows: fall > collapse (including “fit”, “blackout”) > head (including facial) injury > assault (comprised of “domestic assault” and “other”) > non-specific gastrointestinal > unwell > psychiatric (including “depression”, “overdose”, “confusion”) > cardiac (including palpitations, chest pain) > self neglect > repeat attendance.
Data in table 2 show the PAT positive yield expressed as ratios: (1) (PAT positive/(PAT positive + PAT negative)), and (2) (PAT positive/PAT possible). Column 1 therefore shows the yield of PAT positives as %, wherein the denominator is the number of patients with this presenting complaint that were actually asked about alcohol. Column 2 shows the yield of PAT positives, with the number of PAT possible as denominator. A marked discrepancy therefore, between the two columns for any category indicates that doctors are poor at asking about alcohol for this condition (for example, falls or psychiatric).
Discussion
This study shows the value of ongoing audit with feedback in detection of alcohol misuse within A&E. This process significantly increased PAT use and the identification of PAT positive patients while withdrawal of feedback resulted in decreased PAT use and number of PAT positive patients detected (figs 1, 2, 3). Not surprisingly, there was large variation between SHOs in the number of completed questionnaires over the four month study period, with a trend for fewer reports to be completed at night (when the department is generally busier) than during the day.
Several modifications have been made to the PAT to make it faster to complete and more user friendly. The PAT possible complaints have been reformulated in a revised PAT with 10 PAT possible complaints (fall, collapse (including fits), head injury (especially facial), assault, non-specific gastrointestinal, “unwell”, psychiatric (including overdose), cardiac (including palpitations), self neglect, repeat attender) as compared with 26 (appendix 1). This “top 10” will be printed in future editions of our A&E record to serve as a further reminder to the clinician. The second part of question 2 on the PAT has been removed. All patients who were PAT positive on this criterion, were PAT positive on the basis of question 3 as well—that is, this section of question 2 conferred no additional discriminatory power. Furthermore, it is proposed to make ongoing audit a feature of PAT practice in the department, as withdrawal of feedback caused a reversal of the improvement of PAT uptake. Our study has confirmed that the “top 10” PAT possible conditions seen in central London are similar to the predominant conditions highlighted in studies from Baltimore23 and Los Angeles.11
Table 2 shows derivative data of ratios for the PAT positive yield of each complaint category. The ranking of each category was broadly consistent between the two columns. Repeat attenders were the most likely to be found PAT positive. Conversely and surprisingly, “cardiac” presentations (comprising chest pain, palpitations) had a poor PAT positive yield. Alcohol is known to cause myopathic changes44 and cardiac arrhythmias, but the resulting clinical problems are not common. Some categories such as “fall” are common presentations in A&E frequently associated with alcohol misuse, but the opportunity for screening for alcohol misuse is still often missed. Interestingly, although 51 complaints pertained to road traffic accidents, no such patient admitted to being PAT positive. Legislation for drinking and driving is an example of a recent change in attitudes and practice.45
Patients were asked, in question 1 of the PAT, their maximum daily alcohol consumption, which may underestimate the actual amount drunk. The values of six units for women and eight units for men that we used as a cut off are twice the recommended daily maximum,46 but were chosen empirically as alcohol intake above these values is associated with an increased incidence of facial injuries.6, 8 Our methodology did not review blood alcohol concentrations. Interestingly, Carrigan et al47 demonstrated a significantly higher prevalence for alcohol intoxication in the non-RTA trauma group than the RTA trauma group. We suggest that where a patient is unable to answer questions concerning possible alcohol misuse, then a blood alcohol level should be requested. This should also apply to the non-traumatic conditions listed in the “top 10”.
Despite the generally positive attitudes of A&E medical professionals towards detecting alcohol misuse, and the issue of medicolegal liability if alcohol is ignored as a possible cause for certain complaints,31, 41 there are few examples of alcohol treatment facilities being integrated with A&E departments.15 Indeed, at present we know of only three other UK A&E departments that incorporate AHWs (Hope Hospital, Manchester; Royal Liverpool University Hospital; North Tees General Hospital, Stockton on Tees). We believe this should become universal practice, to minimise missed opportunities for early intervention in the treatment of alcohol misuse.
Part of the role of A&E doctors and nurses is to detect alcohol misuse in a non-judgemental manner, and to encourage the patient to recognise that they have a problem. In this way, patients may become receptive to the idea of self help and want to be referred to an AHW. The role of the trained AHW is to provide counselling. A lack of definition of such roles is, in our view, why other studies have suggested that A&E is a difficult location to motivate drinking patients to alter their habits.48–50
Nationally, it is time to confront the apathy with which the health service in general and A&E in particular regard the detection and treatment of alcohol misuse.51 The fact that more patients present to A&E with a PAT possible than a non-PAT possible condition means that for the “top 10” presentations, the question every doctor should ask themselves is not so much “Should I ask about alcohol?”, but “Can I afford not to ask about alcohol?”.
Appendix 1
Summary data by month. Number of patient falling into each PAT category, by month. The figures in parentheses are % of patients presenting with PAT possible condition(s)
PAT positive yield according to modified complaint groupings

Categorisation of PAT possible patients according to month. PAT-ND = PAT possible but not done.

Individual SHO performances showing PAT-ND (PAT possible patients with PATs not done) as a percentage of their total PAT possible load, according to month.

Number of PAT positive patients according to month. Black area shows number accepting AHW referral.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acknowledgments
We gratefully acknowledge the cooperation and forbearance of all SHOs in “Team 25” and our AHWs including Phillip May, Adrian Brown, BKCW Mental Health Trust. In addition we thank Mr A Duffy and Ms S Wright for access to their internal audit of 1997; Professor J A Henry, Dr T Challoner and Mr S G T Smith for their comments and discussion.
References
Footnotes
-
Funding: none.
-
Conflicts of interest: none.
-
Addendum
-
Updated PATs (PAT 2001) available from R Touquet.