Article Text

Abstract
Objectives: Activated charcoal is now the mainstay of non-specific treatment for self poisoning in accident and emergency (A&E) departments and should be administered within one hour of ingestion of an overdose. This study aimed to investigate if compliance with treatment guidelines may be improved by the prehospital administration of activated charcoal.
Method: Ambulance report forms and case notes were reviewed in all patients presenting to A&E by ambulance after self poisoning. Information was gathered using a standardised abstraction form. The times collected were: time of ingestion, time of call to ambulance control, time picked up, time of arrival in A&E and time seen by doctor.
Results: 201 patient records were reviewed. Twenty six were excluded because of incomplete data on report forms or case notes. The median time between ingestion and pick up by an ambulance crew was 77 minutes. This compares with a median of 140 minutes for the time to assessment by medical staff. Seventy three patients were picked up by an ambulance within one hour of overdose, only 11 (15%) of these were seen by medical staff within an hour of ingestion. Forty nine of these 73 patients would have been suitable candidates to receive activated charcoal.
Conclusions: The prehospital administration of charcoal provides an opportunity to comply with international guidelines on reducing the absorption of a potentially fatal overdose. The administration of charcoal results in few side effects provided the patient can adequately protect their airway and ambulance staff could be trained in its use. Further studies would be necessary to investigate if this would effect clinical outcome.
- charcoal
Statistics from Altmetric.com
Activated charcoal is a preparation commonly used in the first line treatment of overdose in accident and emergency (A&E) departments. Its use can reduce the absorption and aid the elimination of certain drugs by adsorbing the drug in the gastrointestinal tract.1 Recent evidence has lead to more restricted indications for the use of gastric lavage and has rendered the emetic, ipecachuana obsolete.2,3 Both can produce a “wash through” of drug into the duodenum, in theory leading to faster absorption and circulation within minutes.4 Activated charcoal therefore often forms the main, non-specific gut decontamination treatment available in A&E.2
It is advised that charcoal should be administered within one hour of ingestion of a potentially toxic amount of most poisons.1 This objective is difficult to attain because of the time taken to contact emergency services or to transport the patient to hospital where the charcoal can be prescribed. The aim of this study was to assess the proportion of patients in which prehospital administration was feasible, so improving compliance with current guidelines.
METHODS
The study took place in the Accident and Emergency Unit in Raigmore Hospital, Inverness. This unit sees approximately 26 000 new patients per annum and covers a geographical area the size of Wales. The study started in June 1999 and continued for a period of nine months. All patients who were transferred to A&E by ambulance having taken an oral overdose of medication were included in the study. A case note review was conducted with data extracted on a standardised sheet by an unblinded abstractor. Data were collected from emergency department case notes and ambulance records completed at the time of the attendance. Patients were excluded if times were missing from the clinical documents.
The following data were collected: time of ingestion of overdose, time of call to ambulance service, time of arrival of the ambulance, time of arrival in A&E, time seen by doctor, time of charcoal administration. From this, it was possible to calculate the time from ingestion to pick up by the ambulance crew, the journey time to A&E and the time from ingestion to assessment by medical staff. A judgement was made as to whether activated charcoal was indicated in each case by referring to current guidelines from the National Poisons Centre.
RESULTS
A total of 201 patients records were reviewed 26 were excluded because of incomplete documentation of times. The median time between ingestion and pick up by an ambulance crew was 77 minutes (interquartile range, 36 to 204 minutes). This compares with a median of 116 minutes (interquartile range, 61 to 245 minutes) for the time from ingestion to arrival in A&E and 140 minutes (interquartile range, 85 to 264 minutes) for the time from ingestion to assessment by medical staff. The median time from pick up to medical assessment was 49 minutes with a mean of 46 minutes (interquartile range, 32 to 65 minutes). Seventy three (41.7% of all patients) patients picked up within an hour, only 35 (48%) arrived in A&E and 11 (15%) were seen by medical staff within an hour, as illustrated in figure 1.
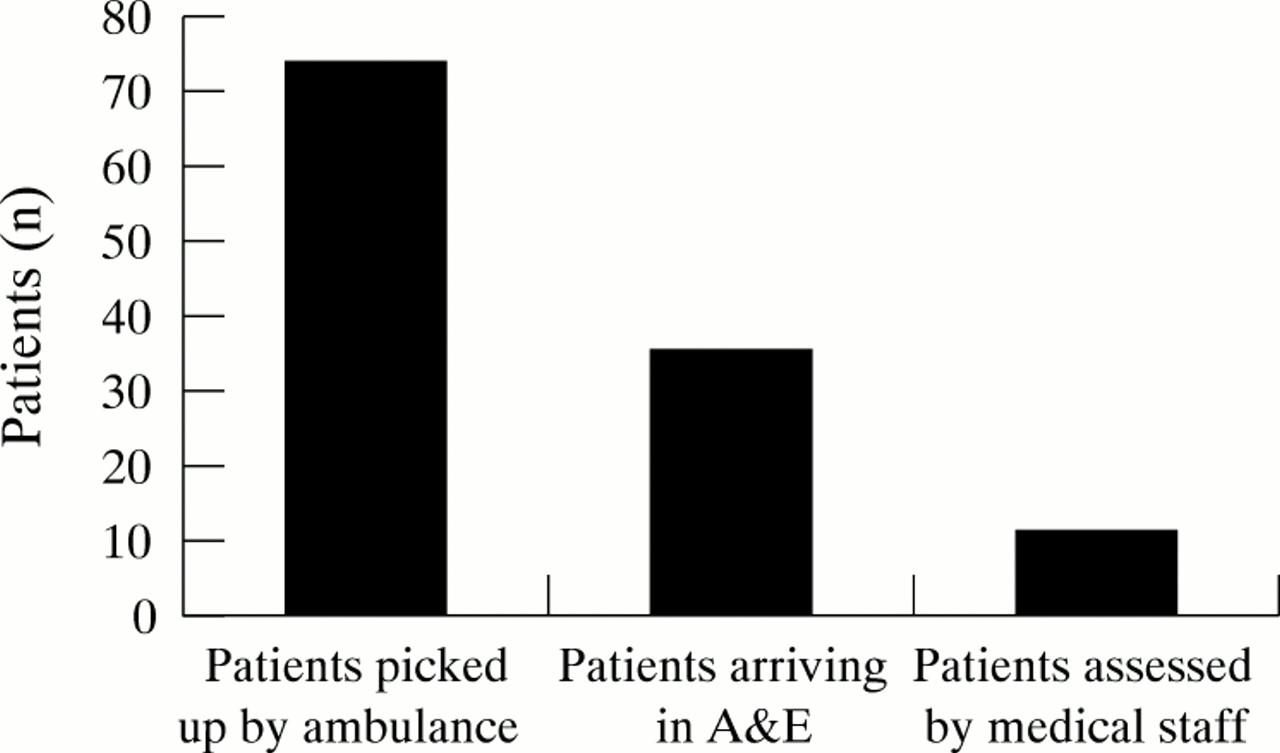
Patients picked up wihin an hour of ingestion of overdose.
Journey times to A&E show a median of 27 minutes and a mean of 29 minutes with an interquartile range of 17 to 40 minutes. Of the 73 patients picked up within an hour of ingestion of their overdose, 49 (67%) would have been suitable candidates for activated charcoal according to National Poison Centre guidelines.
DISCUSSION
Traditionally, the three options for gut decontamination after overdose have been gastric lavage, an emetic or activated charcoal. In recent years evidence has mounted in support of activated charcoal and it is now the mainstay of non-specific, load reduction treatment in A&E departments.1–3 This is the first study to examine the potential role of the prehospital administration of charcoal in the United Kingdom.
Activated charcoal adsorbs a poison in the gastrointestinal tract and therefore reduces its absorption into the systemic circulation. Its use as a method of gut decontamination is supported in the Position Statement of the American Academy of Clinical Toxicology, European Association of Poisons Centres, and clinical toxicologists.1 This suggests that it is administered within an hour of ingesting a potentially toxic overdose. It may also be considered in cases that present over an hour after ingestion, however data on efficacy are insufficient.1 Volunteer studies suggest that activated charcoal reduces absorption of ingested drugs. However, these results may not be applicable to the situation of acute overdose because of: variable delays in the administration of charcoal, differences in the adsorptive properties of charcoal in the empty stomach of a human volunteer compared with the often full stomach of a patient taking an overdose, and variations in pharmacokinetics seen in toxic as compared with therapeutic doses of medication.1 Despite these limitations such studies do provide human in vivo evidence of the effect of charcoal. Clinical studies have suggested activated charcoal is beneficial when used in the context of overdose.5–8 One study showed a 52% fall in the plasma paracetamol concentrations of poisoned patients, the control arm of the study was stopped as paracetamol concentrations rose during the period of the study.7 The other studies had no control group but indicated that charcoal was as effective as other forms of gastric decontamination.5,6,8 The case for prehospital treatment with activated charcoal is supported by volunteer studies suggesting that the sooner it is administered the more beneficial the effect. Mean bioavailability is reduced by 88.6% when a dose of at least 50 g of activated charcoal is administered at 30 minutes after overdose. The reduction is only 37.3% when charcoal is given at 60 minutes after ingestion.1
There may be debate as to the relative benefits of gastric lavage and activated charcoal in the first hour after ingestion. In a separate Position Statement a review of clinical studies involving gastric lavage revealed no conclusive proof of its benefit.9 It is therefore only recommended for potentially life threatening overdose ingested within the preceding hour.9 This more demanding indication and the potential complications of gastric lavage have made it a far less commonly used mode of treatment. Indeed it has been suggested that gastric emptying can be omitted from the treatment of acute oral overdose.5
It would seem that a significant proportion of patients are missing the opportunity for treatment in accordance with the above guidelines. Seventy three patients were picked up within an hour of overdose, however only 11 of this group received medical assessment within one hour. Compliance with the current guidelines could be improved if ambulance personnel were able to administer charcoal. Crockett and colleagues found that the average time from first encounter to administration of charcoal by paramedics was five minutes.10 This compares with a reported mean of 48 minutes for the time from arrival in an emergency department to charcoal administration.11 This study has shown the average time from pick up to medical assessment in our catchment area to be 46 minutes. As charcoal is usually not administered without medical assessment, there could therefore be a saving of 41 minutes if paramedics provided treatment.
Previous studies have shown that prehospital gut decontamination has been attempted. Wax and Cobaugh reported that just 2% of cases in their series received treatment in the prehospital phase.12 However, the method used was the emetic, ipecachuana and the low uptake of treatment possibly reflects the fact that emesis makes patient management difficult. When activated charcoal has been used in the prehospital setting it seemed to be well tolerated by patients.10 There may be concerns over the safety of activated charcoal administration and complications have been noted, ranging from corneal abrasion to pulmonary aspiration.5,6,13,14 However, contraindications are clearly documented, namely, an unprotected airway, a gastrointestinal tract that is not anatomically intact and the few medications that are not adsorbed by charcoal.1 In practice, only patients who are alert, with intact airway protective reflexes having taken drugs amenable to activated charcoal would be candidates for prehospital treatment. A suggested protocol for the prehospital use of charcoal is given in figure 2.

{kind=link}
{kind=link}
A suggested protocol for the prehospital administration of oral acitvated charcoal.
The continued use of activated charcoal will depend on evidence of improved clinical outcome. Prehospital administration has not been a part of previous studies into clinical outcome, however, this setting provides the potential to significantly reduce the interval between ingestion and administration. This could bring greater reductions in bioavailability of the drug,1 in theory leading to improved clinical outcome. To reduce the time interval to administration, greater priority needs to be directed towards the early management of self poisoning. The requirement for medical assessment in hospital before charcoal administration should be questioned. It should be remembered that activated charcoal is not a prescription medication. Treatment should be provided by the first person attending the patient, whether this is the paramedic, triage nurse, nurse practitioner or general practitioner. In conclusion, it may be argued that attention should be paid to the “ingestion to charcoal” time in the same way that “door to needle” times are emphasised in the administration of streptokinase. Further research looking at the impact of early use of activated charcoal on the subsequent need for supportive or interventional treatment may underpin the cost effectiveness of this proactive approach.
Acknowledgments
Contributors: Shobhan Thakore initiated the study hypothesis, developed the abstraction form, collected the data, analysed the data and wrote the paper. Noelle Murphy contributed to the study design, edited the paper and is the guarantor of the paper.
REFERENCES
Footnotes
-
Funding: none.