Article Text

Abstract
Objectives—To evaluate the capability of accident and emergency (A&E) departments in six health regions of England to safely decontaminate casualties exposed to hazardous chemicals.
Methods—In January 1999 a postal questionnaire was sent to the clinical director of all A&E departments in Trent, North and South Thames, South and West, North West and, Anglia and Oxford Health Regions. The questionnaire inquired about characteristics of the department, decontamination facilities and equipment, and staff training. Non-responders were sent a second questionnaire and contacted by telephone if they failed to respond to the second mailing.
Results—308 of 326 departments identified (94%) returned a questionnaire. There was no significant difference in response rate by region (p = 0.99). Analysis was restricted to 154 major departments seeing more than 20 000 new attendances per year. Of these 154 departments, 109 (71%) had a written chemical incident plan but only 55 (36%) maintained a list of nearby industrial chemical sites. Fifty nine departments (38%) stated that members of staff had received training in the management of chemically contaminated casualties in the preceding year. Eighteen departments (12%) possessed the level of personal protective equipment (PPE) recommended for decontamination by the Ambulance Services Association. Ninety six departments (62%) had a designated decontamination room but only seven (7%) of them incorporated all the features generally considered necessary for safe decontamination. Forty one units (27%) had the capability to decontaminate casualties outside of the department either with warm water from a shower attachment or with a mobile decontamination unit. Thirty six departments (23%) had neither a decontamination room nor the ability to decontaminate casualties outside the department. Only 16 units (10%) had both adequate PPE and either a decontamination room or the capability to decontaminate outside the department.
Conclusions—This study has identified deficiencies in the current NHS capability to respond to chemical incidents. To resolve this, nationally recognised standards for decontamination facilities, equipment and training should be formulated, agreed and implemented.
- decontamination
- hazardous chemicals
Statistics from Altmetric.com
Accidents that expose members of the public to hazardous chemicals pose a particular challenge to the health service. A prospective study of chemical incidents attended by the UK Fire Service in 1980 identified an average of three incidents and two casualties per day in UK.1 Also, the Sarin attacks in Japan highlight our vulnerability to terrorism using hazardous chemicals.2, 3 While there are no comprehensive and nationally recognised guidelines on health service requirements for safe decontamination there are well defined expectations and responsibilities.
The NHS Executive guidance on planning for major incidents places a responsibility on acute hospital trusts to “ensure that satisfactory arrangements are in place for the provision of health care to casualties of a chemical incident”.4 Not only is there a duty of care to casualties there is also a statutory duty on hospital trusts as employers to ensure the health and safety of all employees.5 The NHS Executive also states that acute hospital trusts must, “provide the facilities and equipment necessary for staff to fulfil their roles in a safe working environment: these include decontamination facilities (including for the collection and disposal of contaminated waste water) and personal protective equipment”.4
Doubts have been raised about the ability of health services in the UK to fulfil their responsibilities in relation to incidents involving hazardous chemicals.6–8 We are not alone, in the United States it has been observed that “the hospital response to a toxic chemical accident [is] one of the weakest links in the community response”.9 Despite these concerns little quantitative information is available on the capability and capacity of acute hospital trusts to safely manage casualties of chemical incidents. Earlier works do provide limited evidence that accident and emergency (A&E) departments in the UK are poorly prepared to deal with chemically contaminated casualties.8, 10, 11 This study was undertaken to evaluate whether A&E departments in six health regions of England have the capability to safely manage casualties contaminated with hazardous chemicals.
Methods
A questionnaire on decontamination of casualties exposed to hazardous chemicals was designed and piloted by the authors. The questionnaire asked for characteristics of the department including number of new attendances per year, the existence of a chemical incident plan, staff training, decontamination equipment including personal protective equipment (PPE), and indoor and outdoor decontamination facilities. As there are no nationally agreed standards against which to evaluate the decontamination facilities and equipment of a department a variety of sources were used to identify service specifications required for safe decontamination.
The Ambulance Service Association (ASA) has recently published a document detailing the specifications of PPE considered necessary for safe decontamination.12 This has been endorsed by the NHS Executive and was the basis for the questions on PPE.4 Health Building Note 22 of the Department of Health and Social Security outlines recommended features for a decontamination room.13 These recommendations are similar to those in other published literature.14–17 While Health Building Note 22 states that dilution makes collection of contaminated waste water unnecessary, the NHS Executive has designated “the collection and disposal of contaminated waste water” an essential action for acute hospital trusts.4
Some sources recommend that, weather permitting, decontamination should take place outside of the A&E department.12, 14, 15 Questions were therefore included on the ability to decontaminate casualties outside of the department. The Agency for Toxic Substances and Disease Registry in the US has outlined requirements for adapting part of the A&E department into an ad hoc decontamination area.14 Questions were therefore also included on equipment necessary to adapt part of the department into a decontamination area.
A list of all A&E departments in the following six regions of England was obtained from the British Association of Accident and Emergency Medicine (BAEM): North Thames, South Thames, North West, Trent, Anglia and Oxford, South and West.
These regions all hold contracts with the Chemical Incident Response Service, Medical Toxicology Unit, Guy's and St Thomas' Hospital Trust. In January 1999, the questionnaire and a covering letter were sent to the clinical directors of the 326 A&E departments identified. Departments that had not responded after four weeks were sent a second questionnaire and a reminder letter. After a further five weeks those who had still not returned a completed questionnaire were contacted by telephone.
The entire dataset was independently entered into two data files (EPI-INFO version 6.0) by two information officers at separate sites (double data entry). All fields were compared between the two datasets and inconsistencies checked against the original questionnaire by one of the authors (PH). Statistical analysis of response rate by region was done using a χ2 test for contingency tables.
The BAEM Directory 1998/99 was consulted to find out the number of new attendances per year for those departments that did not return a questionnaire and those that did not provide this information.
Results
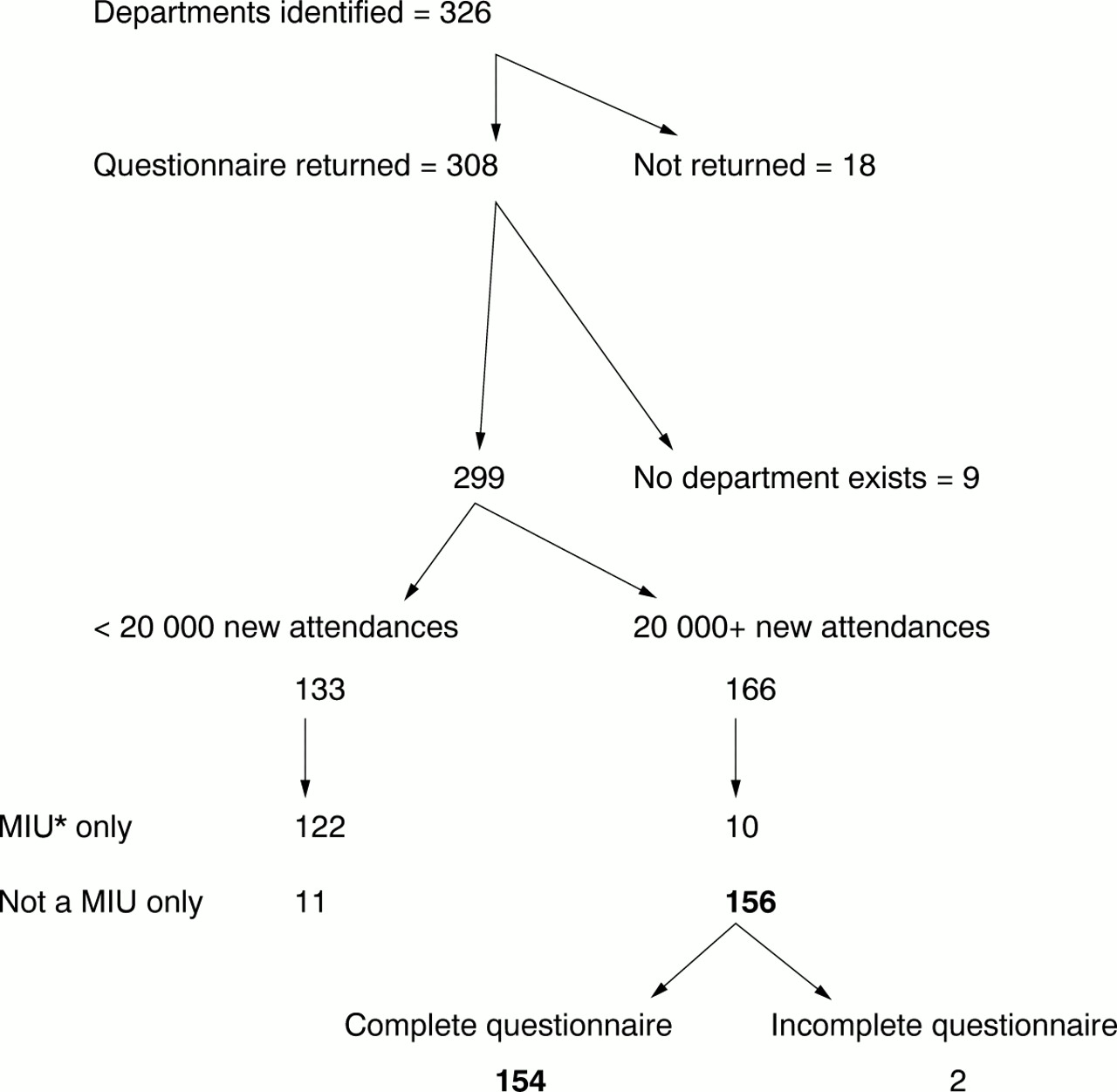
Three hundred and eight of the 326 departments surveyed (94%) returned a questionnaire. There was no significant difference in response rate by region (p = 0.99). Nine questionnaires were returned with a note stating that the hospital was closed or that there was no A&E department or minor injuries unit at the hospital. Of the remaining 299 departments many were minor injuries units, which might not be expected to be able to decontaminate victims of chemical incidents. Analysis was therefore restricted to the 156 departments that had 20 000 or more new attendances per year and that did not describe themselves as a “minor injuries unit only” (fig 1). Two of these 156 units returned incomplete questionnaires and these have been excluded from the analysis. The 154 units included in the analysis are termed “major units” in the rest of the paper.
{kind=link}
Summary of response rate and characteristics of responders. *MIU = minor injuries unit.
Of the 18 units that did not return a questionnaire, five saw 20 000 or more new attendance per year and 13 less than 20 000 new attendance per year. Therefore, in the six regions a total of 161 units could be identified that see 20 000 or more new attendances per year and are not minor injuries units; 156 that returned questionnaires and five that did not. Of these, 154 (96%) are included in the results.
Of the 154 major units 109 (71%) had a chemical incident plan of which 38 (35%) had exercised this plan in the preceding 18 months. Fifty five units (36%) maintained a list of local industrial chemical sites. Fifty nine units (38%) indicated that members of permanent staff had received training in the management of chemically contaminated casualties in the preceding 12 months. Fifty two units (34%) reported that during 1998 staff members had been involved in managing casualties contaminated with a hazardous chemical.
One hundred and thirty nine departments (90%) had protective goggles and 93 (60%) had protective boots. Sixty three departments (41%) had chemical protective over-suits but in only four did the suits have integral boots as recommended by the ASA. Fifty three (34%) had protective gloves other than latex examination gloves and 25 (16%) had an air purifying respirator with chemical cartridges. Only 18 departments (12%) had protective gloves and over-suit and footwear and an air purifying respirator. This is the level of protection recommended by the ASA for patient decontamination.12 The number of departments equipped with this level of PPE is shown by region in table 1.
Personal protective equipment in major units by region
Although the questionnaire did ask if the PPE conformed to the specifications recommended by the ASA these questions were extremely poorly answered. This probably reflects either the time taken to check equipment specifications or lack of awareness of the guidelines.
Ninety six of the major units (62%) had a room designated for decontamination and of these 64 (67%) were purpose built for decontamination. As might be expected, and as is suggested in Health Building Note 22, 76 (79%) of the decontamination rooms are used for purposes other than decontamination.
The 96 designated decontamination rooms did not all possess the features commonly recommended for safe decontamination (table 2). Only 10 decontamination rooms (10%) possessed all the following features; their own entrance from outside and a separate exit to the department, sufficient space to treat a casualty on a stretcher, a shower and a ventilation system independent from the rest of the department. Only seven decontamination rooms (7%) had all the above features and also the facility to contain contaminated water.
Attributes of designated decontamination rooms
Those completing the questionnaire were asked if their department had the ability to decontaminate casualties outside of the department either with warm water from a shower attachment or with a mobile decontamination unit. Forty one of the 154 major units departments (27%) had this capability (table3).
Capability of major units to undertake decontamination outdoors
Thirty six of the 154 major departments (23%) had neither a decontamination room nor the ability to decontaminate casualties outside the department (table 4).
Indoor and outdoor decontamination facilities
Although not recommended and of questionable safety, when decontamination facilities are not available it may be possible to improvise a decontamination area in part of the main A&E department. In the event of this being necessary, 23 of the 58 departments without a decontamination room (40%) had plastic sheeting to cover the floor to minimise secondary contamination of the department. Of the 36 departments with no decontamination room or outside decontamination capability only 12 (33%) possessed plastic sheeting to minimise secondary contamination. Thus 24 major units (16%) have no decontamination room, no ability to decontaminate outside the department and cannot safely improvise a decontamination area. Only 16 units (10%) had both adequate PPE and either a decontamination room or the ability to decontaminate outside the department.
Discussion
When evaluated against available recommendations it seems that many major A&E departments in the six regions surveyed are ill prepared to deal safely with patients contaminated with hazardous chemicals. Many do not have the facilities to decontaminate without risking secondary contamination of the department and very few possess the level of personal protective clothing recommended by the ASA for decontamination. There is also evidence that staff training is infrequent, which, even in a fully equipped department, may result in an inadequate response. Even worse, inadequate training may result in injury or equipment failure.18
The deficiencies identified are not compensated by better provision elsewhere in the emergency service structure. Most ambulance trusts are not equipped to decontaminate casualties.12 The fire service cannot be expected to decontaminate casualties as they may have other priorities and their equipment is designed to decontaminate ambulant firemen wearing full PPE.
We contacted all A&E departments in the six regions and had a very good response rate, partly we believe because of the interest in this subject. The response rate from the major units was particularly high. It is therefore probable that our results are representative of the true picture in the six regions and possibly elsewhere in the UK. Analysis was restricted to the 154 major units identified because to include the smaller units would have biased the results towards a more unfavourable outcome.
The questionnaires were addressed to the clinical director of the A&E department but it was often unclear if the questionnaire was completed by that person. This is because the free text field asking for the name and grade of the person completing the questionnaire was frequently left blank. However, this field was completed for 52 of the 154 major units and 35 of these (67%) were completed by A&E consultants and 15 (29%) by a nurse.
We have identified a gap in the NHS capability to respond to chemical incidents. This has long been suspected but can no longer be ignored. The NHS guidance on planning for major incidents is very clear, both health authorities and acute hospital trusts have a responsibility for ensuring that arrangements are in place for managing victims of chemical incidents.4 These arrangements must protect the patient, health care staff and the functioning of the department.
Current NHS guidance designates clear responsibilities in relation to decontamination but does not detail service requirements. Until clear and detailed standards exist together with an explicit obligation to meet them, resources and effort are unlikely to be diverted from competing priorities into improving the service.
There are several options for improving the current provision for decontamination, only one of which entails fully equipping every major A&E department. Policy makers need to assess the cost effectiveness of the alternatives and come to firm conclusions. Part of this process should involve a transparent appraisal of the level of acceptable risk. Although the optimum service is liable to be sacrificed for affordability and feasibility, we feel it is improbable that the status quo constitutes an acceptable risk. A disaster has been defined as “a catastrophic event which, relative to the manpower and resources available, overwhelms a healthcare facility”.19 For the time being it seems that little stands between a chemical incident and a chemical disaster.
Acknowledgments
Contributors
Peter Horby was responsible for designing the study protocol, questionnaire and database. He coordinated the study, checked data quality, undertook telephone follow up and interviews, analysed the data and wrote the paper. Peter Horby is the guarantor of the paper. Virginia Murray, Amelia Cummins and Kevin Mackway-Jones were responsible for the study concept, critical input into the design of the study and questionnaire, and critical revision of the paper. Rico Euripidou contributed to the study design and participated in study coordination and data collection.
We would like to acknowledge the valuable assistance of Nina Ndubuisi and Rhysian Morgan.
Footnotes
-
Funding: none.
-
Conflicts of interest: none.