Article Text

Abstract
Volar dislocation of the metacarpophalangeal joint is a very rare clinical finding. A volar dislocation of the metacarpophalangeal joint of the left index finger in a 44 year old man is reported. Closed reduction proved unsuccessful requiring subsequent open reduction and internal fixation via a combined dorsal and volar approach. The presentation, mechanism of injury and treatment of this case and other previously reported cases are discussed.
- vovar dislocation
- metacarpophalangeal joint
Statistics from Altmetric.com
Volar dislocation of any metacarpophalangeal joint (MCPJ) is rare in comparison with its dorsal equivalent, which was described by Kaplan in 1957 and subsequently by other groups.1–3 Only nine cases of volar dislocation of the MCPJ have been described in the English medical literature.4–10
The condition is classified as simple if closed reduction is successful, or complex, if open reduction is necessary to overcome soft tissue interposition.7 We present a further case of volar MCPJ dislocation of the index finger and its management following a hyperflexion injury that has only been reported as a cause once before.5
Case report
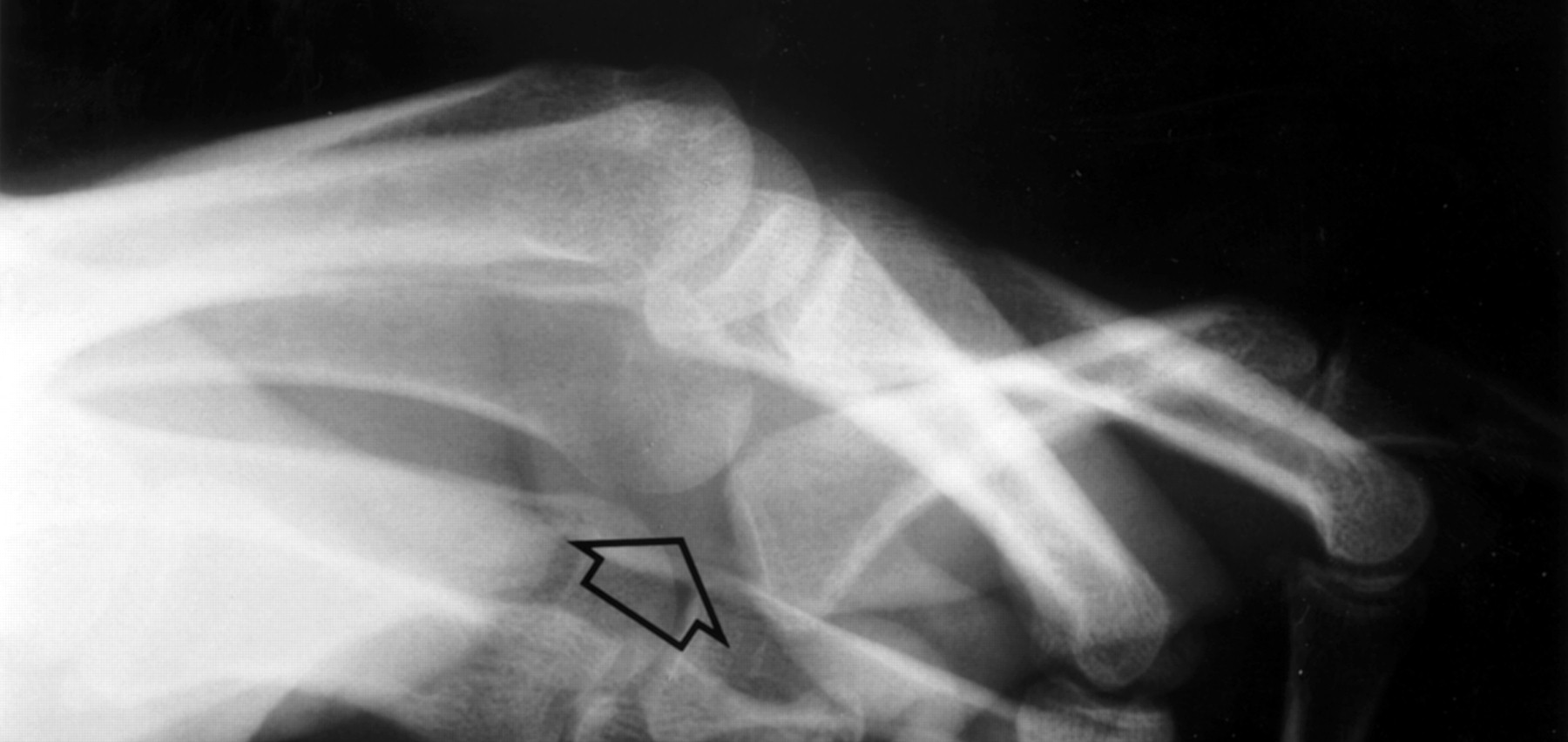
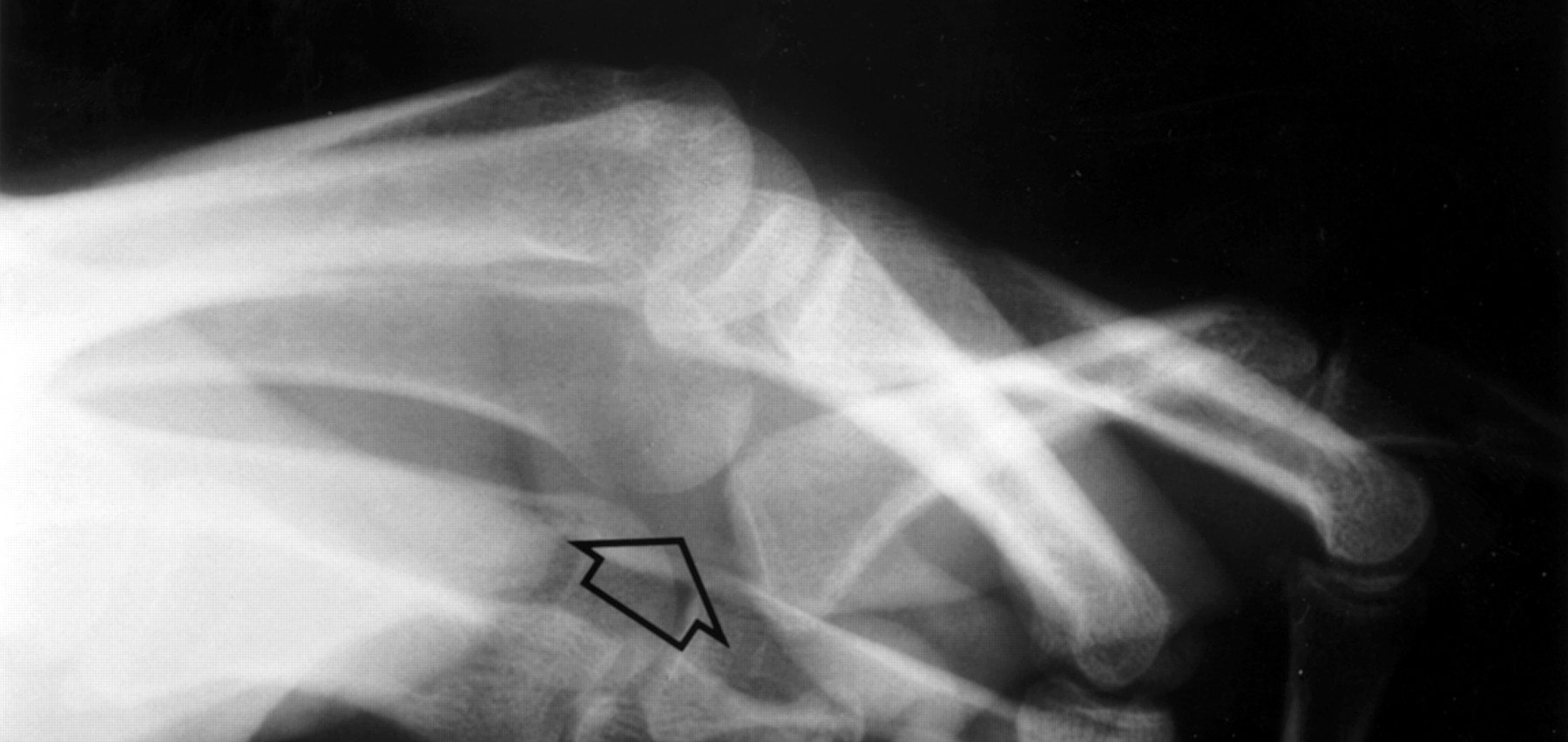
A 44 year old right handed labourer presented to the accident and emergency department having fallen onto his outstretched left hand sustaining a hyperflexion injury. He complained of swelling and tenderness over the base of the left ring finger plus paraesthesiae and decreased movement in the digit. Examination revealed loss of bony prominence of the left ring knuckle and no movement at the MCPJ but normal movement in the joints distal to this. Radiological examination revealed volar dislocation of the left ring finger MCPJ associated with a minimally displaced fracture of the base of the proximal phalanx (fig 1). All other hand and wrist examinations were normal.
{kind=link}
Lateral view radiograph of the left hand demonstrating volar dislocation of the ring finger metacarpophalangeal joint (indicated by arrow).
An immediate successful closed reduction was performed using inhalational anaesthesia being confirmed on radiological examination. The left ring finger was neighbour-strapped and the patient returned the following day when reduction was maintained. A week later, the patient complained of pain and stiffness around the left ring finger MCPJ. Examination revealed a maintained reduction and physiotherapy started. At three weeks after injury, once again there was loss of prominence of the left ring knuckle and a protuberance on the volar surface. Check radiography revealed a recurrent volar MCPJ dislocation and slight displacement of the fracture at the base of the proximal phalanx.
It was decided to correct the deformity by open reduction and internal fixation. Under general anaesthesia, a dorsal incision revealed the presence of scarring around the capsule and collateral ligaments. There was callus formation surrounding the base of the proximal phalanx and incongruity of the articular joint surface. Reduction of the MCPJ proved impossible by this approach alone so that a volar incision was made. This revealed an interposed volar plate within the MCPJ. After partial resection of the volar plate, reduction of the MCPJ was possible. The joint and fracture were fixed using an intra-articular k-wire. Three weeks later, the k-wire was removed and two months later there was no recurrence of deformity with 10–90 degrees of flexion at the MCPJ and full movement of the proximal and distal interphalangeal joints.
Discussion
The reports of volar dislocation of any MCPJ are rare. To date, nine cases have been reported.4–10
The mechanism of injury has been reported as hyperflexion in five patients, hyperextension in three and unreported in one. The management has been by a dorsal approach in five, combined dorsal and volar approach in two, closed reduction in one and unreported in the other.4–10
Normally, dislocation of the MCPJ is prevented by both the shape and supporting structures surrounding the joint. The MCPJ is a condyloid joint whereby the metacarpal head is narrowed dorsally and flares in a volar direction giving increasing contact with the base of the proximal phalanx as the joint is flexed. The capsule of the MCPJ extends from the neck of the metacarpal to the base of the proximal phalanx but is strengthened on all sides. Dorsally, there is a loose insertion of the common extensor tendon. The volar surface of the joint capsule is supported by the volar plate, which has a thick fibrocartilaginous distal portion and a thin membranous proximal portion. The volar plates are linked laterally by the intervolar plate ligaments. The lateral margins are also reinforced by collateral ligaments, which are more taut in flexion than extension. The saggital bands of the palmar fascia and tendons of the intrinsic musculature of the hand provide further support. The MCPJ joint is thus most stable laterally in full flexion but allows abduction and adduction in extension.
Two theories have been proposed as to the mechanism of volar dislocation of the MCPJ. Renshaw and Louis (1973) proposed that hyperextension of the MCPJ produced interposition of the volar plate, between the metacarpal head and base of the proximal phalanx, after rupture of its proximal membranous portion thereby preventing closed reduction.11 However, Wood and Dobyns (1981) proposed that hyperflexion of the MCPJ with simultaneous proximal displacement of the proximal phalanx occurred resulting in interposition of the dorsal capsule into the MCPJ preventing closed reduction.5 Furthermore, they performed cadaveric studies in which they applied hyperflexion and hyperextension forces to the proximal phalanx. In 5 of 10 hyperflexion injuries they reproduced interposition of the dorsal capsule but no cases after a hyperextension injury out of 16 investigated digits.5 It is probable that the actual mechanism is a combination of the two processes, as in this case the dorsal capsule was attenuated and scarred plus interposition of the volar plate requiring partial resection.
In this case, an initial closed reduction was performed with temporary success. In only one previous case has initial closed reduction proved successful without internal fixation eventually.8 Open reduction is necessary because of soft tissue interposition, which in this case was attributable to the volar plate.
Previous reports recommend an initial dorsal approach to the MCPJ as soft tissue interposition usually occurs on the dorsal aspect.7, 10 Occasionally, interposition of the volar plate occurs and cannot always be remedied via the dorsal approach. A subsequent volar approach is then necessary to achieve reduction.
From our experience and that of others, it is probable that simple closed reduction in the accident and emergency setting may prove difficult or impossible because of soft tissue obstruction. If reduction is unsuccessful, referral to the hand surgery service is required to release soft tissue interposition. A dorsal approach, based on the previous cadaveric studies, should be attempted first, before a volar approach if suspected that the volar plate is involved. Furthermore, even if reduction is successful, referral to the hand surgery service is recommended, because of the likelihood of recurrent dislocation resulting from stretching of the joint capsule and surrounding ligaments. In this scenario, internal fixation of the MCPJ will be required.
Acknowledgments
Contributors
Wee Leon Lam identified the rare nature of the case, initiated the case report and contributed to the writing of the case report. Aidan Fitzgerald took charge of researching and writing the case report. Geoffrey Hooper was the surgeon who operated on this case and continued the patient's management as an outpatient as well as editing the case report.
Guarantor
Mr Geoffrey Hooper, FRCS, Consultant Hand and Orthopaedic Surgeon and editor of British Journal of Hand Surgery.
Footnotes
-
Funding: none.
-
Conflicts of interest: none.