Article Text

Abstract
Objectives—To study the current practice of rapid sequence intubations (RSIs) in four different emergency medicine training programmes in the UK.
Methods—Observational study design involving four regional training programmes (Wessex, North West, Yorkshire, Avon). Data were collected in real time using a previously piloted survey tool. Data were collected by specialist registrars in emergency medicine over a continuous 28 day period. Data collected included: indications for RSI; key timings of RSI procedures; details of RSI practitioner; complications and outcome of procedure.
Results—Data from 60 RSIs were recorded and collected. The majority of decisions to perform RSIs were made by emergency physicians (74% cases). Over 50% of the RSIs occurred after 4 pm. Emergency physicians performed 26% of RSIs although the majority were performed by anaesthetists. Most of the given indications for RSIs were based on an assessment of airway protection. Hypoxia was an uncommon reason for RSI in this study (5%). In two thirds of cases the time taken from the decision being made to perform an RSI, to the achievement of successful intubation, was greater than 20 minutes. No failed intubations were recorded, although six other complications (all minor problems) were recorded. There was no significant difference in the response times between anaesthetists and emergency physicians.
Conclusions—This study shows that emergency physicians are currently performing RSIs in emergency departments in the UK. It also suggests improvements could be made to patient care. In particular, standards of care should be agreed for the provision of RSI in the emergency department, including the personnel involved and the appropriate training of individuals. RSI activity in emergency departments in the UK should be audited nationally using an agreed audit tool.
- rapid sequence intubation
- anaesthesia
Statistics from Altmetric.com
Safe effective airway management in critically ill or injured patients is the cornerstone of resuscitation. Rapid sequence intubation (RSI) represents an important element in this process. It is defined as the virtual simultaneous administration of a potent sedative agent and neuromuscular blocking drug to facilitate tracheal intubation.1 By providing unparalleled access to the airway, and superior protection against adverse effects such as aspiration, RSI is the fastest and safest way of securing a definitive airway.
The aim of this survey was to examine the current practice of RSI undertaken in emergency department resuscitation rooms in four different emergency medicine training programmes. For the purpose of this survey RSI was defined as the use of drugs to facilitate endotracheal intubation.
Method
A survey tool for rapid sequence intubation was developed and piloted at Southampton General Hospital (appendix 1). Four training programmes were recruited (North West, Wessex, Avon, Yorkshire). A lead consultant and specialist registrar were identified for each programme. Consultants in each of the training accident and emergency (A&E) departments were asked to approach the lead clinicians responsible for emergency medicine and anaesthetics/ITU in each hospital and seek agreement to participate in the survey. Hospitals within the specified regions were selected with the only inclusion criteria being that the hospital had specialist registrars in emergency medicine.
Data were collected by specialist registrars in emergency medicine only when they were present in the emergency department for a seven day pilot period followed by 28 consecutive days (regardless of holidays or secondments). The data collected are summarised in the box. No alterations were made to the survey tool following the pilot analysis. Data were collected in real time and only on cases where the A&E SpR was present during the RSI. There were no other exclusion criteria in this survey.
Ethical approval was not needed because this was a descriptive study of current practice. The lead specialist registrar for each training programme was responsible for the distribution of the survey tool, training in data collection and collection of completed data sheets. Results and responses from the pilot period were analysed to identify problems before starting the main survey. The final data were collected and analysed using an Excel database.
Results
Details of 60 RSIs were recorded by 27 SpRs over a one month period. The mean age of the patients was 42 years (range 6 months to 85 years) of which four cases were aged less than 10 years old. The RSIs were all performed by anaesthetists in these four cases. The male to female ratio was 1.7:1. Interestingly 50% of cases arrived in the emergency department after 4 pm.
The results from the analysis of both the decision making process and the nature of the RSI practitioner are shown in tables 1 and 2. The clinical indications for RSI are recorded in table 3. A wide variety of medical conditions precipitated the need for an RSI (table 4). Table 5 shows the induction and paralysing agents used. Only five RSI cases were performed by a consultant (8%). On five occasions more than one anaesthetist was present during the procedure.
Results by specialty
Results by seniority
Indications for RSI (more than one indication was often given)
Conditions precipitating the need for an RSI
Drugs used during RSI
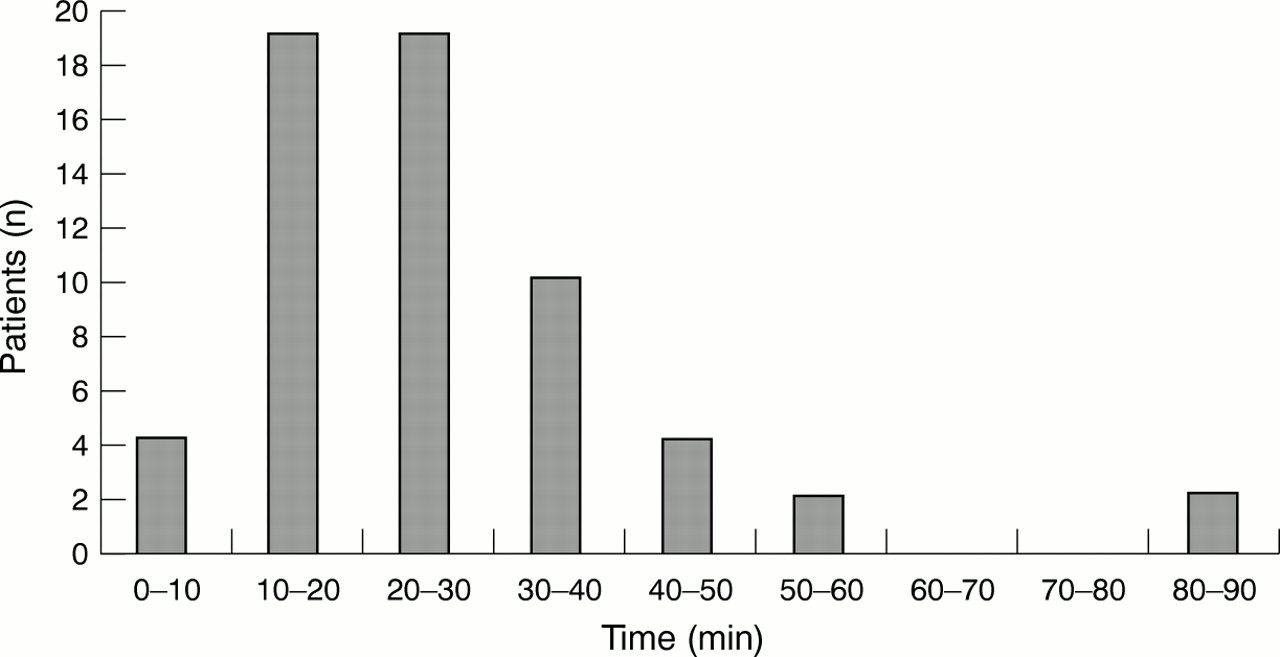
The median time from arrival of the patient in the emergency department to the decision being made to do an RSI was 20 minutes (fig 1). The time from the decision being made to the arrival of the RSI practitioner is shown in figure 2. In two thirds of patients it took up to 20 minutes to successfully intubate the trachea from the time the decision was made (fig 3).
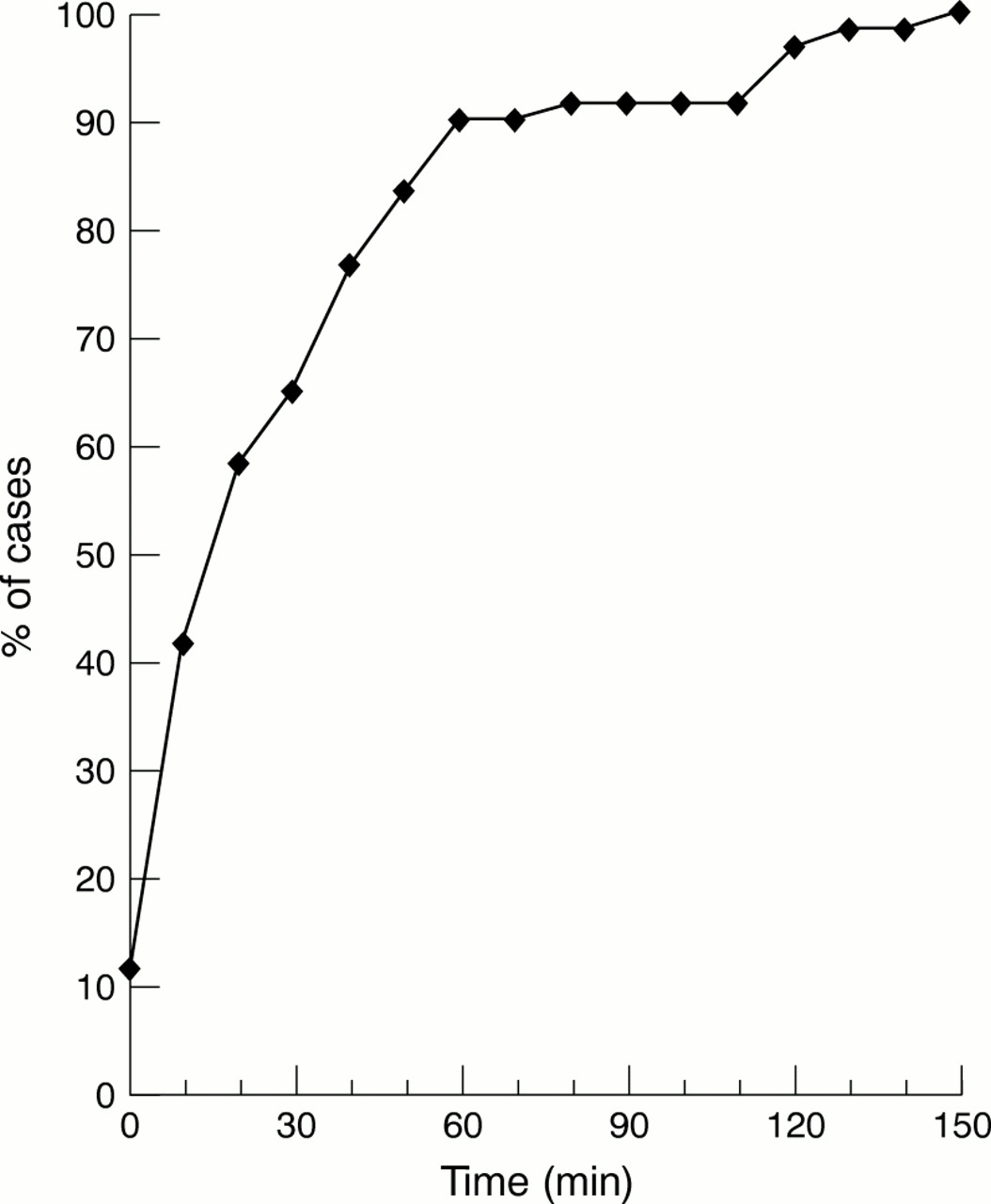
Cumulative frequency curve showing the time from arrival to decision to do RSI.

Time from decision made to do RSI to arrival of RSI practitioner (59 cases).
Time taken from decision to do RSI to securing tracheal intubation.
All intubations were successful. In no patient was a failed intubation drill carried out. Difficulties with drugs/equipment occurred on two occasions causing delays. In one case there was a delay waiting for a drug, and on another, a bougie was unavailable. The tracheal intubation was recorded as “difficult” on two occasions.
In six cases complications were reported of which there were two episodes of desaturation (Sao2<85% during intubation attempt). The other complications included: three episodes of hypotension (defined as a decrease in systolic BP < 90 mm Hg), and one post-RSI cardiac arrest. The aetiology of the cardiac arrest was most probably related to the underlying cardiac problem and not the RSI, but it included here for completeness. For these six episodes the specialty of the RSI practitioner was an ITU/anaesthesia specialist in three cases but was not recorded in the remaining cases.
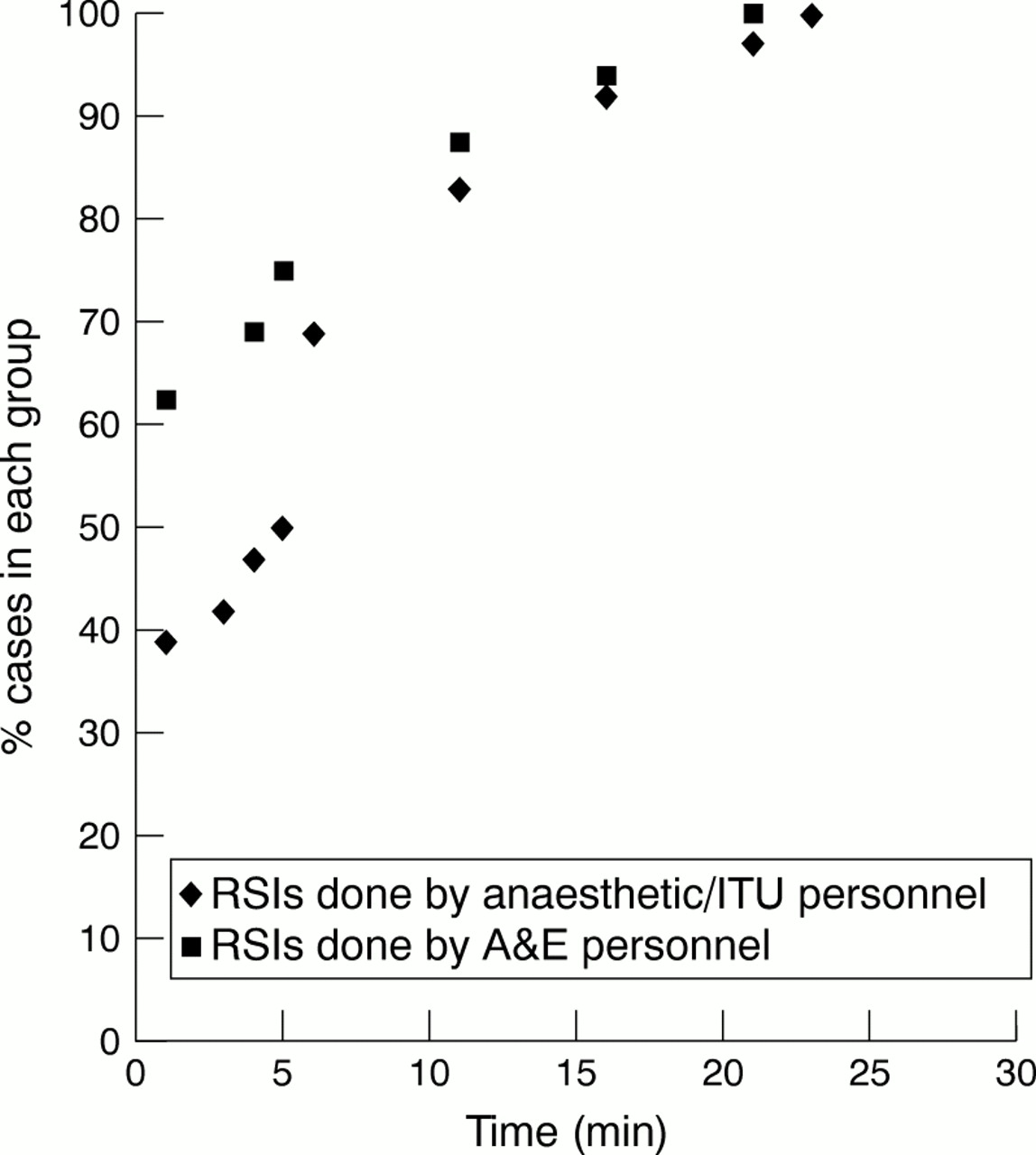
Figure 4 demonstrates the response times from the decision being made to perform an RSI to the arrival of the RSI practitioners. In 10 of 16 patients (62%) in whom the RSI was performed by emergency physicians, the RSI practitioner arrived in the department within five minutes. In the 35 cases in which the RSI was performed by the anaesthetic/ITU specialist, the RSI practitioner arrived in the department within five minutes on 18 occasions (51%). The mean response times were 5 minutes 42 seconds in the ITU/anaesthetic group and 3 minutes 52 seconds in the A&E group. Analysis using a Mann-Whitney U test (Excel) found no significant difference between the two groups (p=0.17).

Time from decision made to arrival of RSI practitioner.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
The goal of this survey was to gain a better understanding of current RSI practice in UK resuscitation rooms. From the analysis of the data collected we estimate that, in a typical month, an SpR in emergency medicine will be involved in the management of two patients requiring RSIs, a significant proportion of which will occur after 4 pm. The study found that A&E specialists (mainly SpRs) decided who needed an RSI in 72% of the recorded cases. Table 1 shows that the majority of indications related to the assessment of the airway and Glasgow Coma Scale. There was agreement in most cases between emergency physicians and anaesthetists with regards to airway assessment. This finding is in contrast with previous reports that have suggested a high incidence of inappropriate assessment of the airway in emergency departments.2 Further work is needed in this area to establish precise indications for airway intervention.
The time from the decision being made to the arrival of the RSI practitioner (see fig 2) was greater than 10 minutes in 20% of cases. In 53% of cases the RSI practitioner arrived within 2.5 minutes. The RSI practitioner came from the specialty of ITU/anaesthesia in 35 cases (58%) and from emergency medicine in 16 cases (26%). The vast majority of RSIs were performed by specialist registrars (62%). Subgroup analysis of RSIs performed by anaesthesia/ITU showed that in more than 50% of cases the practitioner arrived in the emergency department within five minutes of being called, however in 25% of cases there was a delay of over 10 minutes before their arrival. Our data suggest that up to 60% of this subgroup of patients had an airway at risk requiring urgent protection. This finding raises the question of whether accepted standards should be agreed for RSI practitioner response times in emergency patients. A previous survey of consultants in emergency medicine in 1995 reported that 31% of responders had had previous difficulties obtaining an anaesthetist.3
The majority of RSIs were performed because the airway was felt to be at risk (32% of patients had GCS<8), rather than because the patients required ventilation for hypoxia. This finding is supported by work looking at the incidence of hypoxia in trauma patients with a GCS<8 (C R Fitzsimmons, et al, annual scientific meeting of the faculty of accident and emergency medicine, London, December 1999). The majority of comatosed patients were not hypoxic and RSI was needed for reasons other than the correction of hypoxia. Assessment of the airway reflexes is controversial. Moulton et al4 suggested that airway reflexes are not related directly to the GCS and that even at low levels of GCS reflexes may remain intact. Airway assessment will continue to be debated, although GCS<8 remains a widely accepted indication for RSI.
The RSIs were performed mainly for medical indications (table 4), the commonest category being in patients who had taken an overdose. No clear guidelines exist on the indications for RSI in these patients. These results compare with previous observational studies from the USA.5,6 Trauma accounted for 21 of 60 cases with the vast majority of RSIs being carried out in patients with head injury. All these patients were intubated with manual in line stabilisation of the c-spine, thereby increasing the number of personnel involved and arguably, the likehood of potential complications during the RSI (a higher incidence of difficult intubations).7
RSI is not without risks. The drugs used have the potential to turn an urgent airway problem into a life threatening situation. In this study a wide variety of drugs were used during the RSI with all patients receiving a neuromuscular blocker before intubation. In line with UK practice no patients received pretreatment with either lignocaine (lidocaine) or defasciculating doses of neuromuscular blockers before induction. During the study six complications were reported, of which two were episodes of desaturation (Sao2<85% during intubation attempt). Our recorded complication rate of 10% is similar to that reported elsewhere.5,6 It reflects the rates reported by the National Emergency Airway Register (NEAR) group (11.6%) with the majority being minor problems.8 No failed intubations were recorded in our study, reflecting the high rate of successful intubation found in US studies.5,6,8–11 In the NEAR series of 596 cases, 97.8% of patients were successfully intubated in less than three attempts.
This survey is open to potential bias. The data were collected by people directly involved in the treatment of the patient (occasionally the person performing the RSI). Consequently, the potential exists for the underreporting of complications. The data are also open to selection bias, as there was no independent verification of the data collection. It is possible that RSIs were missed or preferentially recorded by the investigators. However, despite these problems, the SpRs were shown to be reliable recorders during the original pilot stage. Only immediate complications were recorded in the study. No follow up was arranged and factors relating to complications were not studied in detail.
This observational study shows that emergency medicine specialists can and are currently performing RSIs in the UK (26% of recorded cases in this study). It also suggests that the provision of care to patients requiring an emergency RSI could be improved. The defining characteristic of emergency medicine is the rapid application of lifesaving measures. Airway management remains the first priority in resuscitation and is critically important to the outcome of these patients.
In its growth as a specialty emergency medicine has frequently faced claims that certain procedures should not be performed or certain drugs should not be administered in the emergency department. One such area is the use of procedures and drugs previously limited to the practice of anaesthesia.12 There is no reason to believe that the drugs and procedures used by anaesthetists could not be safely used by emergency physicians providing that they possess sufficient training. Clarification is still needed on the necessary length and type of training required for a doctor to become “RSI competent”. The American College of Emergency physicians released a statement in 1997 on the topic of RSIs in which they stated that: “RSI is in the domain of emergency medicine practice. Physicians performing RSI should possess training, knowledge and experience in the techniques and pharmacological agents used to perform RSI. Neuromuscular blocking agents and appropriate sedative and induction agents should be immediately available in the ED and accessible to all physicians who perform RSI in the ED”.13 Increasingly RSI is becoming a technique used by emergency physicians. Graham et al reported a survey in which 47% of emergency physicians had used drugs to facilitate intubation in the past one month (C A Graham, et al, annual scientific meeting of the faculty of accident and emergency, London, December 1999).
The body of literature supporting the safety of RSI in the hands of emergency physicians is relatively small. Dufour et al in the USA10 retrospectively studied 219 cases of RSI. All patients were successfully intubated. Aspiration occurred in three patients, hypotension in 24 cases, and arrhythmias developed in three cases. They concluded that RSI is safe and effective in the hands of emergency physicians. Walls et al8 in the first report of the National Emergency Airway Registry (NEAR) reported success rates and complications with 596 intubation attempts from seven centres. Oral intubation with neuromuscular block was the technique used in 77% of intubations. The first intubation attempt was successful in 82.2% of cases with intubation achieved in less than three attempts in 97.8% of cases. The majority of the RSIs were performed by emergency physicians. Their overall complication rate was 11.6% with the majority of complications being minor. Calderon et al9 prospectively analysed 324 patients undergoing intubations at an emergency medicine residency, and found that 99% of cases were successfully intubated by emergency physicians. The overall complication rate was 13%. Sakles et al6 prospectively studied 515 patients requiring an RSI in the emergency department over a one year period; 93% of these were performed by emergency medicine personnel with a complication rate of 8%. Mackay et al found RSI to be safe and effective procedure in the hands of appropriately trained emergency physicians in the prehospital environment (C A Mackay, et al, annual scientific meeting of the faculty of accident and emergency medicine, London, December 1999).
In the USA RSI has become established as routine practice for emergency physicians. Ma et al14 in 1995 found that 41% of departments never requested an anaesthetist for intubations, with only 7% of departments mandating the presence of anaesthetic personnel during the administration of paralysing agents. In the UK system it is probable that anaesthetic experience will play a pivotal part in the training of emergency physicians in this technique. Therefore it is vital to foster cooperation between specialties in the future development of this technique. Emergency physicians should recognise the need for anaesthetist to be involved in resuscitation for their own experience and training and anaesthetist should accept the need for emergency physicians to be competent and practised in RSI techniques. Further work is needed to determine if there is any difference in outcome/complication rates between non-anaesthetist and anaesthetists in performing emergency RSIs in the resuscitation room in the UK.
Guidelines from the Association of Anaesthetist recommend that 24 hour cover of emergency departments by skilled anaesthetic staff should be immediately available.15 However, the increasing workloads placed on anaesthetic/ITU departments means it is difficult for anaesthetists to be consistently present for the arrival of critically ill/injured patients. RSI is a technique that both emergency physicians and anaesthetists should possess. This study demonstrates that RSI is currently being performed by emergency physicians. Emergency medicine in the UK needs to develop a fundamental understanding and ownership of emergency airway management, including the development of agreed indications in which it is appropriate. Given the central position of RSI in resuscitation should not each UK department continuously audit this activity with the ultimate aim of creating a national database of activity similar to the NEAR database in the USA?
Data collected by survey tool
Date and time of RSI
Age and sex of patient
Timing of the decision made to do an RSI
Grade and specialty of decision maker
Indications for RSI
Time at which RSI practitioner* contacted
Arrival time of RSI practitioner*
Profile of RSI practitioner* (grade and specialty)
Time to securing definitive airway
Drugs used
Complications
*The RSI practitioner was defined as the person/s administering the anaesthetic drugs and performing the tracheal intubation.
Acknowledgments
The authors would like to acknowledge the assistance of all the regional lead consultants and specialist registrars: Jason Kendall, Paul Younge, Alisdair Gray, Gary Kitching, Alistair McGowan as well as all the specialist registrars involved in the data collection for this study.
References
Footnotes
-
Contributors
Mr J M Butler was responsible for recruitment of study centres, data collection and analysis, critical review of the evidence and wrote the paper. Mr M Clancy initiated the study, developed the survey tool, was responsible for coordinating data collection and analysis and helped to write the paper. Mr N Robinson helped to develop and pilot the audit tool and was involved in data collection. Mr P Driscoll was involved in discussing core ideas, data analysis and contributed to the paper. Mr J M Butler and Mr M Clancy will act as guarantors for this paper.
-
Funding: none.
-
Conflicts of interest: none.