Article Text

Abstract
Objectives: To describe the nature and extent of prehospital doctor activity in an area of the West Midlands by review of group email. To explore the use of email as a means of data collection among a group of prehospital doctors.
Methods: A retrospective review of data collected by a prehospital organisation's email based internet group.
Results: Nearly half of prehospital doctor calls were to road traffic accidents and nearly half of these were “serious”. Road traffic accidents involving pedestrians, trees, and motorcycles often resulted in fatalities. Doctors frequently performed medical interventions at scene. Midazolam and ketamine were administered commonly; the indications for their use varied. At two cases on scene anaesthesia was maintained for over an hour with ketamine.
Conclusions: There remains a role for prehospital doctors. Email provides a very useful medium to share information and facilitate audit among a group of doctors who do not meet on a regular basis or work in the same institution. A computerised proforma to be filled by doctors after each prehospital call is proposed in an attempt to standardise and gather information for future audit and discussion.
- prehospital care
Statistics from Altmetric.com
The importance of providing rapid treatment to patients with time dependent injuries is well established.1 One third of all trauma deaths are preventable.2 Most deaths are attributable to failure to recognise (and treat) airway obstruction, chest injuries, and haemorrhage.3
The debate over “stay and play” versus “scoop and run” is too simplistic.3 For entrapped patients and in conditions where there is a delay in transporting patients to hospital, the presence of an appropriately skilled doctor at the scene can often bridge the gap between the limitations of an ambulance crew and the facilities of an accident and emergency department. Doctors can prolong the time spent at the scene 4 and delay the transfer of patients to hospital. This issue is further complicated by the increasing scope of paramedic skills. Their practice is currently limited by protocols, but with the advent of graduate courses a new generation of independent practitioner paramedic could be upon us.4 In this changing environment we need to redefine the role of the prehospital doctor in the public environment. This is particularly relevant in an age of accountability and clinical governance.
Most doctors who provide care in the civilian prehospital environment are organised into local schemes. Each scheme has its own call out criteria determined by local agreement between the doctors and area ambulance control. Guidelines issued by the British Association for Immediate Care (BASICS) exist to facilitate this process (personal communication). Local arrangements are tailored to suit each area's needs, although there is variation in the use of prehospital doctors by the different ambulance services (personal communication).
Schemes are self funded through charitable donations, with many doctors buying their own equipment and personal protective clothing. The majority of immediate care doctors are GPs, the remainder being hospital doctors from diverse specialties.5
The SoliCare and CentreCare schemes comprise 12 doctors responding to calls in Birmingham, Solihull, and an adjacent rural area. These doctors comprise one GP, two consultants in accident and emergency, one consultant in thoracic surgery, two consultants in trauma and orthopaedic surgery, one consultant anaesthetist, three staff grade doctors in accident and emergency, a specialist registrar in plastic surgery, and a specialist registrar in medicine. All are BASICS members and have completed BASICS training courses. All but one doctor have the diploma or fellowship in immediate care awarded by the Royal College of Surgeons of Edinburgh.
The two immediate care schemes, previously established separately, now operate functionally as one. There is no on call rota; doctors carry a pager. Ambulance control, on receipt of an appropriate emergency call or after on scene assessment by an ambulance crew, will activate a group alert on all pagers. Those doctors that are available telephone ambulance control in response to the group page. The most appropriate doctor, usually the closest, is given details of the incident before travelling to the scene. Ambulance control follow broad guidelines for activating this system. These guidelines have never been formally agreed but recognised indications include reports of patients entrapped, multiple casualties, or difficulty or delay in patient extrication or evacuation to hospital. The decision to notify ambulance control to activate the cascade lies largely with the first ambulance crew at the scene and will often reflect their own experience and capabilities.
The 12 SoliCare and CentreCare doctors share information on all prehospital calls by using the “Imcare” group email system to report all prehospital work and to facilitate discussion and learning points.
To examine current activity and to identify possible areas for improvement in prehospital practice, a review of recent events from the prehospital schemes was conducted and is presented.
METHODS
All email messages covering a 10 month period (3 October 1999 to 27 July 2000) were analysed retrospectively. Data describing the date, time of day, method of call out, case description, and medical interventions performed at the scene were collated and are presented.
There were no data that would permit classification of patients into “serious” or “non-serious” categories using conventional trauma scoring. A serious accident was defined as one which contained a patient with more than one long bone fracture, a suspected fractured pelvis, or an ambulance crew reporting difficulty with treating patient injuries.
RESULTS
Seventy five prehospital events were reported by the 12 doctors in a 10 month period, this is an average response once every four days. The types of incidents are presented in figure 1.
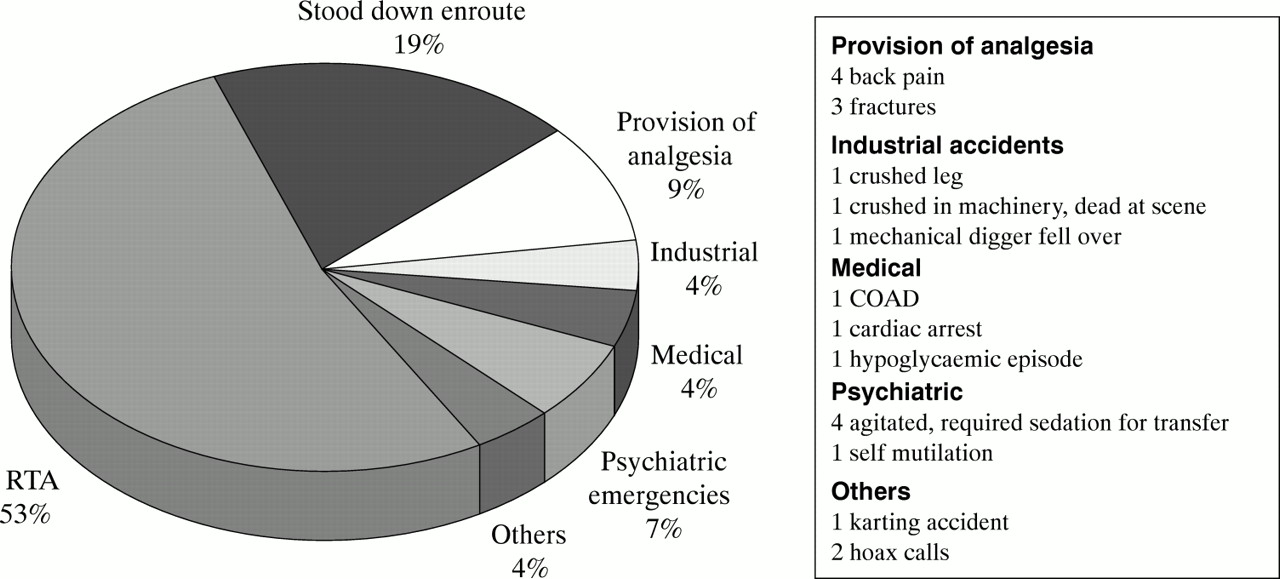
Categories of doctor call out.
The majority of calls, 40 (53%) were to road traffic accidents. Of these, 19 (48%) were patients in “serious” accidents. The call for assistance from a prehospital doctor was thought to be appropriate by the doctor concerned in 14 of the remaining 21 cases by virtue of significant history (massive vehicle damage or a potentially dangerous situation). The remaining seven calls were deemed to be inappropriate.
Motorcycles were involved in five road traffic accidents and each was associated with at least one death.
Six road traffic accidents involved a pedestrian, five of these had serious injuries, one later died.
A tree was involved in six road traffic accidents. In four of these cases, patients had serious injuries. There were two on scene fatalities among this group.
There were nine calls “intercepted” by doctors monitoring ambulance radio. A doctor can tune in to the ambulance radio frequency and monitor the incidents being tasked to the ambulance crews. If any of the incidents appear appropriate that doctor can offer assistance. These group of calls were: one asystolic drowning (that survived subsequent to the doctor's interventions), two serious road traffic accidents (one with a patient dead at scene, the other with a multiply injured patient), one hoax shooting, a cardiac arrest, a hanging, and four minor road accidents with no serious injuries.
Times of calls
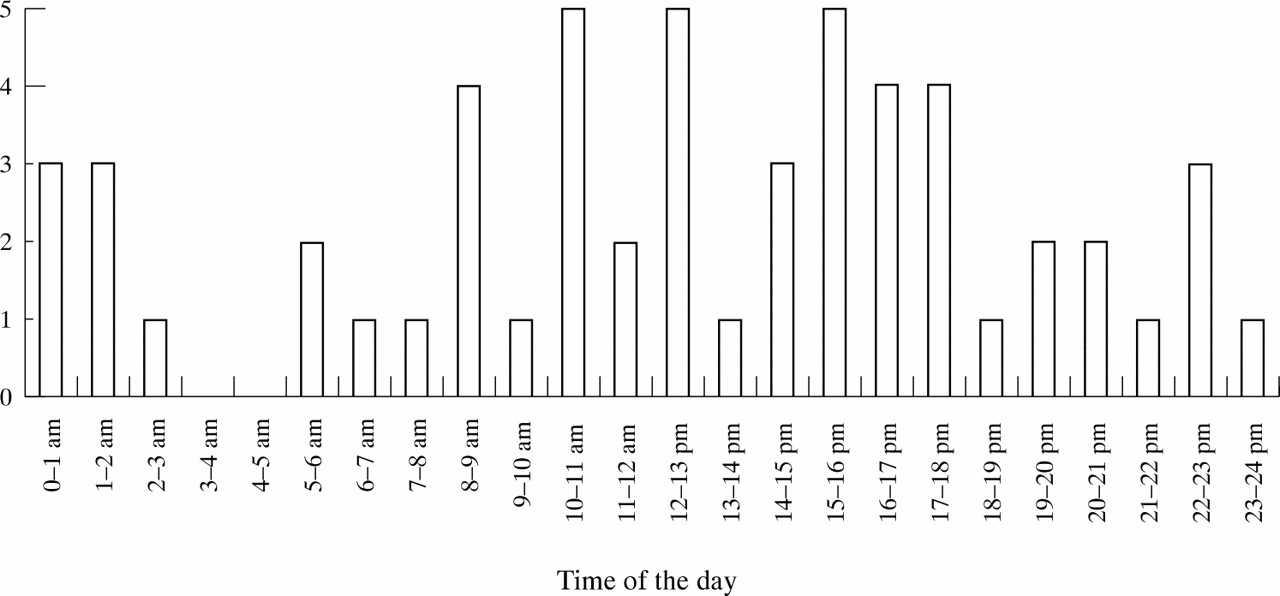
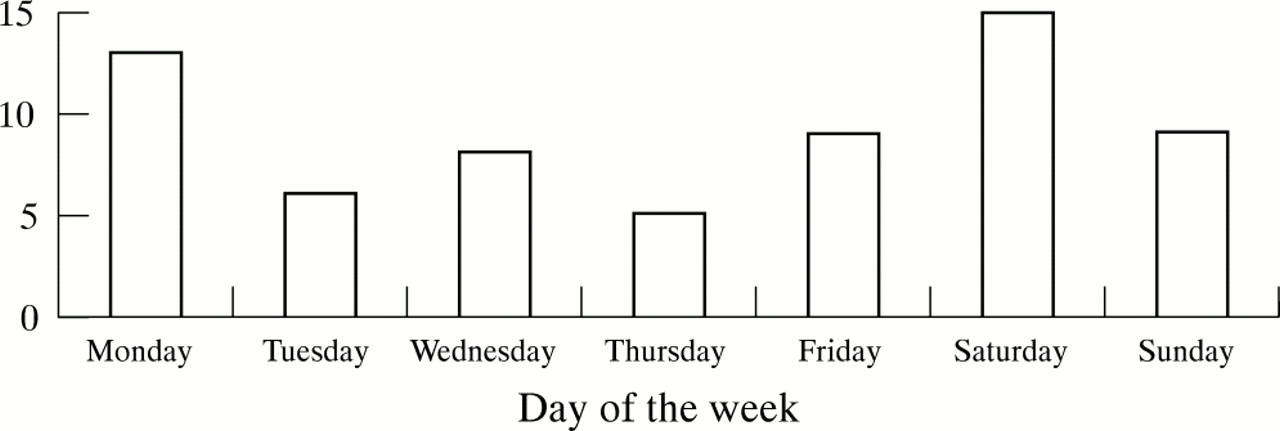
There was a trend towards more activity at the weekends and early evenings. The time and day of the week on which doctors were called are presented in figures 2 and 3. The number of calls was too small to determine the statistical significance of the distribution.

Time of calls.
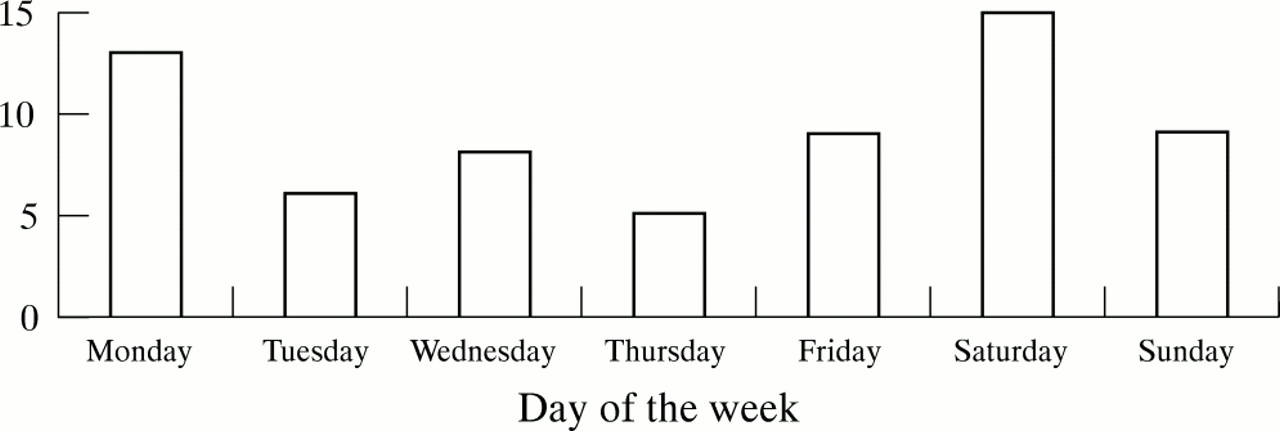
Day of the week.
Medical interventions
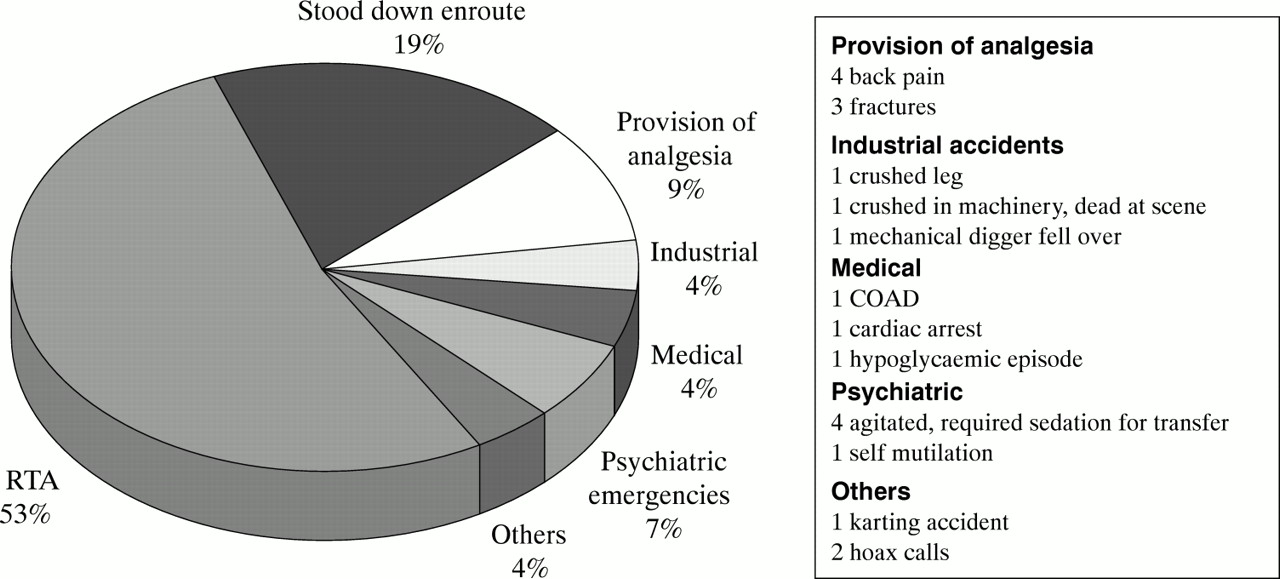
Interventions were performed at 45 of 75 (60%) cases. These are presented in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Doctors' interventions.
Ten different drugs were used: midazolam, ketamine, atropine, lignocaine (lidocaine) as local anaesthetic, three types of opioids, chlorpromazine, entonox and oxygen.
Analgesia was administered in 23 of 75 (31%) of all cases, most of these for road traffic accident victims. Opioids were used five times; ketamine 11 times; midazolam was added to an analgesic agent five times; a nerve block was used once; and entonox was give to one patient. Analgesia and anaesthesia were commonly administered to trapped patients (four of seven cases).
Midazolam was used eight times; seven times for sedating agitated patients and once purely for anxiolysis. Among the agitated group it was used to sedate patients whose agitation was attributable to pain four times and for psychoses three times. It was used at two RTAs. On three occasions it was used with ketamine.
Ketamine was used 13 times by four doctors, 11 times for analgesia and twice to induce anaesthesia. It was used in 17% of RTAs (7 of 40). The two times it was used for anaesthesia were among this group, both with prolonged on scene times because of entrapment (on scene anaesthesia >1 hour). The remaining 11 cases were for analgesia (10 patients with fractures and one impaled patient).
Seven deaths were certified by doctors; five at three RTAs, one at a factory, and one for a patient found hanging.
In four cases doctors reported that they had influenced time at the scene; encouraging prompt evacuation to hospital after recognising time critical injuries. No scene times were recorded.
DISCUSSION
Immediate care doctors are a limited resource and are of potential benefit in only a minority of ambulance work. Further work is required to optimise the call out thresholds and procedures. The high rates of morbidity (and indeed mortality) identified in the “intercepted” radio calls (when a doctor was not activated by the ambulance service) suggest that at present, immediate care doctors are not used to their full potential. In this study, we were unable to collate accurate data on scene times when prehospital doctors were deployed. Clearly, this needs to be examined in future studies and investigated as part of the ongoing evaluation of prehospital medical activity.
To optimise the call out rate, a good relationship with the local ambulance service is essential. They need to be made aware of the potential of immediate care doctors in different scenarios. Similarly, they need to understand when the presence of a doctor is unlikely to be of additional benefit.
In this series it seems that a doctor was of benefit in road accidents where there were entrapped casualties, and in those involving trees, pedestrians, and motorcycles. Other predictors of high morbidity and mortality were accidents involving high velocity impacts, car disintegration, car roll, severe intrusion, and ejection from the vehicle. Where of benefit, the doctors either provided care beyond the remit of the paramedic or influenced scene management. Further work, and more scene information is required to identify other scenarios that should initiate the activation of a prehospital doctor. This will lead to an evidence based protocol for call out criteria.
The data for this series were collected by freehand email. It is clear that a lot of on scene activity was not reported in this way. A standard computer based proforma is required to collate this additional information. A proposed form for all prehospital doctors is presented in appendix 1. Use of such a form on email groups could facilitate a national audit and in turn would enable BASICS to identify the nature and extent of prehospital activity around the country. This would assist in determining the contribution of prehospital doctors in different scenarios and would identify training and funding needs. It would assist in monitoring the difference that training to different standards confers on doctors. Funding will be dependent upon proving our worth.
During the period that this email review was conducted, prehospital doctors in the schemes were dispatched by the ambulance service only after an initial assessment of the scene by an ambulance crew, thus often wasting valuable time. The scheme subsequently entered into an agreement with the ambulance service that doctors would be called out after receipt of an emergency 999 call by virtue of the reported mechanism of the event, and not after scene assessment by an ambulance crew. Initially, it has been agreed that doctors will be called to accidents where there are reports of entrapped patients. This agreement was in part facilitated by email group awareness of the nature of the scheme's current activity mediated by email discussion.
The majority of SoliCare and Centre Care doctors do not work in the same institution or live close to one another. They do not meet on a regular basis. An email forum was established to facilitate discussion and audit. In an age of clinical governance and accountability, we need to prove value, worth, adherence to standards, and a difference to the outcome. We need to define the role of the prehospital doctor in Britain and to maximise patient care and minimise unnecessary call outs. The collation of standardised data is essential to this task. Email provides an invaluable medium for this purpose.
In this study we have presented an overview of recent prehospital medical activity in one area of the country. This is an important first step in auditing this activity. Clearly information detailing scene times, patient scoring, and patient outcomes is required to establish a more meaningful audit cycle. Future work will examine these areas. This requires greater communication between receiving hospitals (particularly those that enter data into National Trauma Audit and Research Network) and prehospital groups. Established hospital centred audit programmes need to feed back information to prehospital groups to disseminate relevant information about patients who received prehospital care back to the prehospital groups. Email can facilitate this process. This will be of great importance in an age of accountability and clinical governance. Prehospital doctors therefore need to collate and submit data in an honest and accurate manner. Communication links need to be established between prehospital groups and hospital audit coordinators.
Appendix1: Proposed proforma for logging prehospital activity
Date: Weather conditions: dry/wet/icy, etc
Day: Contact method:
Time of call: Access difficulties:
Time at scene:
Time clear of scene:
Description of case as given by ambulance control:
Description of case and events:
Equipment used (where appropriate please state which and how much):
Airway adjuncts Oxygen
IV access Fluids
C-spine collar
Drugs:
Other: RSI, surgical procedure, etc
Influenced on scene time? How?
Hospital alerted Y/N
Accompanied patient to hospital Y/N
Comments
Footnotes
-
Funding: none.
-
Conflicts of interest: none.