Article Text

Abstract
Objectives: To design a computerised system of calculating resuscitation requirements and to test this system to ensure that it gives accurate and fast results, so that it could potentially be used in the resuscitation of patients in a accident and emergency (A&E) department.
Methods: Using internet based technology we have developed a program that runs inside most web browsers and can be used to calculate several parameters (including endotracheal tube dimensions and drug doses). The only value that is required is the age of the patient. The weight is calculated and can be adjusted if known. The resuscitation requirement calculations are made from the weight. The program was then tested on staff members in the department to calculate theoretical resuscitation requirements for paediatric and adult patients. Accuracy and speed of the computerised calculator was compared with the conventional paper based calculation methods.
Results: Subjects performed better using the computerised calculator. On average they made significantly fewer errors (21.4% more accurate than using conventional methods) and were three times faster.
Conclusion: The computerised calculator has proved, in a controlled setting, to be a more accurate and faster way of calculating resuscitation requirements than conventional methods.
- resuscitation
- emergency
- calculation
- computer
Statistics from Altmetric.com
Those of us who work in emergency medicine have all experienced the frustration of trying to find and then process a crucial piece of drug information in a resuscitation setting.
Studies show that medication errors are the most common cause of adverse events affecting hospital patients.1 Data also show that medication errors are frequent 2 and that medication errors pose a significant risk to patients.3,4 A significant number of medication errors are preventable.2,5 Medication errors are most commonly caused by prescribing errors, and these include choice of the wrong dose of drug.2,6
Given the inherent pressure that arises in resuscitation situations, it seems evident that a busy resuscitation room in an accident and emergency (A&E) department is a prime place for medication errors to arise,1 with potentially grave consequences.
Current tools that assist resuscitation requirement (including drug) calculation do offer practical solutions, but either entail some manual calculation or only apply to the paediatric population 7 and cannot be applied to the larger number of adult patients that require resuscitation. In our experience, calculations for those adult patients often have to be made by referring to reference texts (for example, BNF, etc). The idea of using computers to assist in the prescribing of drugs is not new.8–10 Several interventions involving information systems have already been shown to reduce medication errors considerably.11–13 However, no system that we have seen, IT based or otherwise, offers a solution to the calculation of resuscitation requirements for both adults and children, in an emergency setting like resuscitation.
The purpose of our own efforts, involving the development of a web based computer program, was to tackle this specific challenge of accurate and speedy resuscitation requirement calculation. The aim of our subsequent study was to verify whether the program provides a safer and faster method of resuscitation requirement calculation than traditional paper based methods.
METHODS
Development
Though there are many computer applications that can be used to solve calculations, we looked at the variety of internet technologies that are available, as these offer solutions that can be easily shared across systems.14 For portability and speed of deployment we chose to use a mixture of the HTML and JavaScript languages. This allows our program to run on the majority of web browsers, allowing it to be run on the internet, on hospital intranets or simply on a stand alone PC.
The program is designed to offer a simple user friendly interface. The opening screen (see fig 1) starts with the user inputting the patient's age. Then a click of a button allows calculation of the patient's weight. The weight is calculated along the 50th centile for children, based on well recognised charts.15 If the patient is 17 or over the user is asked to confirm that the likely weight is 70 kg. This default value can be adjusted if the weight of the patient is known. A click on the “Calculate Resuscitation Requirements” button immediately calculates a total of 23 parameters (including endotracheal (ET) tube diameter and length, fluid bolus and drug doses (mg and ml) for 10 different drugs (see box). This information is displayed on the screen (see fig 2) and printed out and kept with the patient's notes as a record.

The opening screen of the resuscitation calculator.

The calculator shows the results of calculations.
Table of resuscitation requirements calculated
-
Fluid bolus (IV)
-
Drugs (all IV)
-
Morphine
-
Cefotaxime
-
Salbutamol
-
Suxamethonium
-
Etomidate
-
Thiopentone
-
Lorazepam
-
Diazepam
-
Phenytoin
-
Mannitol
-
Equipment
-
ET tube diameter
-
ET tube length
Validation
Once the system was developed it was validated. A prospective trial was conducted.
The system was tested on a total of 20 A&E and paediatric medical staff members (including SHOs, middle grades, and consultants) in a controlled setting. Each was asked to calculate the weight and then a set of resuscitation requirements for three patients—two children (6 and 13 years old) and an obese business manager weighing 100 kg. They were given standard texts to consult 16–22 and a simple calculator and were timed by one of the three researchers. They were then shown the computer based resuscitation calculator, “Resusicalc”, for the first time and using this were asked to complete the same calculations. (The program was started instantly, with a click on the relevant “desktop” icon, on a PC based in the A&E department). They were timed again.
The answers were scored against an agreed range for each parameter (so a correct answer could be calculated from any individual text). The answers were then compared for both accuracy and speed of calculation. Statistical analyses were performed using SPSS for Windows Version 10.1. In addition to descriptive statistics, the Shapiro-Wilk test was used to test distributions; the matched pair t test was used to compare performance between individuals across the two trials, and confidence intervals were constructed for within trial and between trial parameters.
RESULTS
For ease of interpretation, scores have been transformed from “items correct” (maximum score =26) to percentage correct. Such transformations retain the original distributions.
Distributions
Observations for scores attained and times to completion using paper based reference material were normally distributed, as were those for times to completion via the computer based method. The distribution of scores attained during the computer based trial was non-normal; this being entirely attributable to the fact that all bar one subject achieved the maximum score.
However, data representing the time to completion differences between paper based and computer based scores were normally distributed. These results mean that parametric methods are entirely appropriate for comparing resuscitation methods.
Parameters
Scores
The mean score for the paper based assignment was 78.4% (range 38.5% to 100%, standard deviation was 16.5%). Mean score for the computer based assignment was 99.8%, all bar one subject scoring 100% (standard deviation 0.86%, although this figure is largely academic). Figure 3 shows the distribution of individual scores by method.
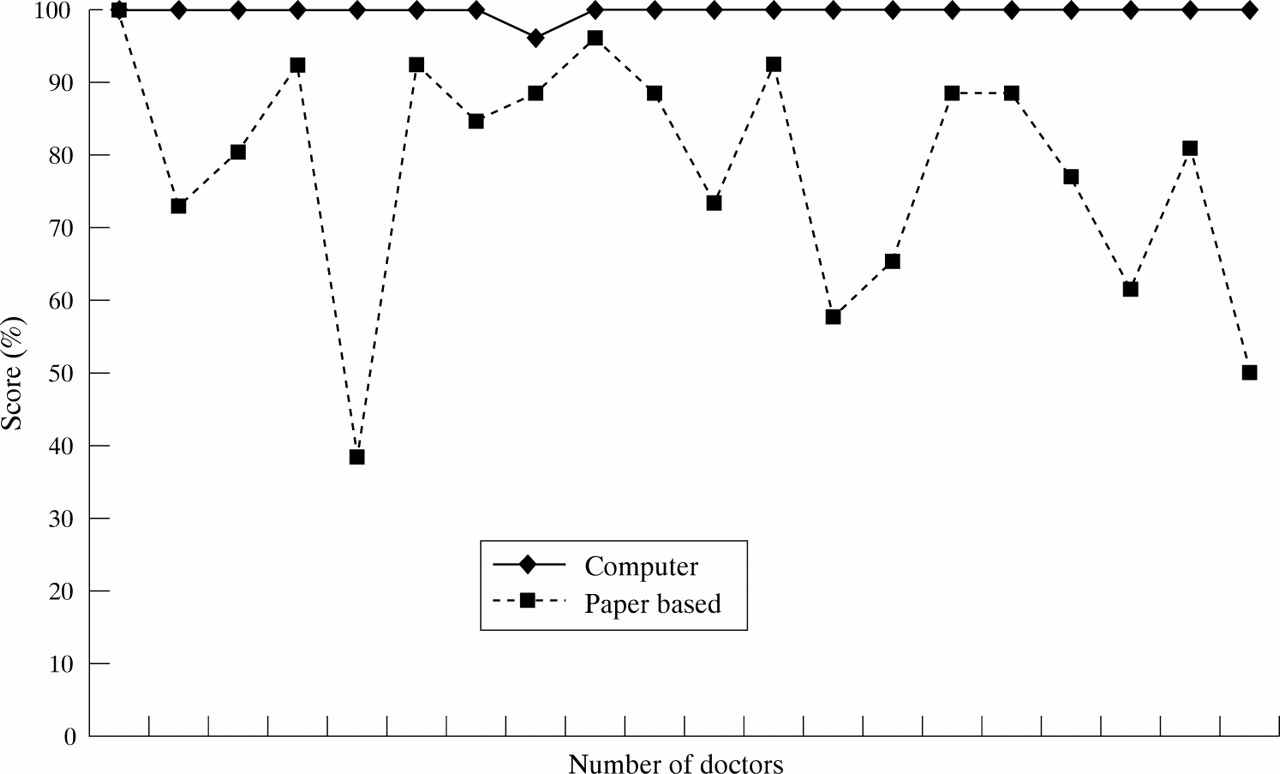
Chart of calculation scores.
Time to completion
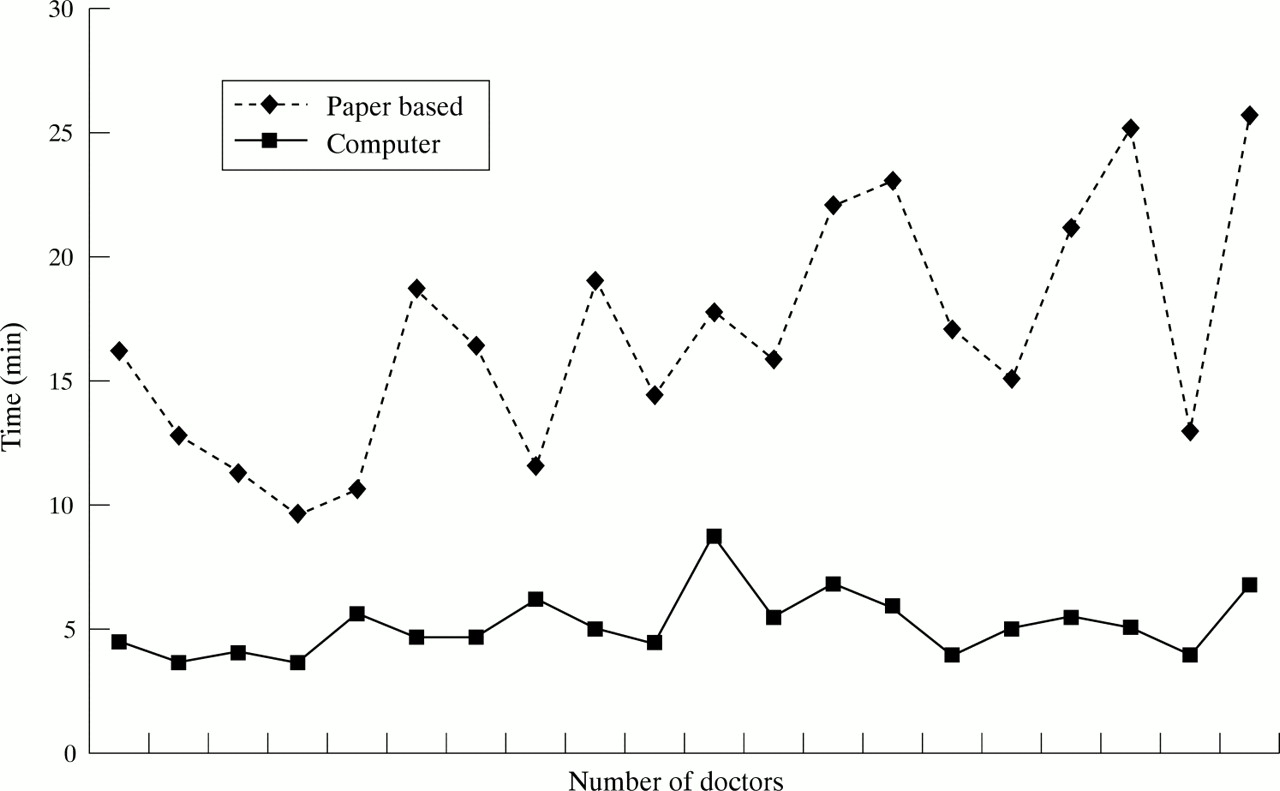
Mean time (minutes and seconds) to completion of the 26 calculations for the paper based model was 16:47, (range 09:40 to 25:30, standard deviation 04:43). Mean time for the computer model was 05:12, (range 03:40 to 08:45, standard deviation 01:43). Figure 4 shows the distribution of individual “times to completion” by method.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Chart of calculation times.
Key points of results
Scores
The mean difference for “items correct” was 21.4% in favour of the computer based method (the 95% confidence intervals for the difference being 13.6% to 29.1%, matched pairs t test, t=5.74, p<0.0001 with 19 degrees of freedom). On average, therefore, the computer program affords 21.4% greater accuracy than the paper based method.
Time to completion
The mean difference in task completion time (minutes/seconds) was 11:35 in favour of the computer program (95% confidence intervals for difference −09:33 to −13:36 minutes, matched pairs t test, t=12.0, p<0.0001 with 19 degrees of freedom). Subjects therefore completed their tasks 11.5 minutes quicker, on average, when using the computer program. On average, therefore, using the computer program was more than three times faster then the paper based method.
DISCUSSION
In an effort to facilitate the stressful and potentially dangerous challenge of resuscitation requirement calculation, for patients of all ages, we have looked for a solution that was accurate yet fast and have found it in an IT based application. Before implementing our computer based solution on a practical basis, we felt it was essential to test its value with a structured assessment.
In the subsequent study, we have chosen to compare our computer based system with paper based calculations, as in our experience, medical staff often have to resort to paper based calculations during the resuscitation of adults patients, who comprise the majority of resuscitation cases. We have chosen to base the calculations on a combination of age and weight, rather than height or sex, in line with most of the standard reference texts (APLS manuals, etc). Our study focuses primarily on the issue of improving the quality of the calculations that are very often necessary during resuscitation, as any error in the calculation is of the greatest significance and potentially disastrous.
The structured assessment of the computer based calculator has proved it to be a more accurate way of prescribing than traditional methods, in common with other IT based prescribing systems and so is a potential adjunct in terms of risk management. It is also considerably faster than conventional methods.
Study limitations
As the system has been validated in this controlled setting, consideration of a clinical trial in a resuscitation setting raises difficult practical and ethical issues. Our feeling is that the calculator's clear advantages in terms of accuracy and speed mean that it is inherently safer than previous used methods, though we accept that ideally a clinical trial is needed to prove that point.
Implications
In our own department, it has been recently introduced into a clinical setting, on a desktop based PC in our resuscitation room. Users are able to start the program in an instant by a simple click on a “desktop” icon on the PC. We have also installed the program on a more portable handheld PC.
We hope that our targeted IT based solution and its subsequent structured assessment go some way to demonstrating the great potential that still exists for IT to make medical care easier for medical staff and potentially safer for the patient.
CONCLUSION
In an effort to improve the accuracy and speed of resuscitation calculation, we have developed a web based computer calculator. It has proved, in a controlled setting, to be a more accurate and faster way of calculating resuscitation requirements than traditional paper based methods. We feel that this validated system has the potential to improve the efficiency of safe medical care practised in our department.
Contributors
Tony Shannon initiated the project, developed the program, and co-wrote the paper. Andy Ratchford and Dougal Southward researched the drug doses involved, tested the subjects, and co-wrote the paper. Anthony Hildreth did the statistical analysis and co-wrote the paper. Tony Shannon is the guarantor for the paper.
Funding: none.
Conflicts of interest: none.
REFERENCES
Linked Articles
- Primary Survey