Article Text

Abstract
Objectives: To describe an experience of emergency department (ED) overcrowding and ambulance bypass.
Methods: A prospective observational study at Royal Perth Hospital, a major teaching hospital. Episodes of ambulance bypass and their characteristics were recorded.
Results: From 1 July 1999 to 30 June 2001, there were 141 episodes of ambulance bypass (mean duration 187 min, range 35–995). Monday was the most common day with 39 (28%) episodes. Entry block alone was the most common reason bypass was activated (n=38, 30.4%). The mean number of patients in ED at these times was 40 (occupancy 174%), including nine in the corridor, seven awaiting admission, and 14 waiting to be seen. Episodes attributable to entry block were typically preceded by a presentation rate of ⩾10 patients per hour for ⩾2 hours (OR 6.2, 95% CI 4.3 to 8.5). Mid-afternoon to early evening was the most common time for activation. Ambulance bypass is increasing in frequency and duration.
Conclusions: Entry overload resulting in entry block results from overwhelming numbers of patients presenting to the ED in a short space of time. Entry block impairs access to emergency care. Unless something is done in the near future, the general public may no longer be able to rely on EDs for quality and timely emergency care. A “whole of system” approach is necessary to tackle the problem.
- emergency department overcrowding
- ambulance bypass
- access block
Statistics from Altmetric.com
Overcrowding in the emergency department (ED) is the most serious issue confronting EDs in the developed world.1 This results in ambulance bypass, a situation whereby an ED instructs the ambulance service to divert ambulances elsewhere, and hence bypass the nearest ED. The reason for this is because it is unsafe for more patients to attend. This is a situation occurring in many countries, and one that is deteriorating.2–,7 During periods of bypass, the ED still accepts critically ill or injured patients.
Overcrowding in ED is caused by a complex web of interrelated issues that have been previously reported and are summarised in boxes 1⇓ and 2⇓. The definition of terms used in this paper are in box 3⇓. The typical reason for ED overcrowding is “exit block” from the ED. Exit block is now termed “access block”—that is, the patient is denied access to an inpatient bed. The prime reason for access block is simply a lack of acute inpatient beds.
Causes of overcrowding in the emergency department (ED)
(Adapted from Derlet and Richards)2
1 Increased complexity and acuity of patients presenting to the ED
Overall increase in patient volume
Lack of beds for patients admitted to the hospital
Financial incentives favour elective surgery over emergency admissions
Avoiding inpatient hospital admission by intensive assessment and treatment in the ED
Delays in service provided by radiology, laboratory, and ancillary services
Shortage of nursing staff
Shortage of specialty consultants
Shortage of administrative/clerical support
Shortage of physical space within the ED
Shortage of junior medical staff
Problems with language and cultural barriers
Medical record documentation requirements
Difficulty in arranging follow up care
Effects of overcrowding in the ED
(Adapted from Derlet and Richards)2
Patient safety at risk—that is, compromised clinical care
Prolonged pain and suffering
Staff may leave because of the incredible demands placed on them
Long waits and dissatisfaction of patients
Ambulance bypass
Decreased clinical productivity and effectiveness
Violence
Negative effect on teaching and research
Miscommunication because of increased volume
Medicolegal sequelae
Inability to evacuate in an emergency, for example, fire
Definition of terms used
Access block
This refers to the situation where patients in the ED requiring inpatient care are unable to gain access to appropriate hospital beds within a reasonable time frame (http://www.acem.org.au/open/documents/standard.htm). We propose that the definition of access block is broadened to include both entry block (impaired access to emergency care) as well as impaired access to inpatient care.
Exit block
An older term now called access block. It referred specifically to a lack of inpatient beds, thus limiting outflow from the ED.
Entry block
Entry to the ED is (functionally) “blocked” because of overwhelming numbers of patients attending the ED in a short space of time (entry overload). It is overwhelming because it exceeds the physical and medical processing capacity of the ED. This results in impaired (or blocked) access to emergency care.
ED overcrowding
This refers to the situation where ED function is impeded primarily because the number of patients waiting to be seen, undergoing assessment and treatment, or waiting for departure, exceeds the physical or staffing capacity of the ED (http://www.acem.org.au/open/documents/standard.htm). This causes doctors and nurses to be unable to provide quality care.2 Objectively, this is reached when the ED exceeds 100% occupancy, or earlier if there is inadequate staff or other resources.
However, ED overcrowding may also be attributable to “entry block”—that is, entry to the ED is (functionally) blocked. With entry to the ED, inflow may be so great (entry overload) that ED overcrowding results, regardless of the number of beds available in the hospital.
The only control that an ED has over inflow is ambulance attendance, achieved by effecting ambulance bypass. At our ED, 42% of all attendances arrive by ambulance. Therefore, ambulance bypass represents an effective mechanism for “turning off the tap”, allowing time to “catch up”, and thereby ensuring patient safety within the ED.
In Perth in the 1990s, ambulance bypass was almost unheard of. In the past few years, it has unfortunately become commonplace. Despite this being an international phenomenon, little has been published from Australia on this subject. This paper reports our experience with ambulance bypass.
METHODS
Study location
Royal Perth Hospital (RPH) is a major teaching hospital and is the largest hospital in the state of Western Australia. Perth is the capital city and has a population of 1.4 million. Prior to 1999, ambulance bypass was extremely rare. The ED has an annual census of some 55 000, with an admission rate of 44%. There are 23 cubicles in the ED. In the period 1996–2001, attendances have increased by 14% and admissions by 16%. In the same time frame, hospital bed numbers have been reduced by about one third. Staffing numbers for the ED ranged from 5–13 doctors and 10–18 nurses, at any one time.
Data collection
Up to October 2000, episodes of ambulance bypass were recorded at the time in the departmental diary. The decision to initiate bypass is made by the duty emergency physician. This judgement is based purely on safety. From mid-2000, a more formalised system was adopted, outlining specific criteria for initiating bypass (fig 4⇓) and the data to be collected, including the time of and reason for bypass. These data were collated and analysed from 1 July 1999 to 30 June 2001. The ED has a computerised patient tracking system (HAS EDIS version 8.54, Oracle), which also records hourly patient presentations. The data were collected onto a database and analysed in SPSS (version 10).
RESULTS
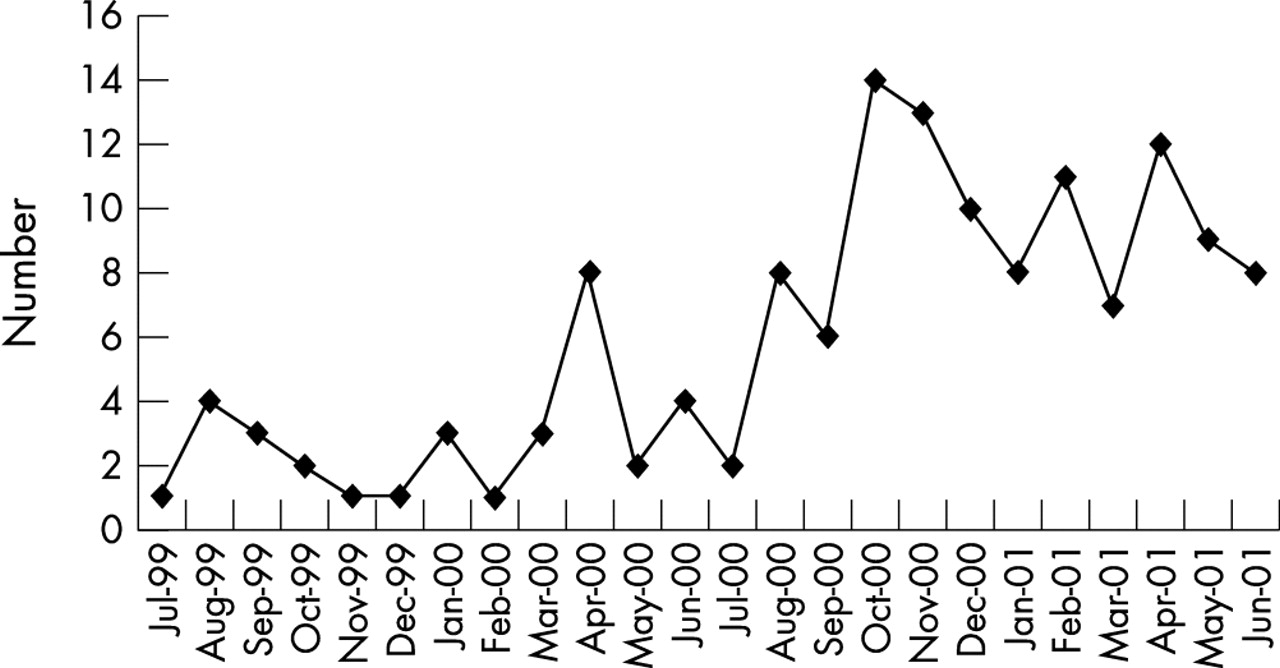
In the period 1 January 1998 to 30 June 1999, there were two episodes of ambulance bypass at RPH. In the two years from 1 July 1999 to 30 June 2001, there were 141 episodes of ambulance bypass, including four days in which bypass was required twice. Hence, on average, the ED was on bypass every fifth day. The mean duration of bypass was 187 minutes (range 35–995) and this is increasing. Figures 1⇓–4⇓ illustrate a number of descriptions of ambulance bypass. Table 1⇓ outlines the volume of patients within the ED when ambulance bypass was activated.
Volume of patients in ED when bypass activated

Monthly episodes of bypass July 1999–June 2001.

Episodes of bypass by day of week.

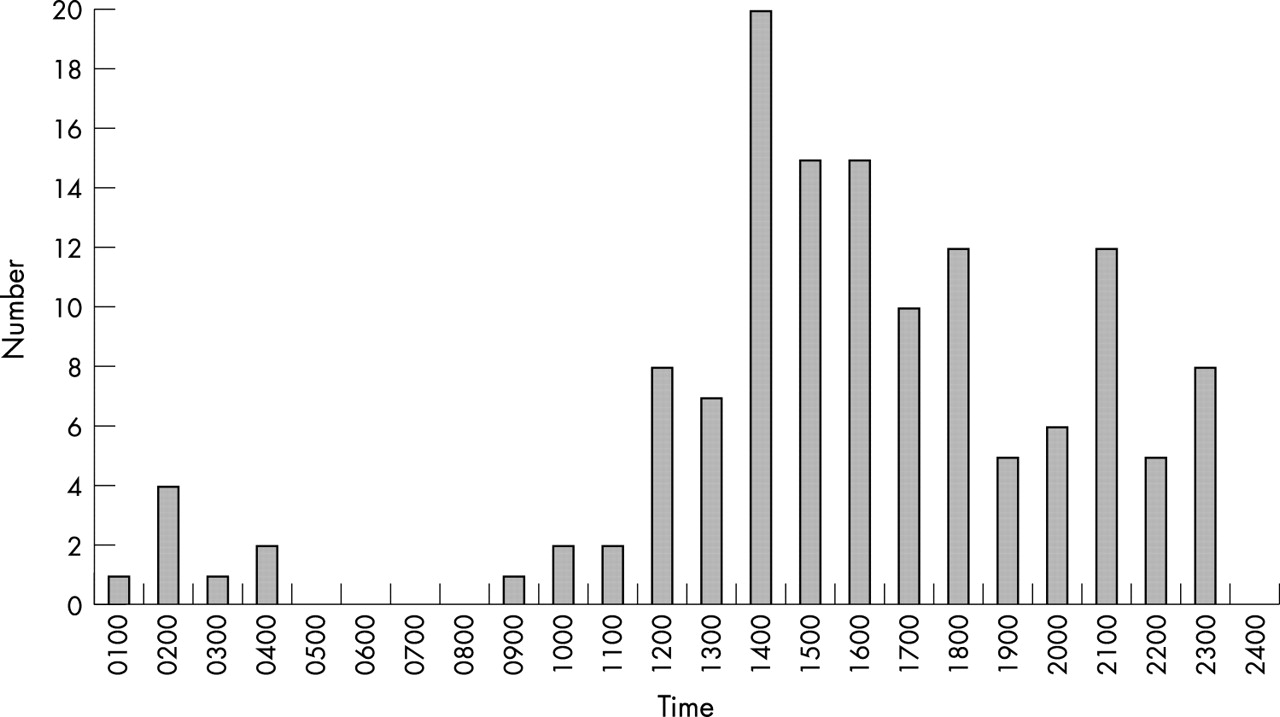
Time of day bypass activated.

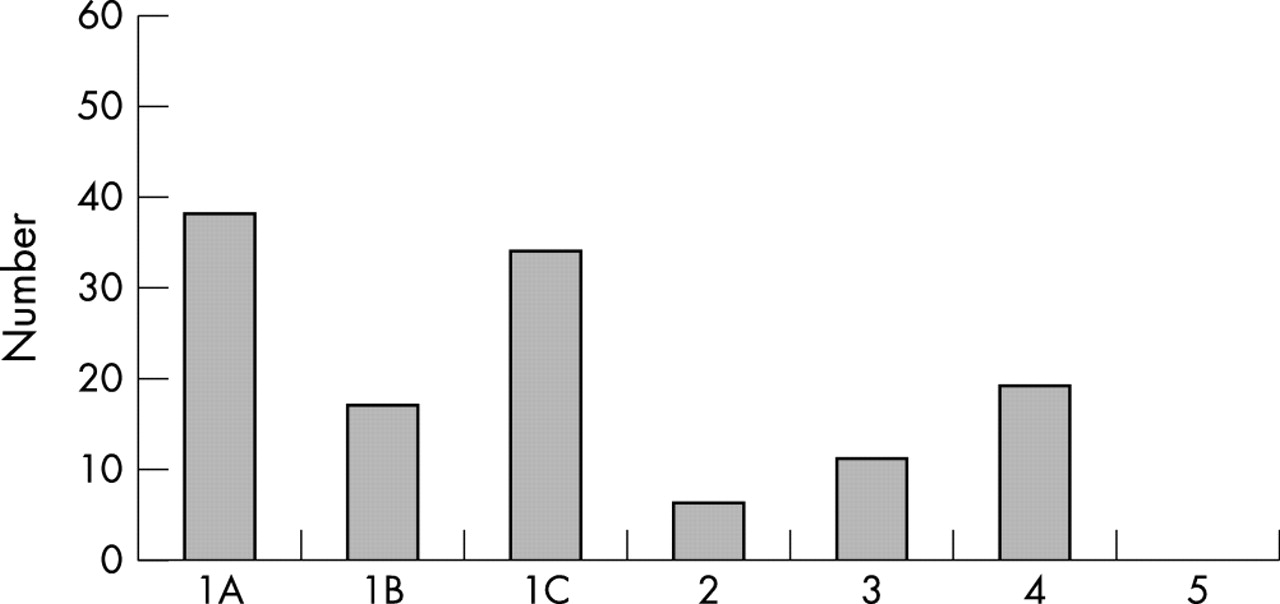
Criteria for initiating ambulance bypass. 1 Excess patient load—from whatever cause; 1A predominantly entry block; 1B predominantly exit (access) block; 1C combination of above. 2 Environmental for example, fire, air pollution, bomb threat, sewerage spill, abnormal noise, etc. 3 Staff/resource issues for example, deficiency, illness, inexperience, power failure, insufficient monitoring facilities. 4 Excessive number of high acuity patients—here the department resources may be overwhelmed by fewer patients than in 1 above. 5 Declared disaster situation—where RPH is site of, or receival centre, for disaster.
Figure 4⇑ highlights the reasons for ambulance bypass. Excess patient load was the most common reason (89, 71.2%). This consisted of entry block (38, 30.4%), exit (access) block (17, 13.6%), and a combination of the two (34, 27.2%). Following this, an excessive number of high acuity patients was the next most common reason (19, 15.2%). (More than one reason was specified on some occasions). Monday was the most likely day of bypass with 39 (28%) episodes. The time bypass was activated was typically mid-afternoon to early evening. April 2001 had the largest total time on bypass of 2704 minutes, which represents 6.3% of the month.
Examination of the number of attendances in the two hours before activation, indicates a typical presentation rate of ⩾10 patients per hour. This compares with an average presentation rate of 6 (SD 3.2) per hour (range 0–19), thus representing a two thirds increase above average. The odds ratio for initiating ambulance bypass when presentations are ⩾10 patients per hour for two hours to the ED is 6.2 (95% CI 4.3 to 8.5).
Data supplied from the ambulance service reveal an increase of about 1000 patients per year being taken to RPH after the opening of a new freeway near RPH (personal communication, St John Ambulance). The proportion of ED attendances arriving by ambulance in the six months before the opening of the new freeway was 40.4%, compared with 43.6% in the six months after.
Data were also obtained on the percentage of ED patients waiting >8 hours for ward admission: 1999–2000: 7.3%, 2000–01: 12.2%, and 2001–02: 20.9%.
DISCUSSION
We have described “entry overload” resulting in “entry block”: overwhelming numbers of patients presenting to the ED in a short space of time. This was our most common reason for requiring activation of ambulance bypass. These data have not been previously described. The result is impaired access to emergency care.
This scenario is similar to the definition of a disaster or major incident. A health service major incident is said to exist when8:
Any occurrence presents a serious threat to the health of the community
The health service is disrupted
There are, or are likely to be, so many casualties that special arrangements are necessary to deal with them.
We consider this situation of ED overcrowding to be a disaster, one now occurring daily and deteriorating. In fact, it is now possible to predict the likelihood of going on ambulance bypass, according to the presentation rate of patients to the ED: ⩾10 patients per hour exceeds our ED’s physical and medical processing capacity. The opening of a new freeway near RPH in April 2000 may have contributed to this phenomenon, as ambulance access to RPH is now quicker and easier.
The mid-afternoon to early evening likelihood of ambulance bypass reflects the cumulative effect of the pattern of ambulance and patient arrivals. The increasing duration of episodes reflects the virtually non-existent flexibility and capacity of the system to respond to the increasing patient load.
Our data clearly demonstrate that ambulance bypass is a year round problem. The “winter flu” cannot explain this phenomenon. Monday was the most likely day for ambulance bypass. Problems with Monday have been previously reported.9 The reasons for this may include that patients may not “bother” their general practitioners over the weekend, and are therefore referred in larger numbers for emergency assessment on Mondays. Also, patients admitted to the hospital on the weekend may not be fully assessed by their team until later in the day on Mondays.
Our hospital’s medical administration have provided enormous support with increased staff and resources, as well as effective bed management. The problem, however, lies outside the hospital. We receive so many patients that our occupancy exceeds 200% at times. It is paradoxical that other departments within a hospital cannot exceed 100% occupancy, and yet the ED, which may contain some of the most seriously ill and injured, is allowed to exceed the safe level of 100% occupancy.
There are a number of factors contributing to our entry overload:
General increase in population
Aging population
Illicit drug use with its attendant psychiatric and social effects
General community expectations for instant treatment. Emergency medicine can also be termed “available medicine”
Lack of acute beds and services in feeder hospitals (both rural and metropolitan)
The network of roads that lead to our hospital
Obviously, a larger ED may help to overcome some of these problems. According to the Australasian College for Emergency Medicine ED design guidelines, our workload requires 60 cubicles.10 A department of that size would require a large increase in human and other resources, which are not available. It would also attract a greater workload, and with access block, perhaps lead to an even greater inpatient load within the ED. Our data describe our experience with ED overcrowding, and has relevance to the many undersized EDs around the world.
The fact that health systems in the USA, UK, and Canada are all suffering from similar difficulties, suggests that a profound change has occurred in the delivery of western medicine.11 Health care in western societies has been through a period of severe economic rationalisation, resulting in closure of thousands of beds in the acute hospital system. For example, in the USA, the number of medical and surgical beds declined by 18% in 1994 to 1999. From 1990 to 1999, attendances at EDs increased 15%.11 There have also been many aged care beds closed or changed to community based facilities.
In simple terms, demand has increased while the capacity of the system has decreased.12 This is best exemplified by our increased workload with decreased hospital beds. As such, after a decade of hospitals downsizing and reducing operating costs, local healthcare systems have been left with little slack to accommodate surges in patient volume.11 It is also worth noting that at least one study has found that if hospital bed occupancy rates exceed 85%, then bed crises occur.13 Spare bed capacity is therefore essential for the effective management of emergency admissions.13 The increasing wait for ward admission from the ED reflects the growing problem with access block. Access block has been described as the major social, organisational, and clinical issue in emergency medicine today (fig 5⇓).14

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A typical scene of emergency department overcrowding. Situations such as these lead to loss of clinical productivity and effectiveness, and places patient safety at risk.
The ED has always been available to help if all else fails in the health system. Unfortunately, that basic tenet is now being challenged, and the general public may no longer be able to rely on EDs for quality and timely emergency care, placing the safety of people at risk.2,15–,17 In addition, Derlet has stated that should there be a major infectious disease epidemic or national catastrophe, EDs and hospitals could not accommodate the demand, undoubtedly leading to increased suffering and excess mortality.12
Ambulance bypass is now an entrenched aspect of emergency medicine in Australasia. However, it has been a major problem in the USA for many years. In one four year period, ambulance bypass increased by 453%.7 In a 1990 survey, 38% of EDs reported holding admitted patients in the ED for 24 hours or longer.15 It has been suggested that the problem is “ a badly flawed approach to financing health care that values profits over patients.”15
Government at all levels need to recognise and acknowledge the problem of ED overcrowding, and that it requires a system wide approach. The government of the Australian state of Victoria has published an “Emergency Demand Management” paper, which reports that they require the equivalent of another major suburban hospital.18 After opening additional beds in 1999–2000, there was a 24% reduction in the number of patients waiting in EDs more than 12 hours for admission, and the episodes of ambulance bypass decreased by 30%. However, in the September 2000 quarter, access block and bypasses increased again, reflecting that the hospital system was operating at capacity and was unable to absorb further pressure.18
The New South Wales government has also investigated “bed access block”, and produced an “Emergency Department Services Plan.”19 This paper states that “access block is a whole of system dilemma”, and “must be adequately resolved to ensure the functionality of EDs.”19
Stop gap measures (box 4⇓) to tackle ED overcrowding, such as ambulance bypass and delaying elective surgery, may help to reduce sporadic strains on capacity, but they focus only on the most immediate problems.11 Specific solutions are needed to address all the causes of ED overcrowding listed in box 1⇑. However, the most immediate solution is simply more acute hospital beds and more aged care beds. For our ED, and for all overcrowded EDs, increasing the capacity of the hospitals across the system would really make a difference.
Stop gap measures for ED overcrowding
Ambulance diversion
Increasing ED capacity, with both human and physical resources
Reopening inpatient beds
Postponing elective surgery
Improving discharge processes
Acknowledgments
The authors are grateful to Deborah Brooks and Julien Harris, Division of Critical Care, Royal Perth Hospital, for their assistance with data collation, Jeffrey Williams, Manager Operations Centre, St John Ambulance, Dr Yusuf Nagree for assistance with statistical analysis, and to all staff working in the ED.
REFERENCES
Footnotes
Conflicts of interest: none declared.
Linked Articles
- Primary Survey