Article Text

Abstract
Aims: To describe the nature, frequency, and characteristics of adult critical care transfers originating from the emergency department (ED).
Methods: A one year prospective regional descriptive study using multiple data sources of all critically ill adults transferred from an ED or a minor injuries unit (MIU) within the former Yorkshire Regional Health Authority Area or into a regional critical care facility if originating from an ED or MIU elsewhere.
Results: 29 EDs transferred 349 adults into the regional critical care facilities. The median number of transfers per department within the region was 18 (range 1 to 42). Seventeen were transferred from outside the region. A total of 263 (75%) patients were transferred for specialist care and 76 (22%) for non-clinical reasons. Altogether 294 (84%) were admitted to intensive care or a high dependency unit at the receiving hospital. The in-hospital documented mortality rate was 26%. A total of 170 patients (49%) had traumatic pathology of which 101 were principally transferred for management of a head injury. Median time in the ED was 3 hours 5 minutes (range 11 minutes to 17 hours 47 minutes). In 146 (42%) patients the decision to transfer was primarily made by the emergency medicine clinician. A total of 251 (72%) patients were intubated. The documented critical incident rate was 15%.
Conclusion: Trauma is the most common reason for transfer of the critically ill adult from the ED. A significant number of patients are transferred, however, with medical and surgical conditions and for non-clinical reasons. There continues to be problems with the quality of care that these patients receive. Emergency medicine clinicians must be actively involved in the development of regional critical care systems as a significant proportion of all critically ill adults transferred originate from the ED.
- secondary transport
- critically ill
- epidemiology
- ED, emergency department
- MIU, minor injuries unit
Statistics from Altmetric.com
The inherent problems with the organisation and process of the transfer of the critically ill and injured are well recognised by emergency medicine clinicians within the United Kingdom. Previous publications have highlighted the deficiencies in the quality of care received during the transfer of the critically ill and injured adult.1–3
A system-wide approach has been suggested for trauma4 and more recently by the Department of Health in the document Comprehensive critical care5 for the critically ill adult. This document defines areas within critical care practice that need improvement. Specifically, the organisation of transfers of the critically ill, the quality of care, and the associated training of the staff involved have been highlighted. Problems with quality of care have been attributed to inadequate monitoring,6 junior accompanying medical staff,1 and poor pretransfer stabilisation.2,7–9 Attempts have been made to improve standards and training by providing specific training courses10 and by developing clinical guidelines.11–13 Despite this little is known about the descriptive epidemiology of this group of patients particularly those transferred from the emergency department (ED). Even less is known about the quality and standards of care received during the transfer process and this patient group’s ultimate clinical outcome.
The aims of this study are to describe the nature, frequency, and characteristics of the critically ill and injured adult transferred from the ED.
METHODS
Setting
The principal study area was centred on 16 hospitals with EDs (13 district general hospitals with one providing some tertiary facilities and three teaching hospitals) within the former Yorkshire Regional Health Authority (YRHA). Patients were also identified and tracked from any ED outside this area if the patient was transferred into a critical care facility within the above setting. Minor injuries units (MIUs) were defined as an ED.
Study period
Data were collected for a one year continuous prospective period on all ED transfers of the critically ill or injured adult, from 15 November 1999 to 14 November 2000 inclusive. The first two month period was used as an integrated pilot period to trial data collection systems.
Population
Patients 16 years and older on the day of secondary transport were defined as adult. All patients transferred from an ED within the YRHA into a critical care facility at another hospital were included for study. Other patients deemed by the local contact at each ED to be critically ill were included if thought appropriate by the lead researcher (AG). Any patient transferred into a critical care facility within the YRHA from an ED outside the region was also included.
Patients discharged from hospital who then had another event were hospital admission that resulted in a critical care transfer were considered to be two unique entities.
Data collection systems
Fifteen of the sixteen EDs had an identified member of clinical or audit staff acting as a local contact for the project. The other hospital had a member of staff coordinating data for the whole hospital. These contacts were involved in the coordination and promotion of the project within their department and in particular the completion of study specific data collection forms for all transferred patients. Other sources acted to confirm or provide additional data that were initially unavailable. If a transfer was identified by any source other than a data collection form, the local contact at that hospital, if appropriate, completed a data collection form retrospectively. Patient administration systems and ambulance service data were searched for appropriate additional data. Once this had occurred a set of missing data was collated and returned to local contacts in attempt to find further data. Local and regional intensive care and trauma databases, if appropriate and available, were also searched. An arbitrary cut off of three months after the prospective data collection period had ended was used to finish data collection.
Data were entered and managed on study specific databases developed on Microsoft Access 2000.
RESULTS
A total of 349 critically ill and injured adults were transferred from an ED within the study period. Four of these were from MIUs. Table 1 outlines the key characteristics of the patients including the length of stay at both referring and receiving hospitals and in-hospital mortality.
Patients transferred from an ED (n=349). All figures median and IQR unless stated otherwise
Sites of transfer
Twenty nine EDs transferred patients fulfilling study criteria. Eleven departments transferring 17 (5%) patients were from outside the study area. The median number of patients transferred during the study period was eight (interquartile range 1 to 19). The median number of transfers originating from an ED within the region was 17 (range 1 to 42).
Twenty three hospitals received patients, six of these being across regional boundaries. The median number of patients received by a hospital was three (range 1 to 191).
Figure 1 outlines the principal receiving specialty and receiving department for the transferred patients at the receiving hospital.

Receiving department.
Diagnosis and reasons for transfer
Figure 2 highlights the reasons for transfer identified on transfer from the ED. Table 2 outlines the main presumptive diagnosis on transfer. A toal of 170 (49%) of all patients had trauma as the underlying reason for transfer of whom 101 (29%) were transferred for head injury care. A further 79 (23%) patients required transfer for continuing management of a non-traumatic intracranial pathology.
Main diagnosis of transfer
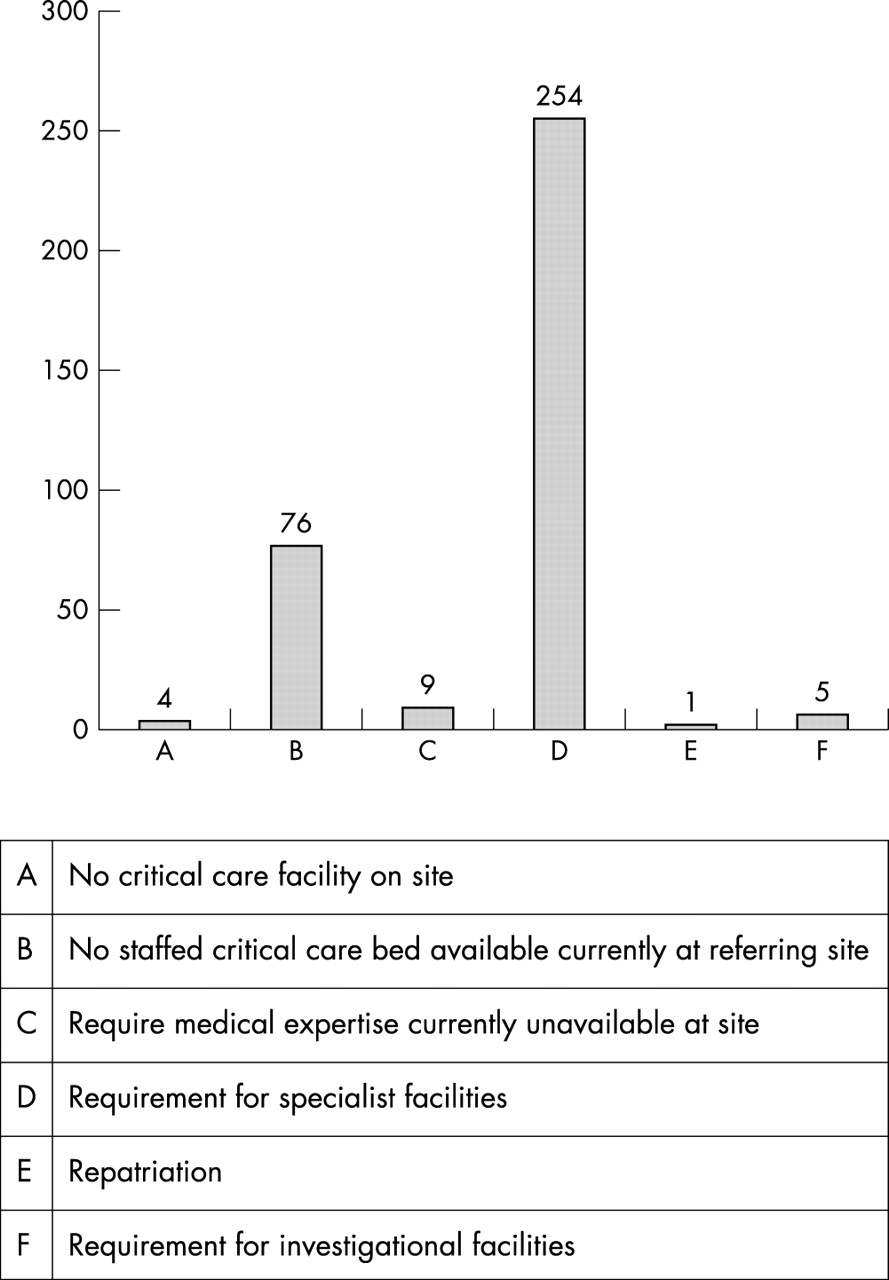
Reason for transfer.
Monthly variation in and time of day of transfer
The median number of transfers per month was 30 (range 19 to 34). The median number of transfers per day was 1 (range 0 to 5). 214 (61%) patients were transferred outside the time period from 08 00 to 18 00. Figure 3 details the hourly variation in number of transfers from the ED.

Seniority of decision making staff and time of day.
Staff involved in decision making and transfer
In 146 (42%) cases the principal clinician making the decision to transfer was the emergency medicine clinician. In a further 93 (27%) occasions the decision was made jointly between emergency medicine and another specialty. The decision making doctor was of consultant grade on 136 (39%) occasions. Figure 3 outlines the seniority of decision making doctor depending on the time of day of the transfer.
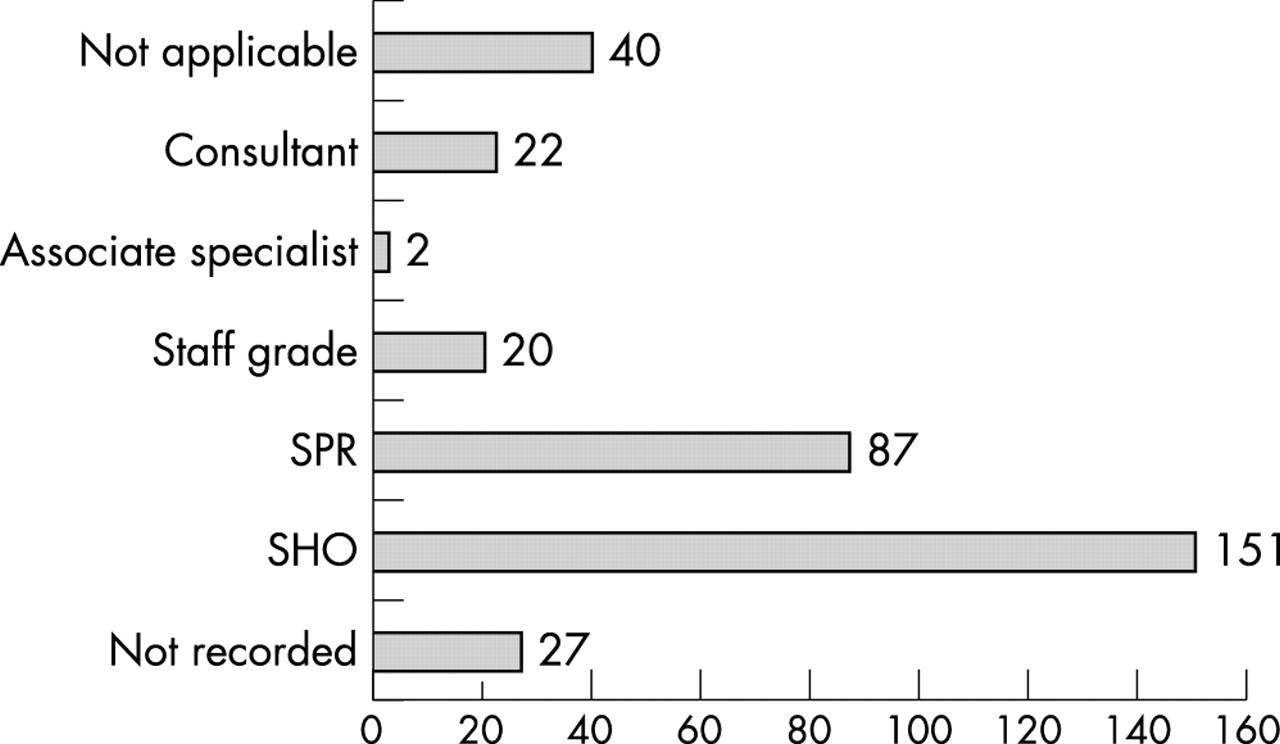
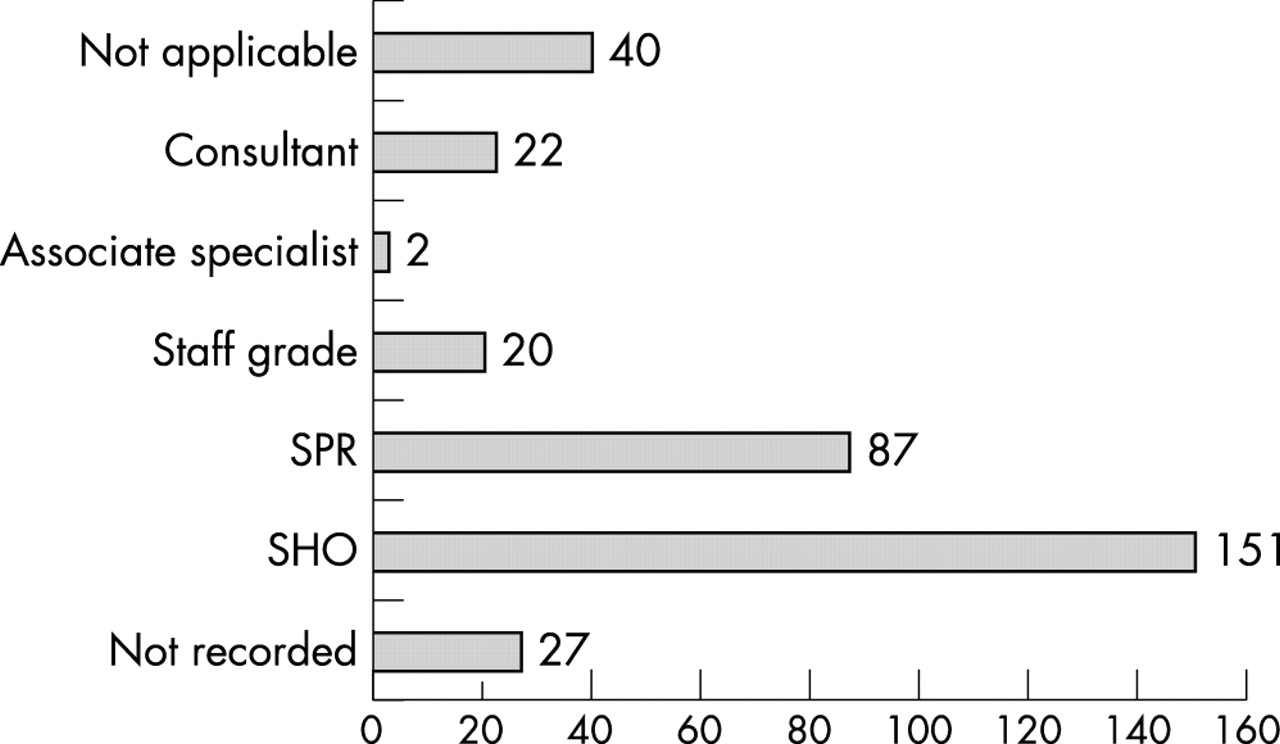
Altogether 308 (89%) patients had a doctor in attendance during transfer. Figure 4 describes the grade of doctor accompanying the patient. A total of 276 (90%) were accompanied by an anaesthetist. Altogether 294 (84%) patients were accompanied by a nurse during transfer of which 271 (92%) were from the ED. Seventy nine (27%) were junior staff at D grade. An ODP and a doctor transferred 22 (6%) patients. A doctor and the ambulance crew transferred 15 (4%) patients. A nurse alone transferred 36 (10%) of the patients. Three patients had no accompanying member of staff other than the ambulance crew during transfer.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Grade of accompanying doctor.
Interventions and monitoring
A total of 251 (72%) patients were ventilated during transfer. Altogether 110 (44%) ventilated patients had end tidal carbon dioxide monitoring during transfer and 195 (78%) had invasive blood pressure monitoring. Seventy one (20%) ventilated patients had central venous access during transfer.
Thirty eight (15%) patients, from 257 with the variable recorded (sensitivity analysis 13% to 19%), had 47 recorded en route critical incidents. These included one patient taken to the wrong hospital and a patient taken to the nearest hospital because of patient deterioration and acute illness of accompanying medical staff.
DISCUSSION
This is the first study to examine, in detail, the characteristics of the critically ill and injured adults transferred from EDs in a defined geographical area in the United Kingdom. The results highlight a number of issues relating to the organisation and process of the critically ill patient requiring secondary transfer from the ED.
The commonest reason for transfer was the need for specialist care. It is of concern, however, that 76 (22%) of patients were transferred for non-clinical reasons such as the unavailability of a staffed critical care bed at the referring hospital. This is alarming given recent recommendations suggesting that if non-clinical transfers must happen then the patient transferred should be the most stable patient requiring critical care6 within the hospital at that time. This is unlikely to be the case for ED patients as they are early in their pathway of care and likely to be at their most clinically labile.
There is considerable emphasis on the management of major trauma within emergency medicine. This group accounts for 170 (49%) of the total number of critically ill transferred.
Fourteen specialties in 12 departments received the patients originating from an ED, highlighting the complexity of the organisation of this group of patients.
Figure 3 outlines the time of day of transfer from the ED, and shows that a large proportion of this patient group present to the ED “out of normal hours” when staffing is at its most stretched with supporting senior staff often not immediately available.
Monitoring levels are poor. Only 44% of intubated patients had end tidal carbon dioxide and 78% invasive blood pressure monitoring during transport despite national recommendations13,14 suggesting these should be minimum standards for monitoring in the critically ill. It is unclear whether this is because monitoring is unavailable or simply not used.
Three patients had no accompanying staff during transfer and 36 (10%) only had a nurse. An appropriate doctor should accompany critically ill patients during transfer as few nurses are specifically trained in this aspect of care. The medical staff, when present, were often junior. During 50% of transfers the doctor was a SHO. Nurses were also frequently junior with 79 (27%) of the nurses accompanying transfers being of only D grade. These findings are concerning in light of published recommendations.13
The recorded critical incident rate of 15% is disturbing as, almost certainly, this represents an underestimate of the true value. This rate is similar to publications describing critical incident rates during the transport of the critically ill within hospital.17,18 Most of the events were potentially preventable by simple measures aimed at improving preparation before transfer. These issues have been highlighted by both training courses10 and previous publications.17,18
Critical care transfers (unpublished data, Alasdair Gray) originating from the ED account for 25%–30% of all transfers and emergency medicine specialists are closely involved in liaison with and organisation of ambulance services. Emergency medicine should, therefore, be central to any organisational developments in transportation of the critically ill and injured. Despite emphasising the need for the whole hospital to be involved in critical care delivery the document Comprehensive critical care5 fails to define how this will be achieved. It is essential for emergency medicine clinicians to be directly involved in critical care delivery at an individual trust and regional level.
This study confirms that the quality of care for this group of patients is suboptimal. There needs to be greater emphasis on training of both nursing and medical staff, better availability of equipment and monitoring, senior clinician involvement in decision making, and robust quality assurance programmes for clinical care to improve.
Interestingly, all YRHA EDs have formal systems for the reception of major injury as a result of a regional trauma accreditation scheme. This includes the presence of a consultant during the patient’s initial assessment, ATLS training for staff, and mandatory clinical audit through UKTARN. However, there are no such systems in place for the management or audit of the critically ill medical or surgical patient. These patients are often managed especially out of hours by junior medical staff. Emphasis needs to be placed on the role of senior emergency medicine staff during the early management of the acutely ill medical and surgical patient. Hospital-wide systems need to evolve to manage these patients. Alternative models of transportation such as, regional transport teams need to be considered and formally evaluated in light of continuing evidence that clinical care during transfer remains suboptimal.
This is a unique regional population based study, which aimed for complete ascertainment of all transfers from the ED of critically ill and injured adults. We examined, in detail, the processes of care received and adverse events.
Previous studies have described the volume of transfers in the intensive care population18,19 and the deficiencies in the quality of care in specific diagnostic groups, such as head injury, both before and after transfer.6–9 These studies were undertaken using questionnaires or cases series with small patient numbers often into a single specialist department and, therefore, are more likely to have inherent flaws in their results.
This is a descriptive study using a mixture of data collection techniques and, therefore, is likely to have some deficiencies in the ability to capture all transfers. Secondly, it is reliant on a large number of individual staff and their interpretation of individual patient events and the process of care. Some data were also collected retrospectively. The reliability and accuracy of some data could be questioned. These could reduce the internal validity of the results. Multiple data sources were used to reduce some of these inherent difficulties by providing data ascertainment. Identification of patients at both ends of the transfer significantly reduced the likelihood of the transfer being missed and increased the probability of pertinent data variables being documented. Often, if a specific study data collection form was not completed at the time of the transfer some data, specifically, monitoring and critical incidents were never available. This does not, we believe, detract from the principal messages of the study.
Conclusions
The transfer of critically ill adults from EDs is a frequent occurrence. A large proportion of patients are transferred for non-clinical reasons and have medical conditions. The quality of care of these patients is poor with a significant critical incident rate, a lack of appropriate monitoring, and junior accompanying staff. The specialty of emergency medicine needs to be actively involved in findings solutions to the inherent problems relating to the transfer of the critically ill and injured adult.
Acknowledgments
The authors would like to thank the steering group of the Yorkshire Critical Care Transport Project and all members of NHS staff who have contributed to data collection.
Contributors
AG designed the study, helped with data collection and inputting, analysed the data, and wrote the paper. SG collected and managed the data. MA and RW helped with the study design and writing the paper. AG will act as guarantor.
REFERENCES
Footnotes
-
Funding: AG has received funding from a regional health authorities research grant to carry out this and other related projects.
-
Conflicts of interest: none.