Article Text

Abstract
Objective: : In 2002 a new protocol was introduced based on the Canadian CT rules. Before this the Royal College of Surgeons “Galasko” report guidelines had been followed. This study evaluates the effects of the protocol and discusses the impact of the implementation of the NICE head injury guidelines—also based on the Canadian CT rules.
Methods: A “before and after” study was undertaken, using data from accident and emergency cards and hospital notes of adult patients with head injuries presenting to the emergency department over seven months in 2001 and nine months in 2002. The two groups were compared to see how rates of computed tomography (CT), admission for observation, discharge, and skull radiography had changed after introduction of the protocol.
Results: : Head CT rates in patients with minor head injuries (MHI) increased significantly from 47 of 330 (14%) to 58 of 267 (20%) (p<0.05). There were also significantly increased rates of admission for observation, from 111 (34%) to 119 (45%). Skull radiography rates fell considerably from 33% of all patients with head injuries in 2001 to 1.6% in 2002, without any adverse effect.
Conclusions: This study shows that it is possible to replace the current practice in the UK of risk stratification of adult MHI based on skull radiography, with slightly modified versions of the Canadian CT rule/NICE guidelines. This will result in a large reduction in skull radiography and will be associated with modest increases in CT and admissions rates. If introduction of the NICE guideline is to be realistic, the study suggests that it will not be cost neutral.
- CT, computed tomography
- MHI, minor head injury
- GCS, Glasgow coma score
- ICI, intracranial injury
- head computed tomography
- NICE guideline
- Canadian CT head rule
Statistics from Altmetric.com
About 0.5–1 million patients present to UK hospitals with head injuries each year. The vast majority of these patients are minor head injuries (MHI)—defined in the UK as Glasgow coma score (GCS 13–15). The clinical challenge in the initial management of these MHI patients lies in the identification of the small subgroup with intracranial injuries (ICI), especially those who will require neurosurgical intervention. This may entail imaging, admission to hospital for observation, or discharge to a safe environment for observation. The radiological investigation of choice to definitively diagnose ICI is a head CT scan. It is generally accepted that patients with moderate or severe head trauma (GCS 3–12, post-traumatic seizures, focal neurological deficit) should be scanned urgently.
Imaging practices for patients with MHI, however, vary widely around the world. In the USA head CT scans are used extensively for MHI in accordance with ATLS.1 This results in very high rates of CT. British practice for MHI imaging was based up until 2003 on various guidelines, available from the Royal College of Radiologists,2 the Society of British Neurological Surgeons (SBNS),3 the Royal College of Surgeons of England (RCSE),4 and the Scottish Intercollegiate Guidelines Network,5 predominantly derived from either literature surveys or consensus. Hospital practices consist mainly of a mixture of skull radiography to identify fractures—which increase the risk of ICI—CT, or observation, depending on the guidelines in use and local resources.
GUIDELINES
The Canadian CT head rule published in 20016 was developed as a clinical tool to predict which MHI patients will have ICI on CT and consequently reduce the number of CT scans performed in North America. Skull radiography has no role in the management of MHI. Implementation of the Canadian CT head rule to UK practice could result in greatly increased CT rates: it has been estimated that if the “high risk” criteria of the rule were applied to the UK (box) CT would be indicated in a third of patients with MHI.7,8 Current baseline CT imaging rates are around 10%–15% of MHIs in the UK.7,8 The addition of the “medium risk” criteria will result in even higher rates.
Clinical variables identified by the Canadian CT head rule for the selection of patients with minor head injuries (GCS 13–15) for CT
High risk (for neurosurgical interventions)
-
GCS score <15 at two hours after injury
-
Suspected open or depressed skull fracture
-
Any sign of basal skull fracture (haemotympanum, “panda” eyes, cerebrospinal fluid otorrhoea, Battle’s sign).
-
Vomiting more than once
-
Age≥65 years
Medium risk (for brain injury on CT) *
-
Persistent retrograde amnesia of greater than 30 minutes
-
Dangerous mechanism of injury (pedestrian struck by vehicle, ejection from vehicle, fall from greater than three feet or five stairs)
All rules and guidelines consider the following to be signs/risks of moderate or severe head injury and warrant urgent immediate CT:
-
GCS<13
-
Post-traumatic seizure
-
Focal neurological deficit
-
Coagulopathy (history of bleeding, clotting disorder, current warfarin treatment)
In June 2003 the National Institute of Clinical Excellence (NICE) released the guideline “Head injury in infants, children and adults: triage, assessment, investigation and early management”.9 The CT recommendations of this important new guideline for MHI are similar to the Canadian CT rule but with some modifications: CT can be delayed up to eight hours in those with “medium risk” criteria, and coagulopathy is a “high risk” indication for CT. Adoption of the NICE guideline in the UK for MHI would thus result in similar rates of CT, with concomitant resource implications.
In 2002 we introduced a new protocol at Addenbrooke’s Hospital, based on the Canadian CT rules. Before this we were applying the SBNS/RCSE guidelines.3,4 Here we evaluate the effects of our new protocol and discuss the implications of the implementation of the NICE guidelines to the UK practice.
PATIENTS AND METHODS
The Cambridge protocol
The care of all head injury patients at Addenbrooke’s Hospital is shared between the on-site regional neurosurgical unit (RNSU) and the emergency department (ED). Up until 2001, our management of MHI was based on the SBNS/RCSE guidelines (see reference 4: appendix A page 43): a mixture of skull radiography, CT, and admission to the observation ward. We had already identified from our earlier study7 that the strict implementation of the Canadian rules would lead to a large increase in requests for CT (from 14% to between a third to a half of MHIs).
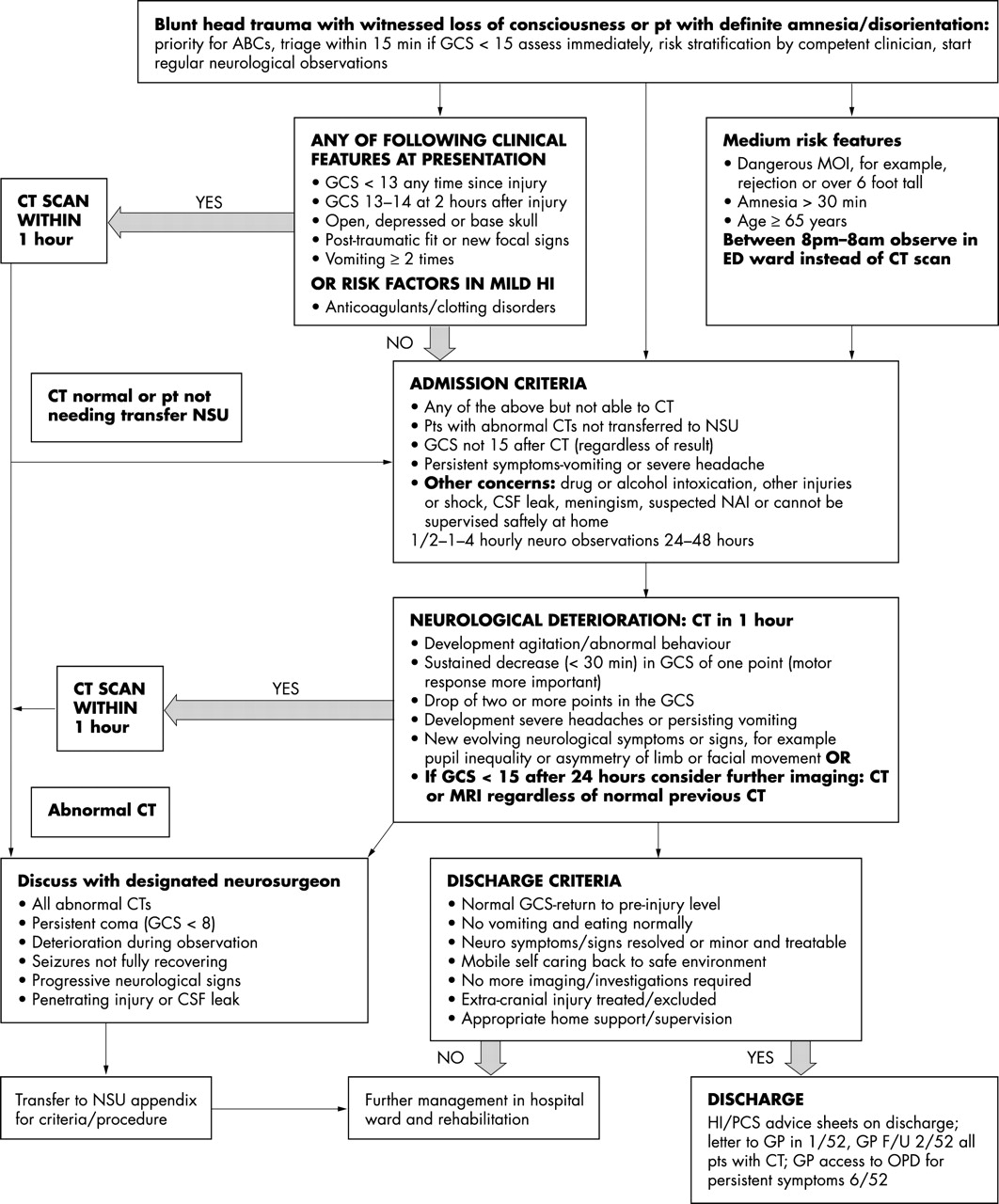
We designed the new pilot protocol for MHI patients and introduced it in January 2002 after discussion and agreement with the departments of neurosurgery and neuroradiology (fig 1). Its objectives were to instigate a policy of risk stratification that would identify those MHI patients that had ICI. We based it on the Canadian CT rule and adapted it to our local set up. Skull radiographs were no longer to be requested for MHI, unless obvious depressed skull fractures or penetrating injury were suspected.

“Cambridge” protocol for minor head injury patients at Addenbrooke’s Hospital introduced in January 2002. Initial management is based on the Canadian CT rules.
The easy access to CT during daytime when both CT scanners are fully operational enabled the full implementation of the Canadian CT rules in our hospital. However, the out of hours service is for emergencies only, rationed by the radiology department and based on patients’ clinical need. Certain modifications were agreed by the three departments to reduce the out of hours demand to manageable levels: between the night hours of 8 pm to 8 am patients with “medium risk” indications for CT (under the Canadian rules, amnesia before impact >30 minutes, or dangerous mechanism,) and those aged >64 but without “high risk” indications, were observed in the ED observation ward overnight instead of having CT immediately. Deterioration in these patients (see protocol for definition) was considered to be an indication for obtaining urgent CT at night. It was felt that the risk of missing surgically significant ICI in this group of patients was very small and the safeguards to identify deterioration adequate. ED consultants routinely perform morning ward rounds and would only request a CT scan in this group of patients if clinically indicated. Implementation of the protocol was carried out by medical staff of all grades in the relevant departments from 1 January 2002.
Methods
We conducted a “before and after” study, using information from ED cards and hospital notes of adult head injured patients (age>15) presenting to the ED over two distinct periods. We aimed to identify all possible adult patients with MHIs. The first period of seven months was 1 April 2001 to 31 October 2001. This formed the “baseline” group. The second period of nine months, subsequent to the introduction of the protocol, was 1 January 2002 to 30 September 2002.
Case notes of patients were identified using routine departmental codes indicating any trauma to the head, face, or “multiple injuries”. They were reviewed individually to confirm they were appropriate for inclusion. We also examined all cases that had had a CT scan of the head or skull radiography if these had not already been identified from their codes. Our hospital uses standardised “head injury forms” for recording clinical data on patients with head injuries. This facilitated consistent data collection. All the relevant parameters for the study were extracted from all possible sources: the ED forms/notes, the hospital records, computer systems, and radiology archives. The data were entered on a spreadsheet by two researchers for the 2001 period and four researchers for 2002 using the same definitions throughout. From the total pool of head injuries we identified cases that fulfilled the Canadian definition of MHI—patients with a GCS of 13–15 on presentation with witnessed loss of consciousness or amnesia/disorientation, subsequent to blunt head trauma. Patients were excluded if they had moderate or severe head injuries (GCS<13) or unstable vital signs, focal neurological deficit, penetrating injuries, or did not experience loss of consciousness or amnesia/disorientation as a result of their head injury. Cases were also excluded if there was no clear history of trauma as the primary event (for example, syncope, seizure), or if the data were incomplete such that the head injury protocol could not be applied. MHI data from the 2001 and 2002 periods were compared using χ2 tests for differences between proportions using Stata statistical software version 7.
RESULTS
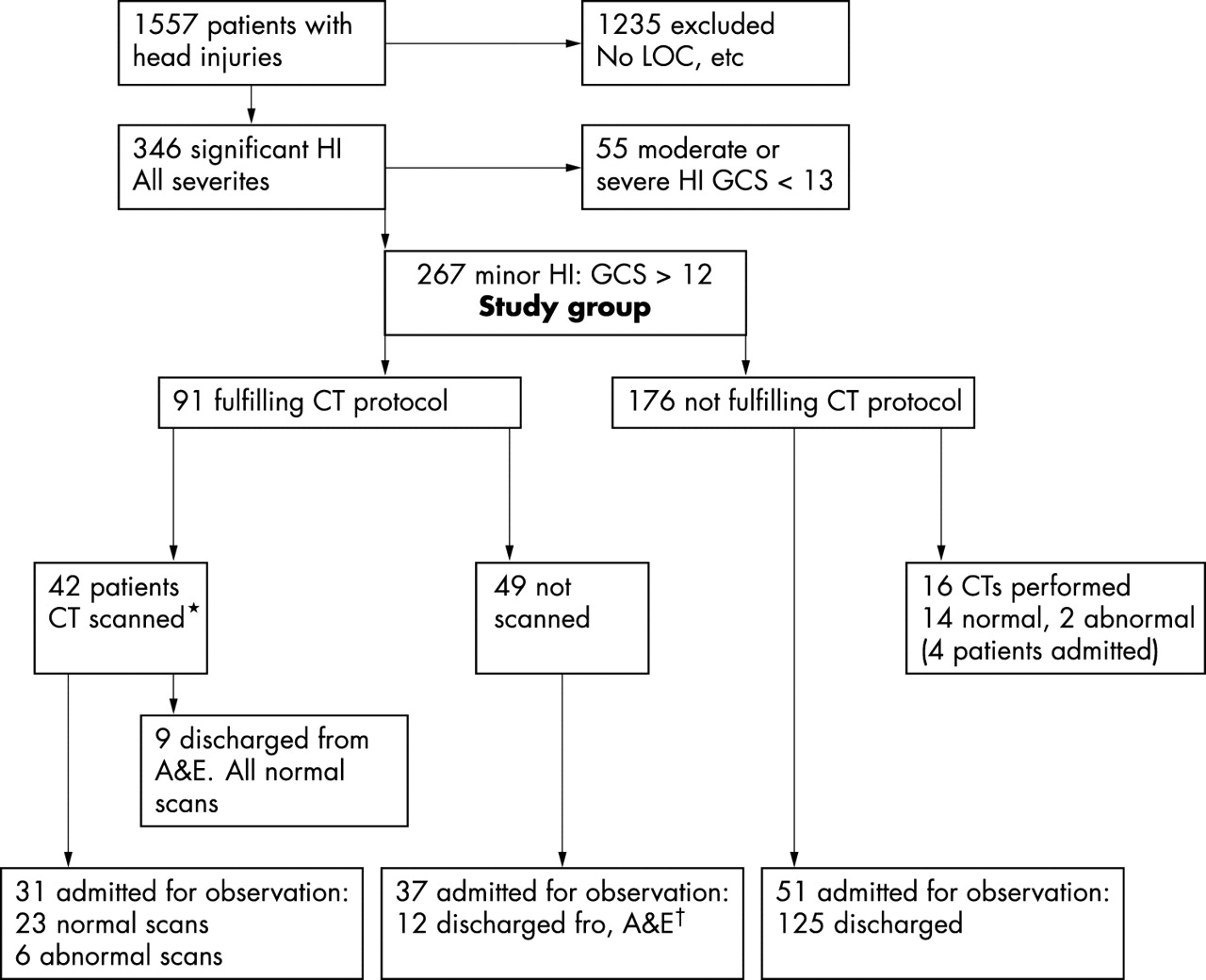
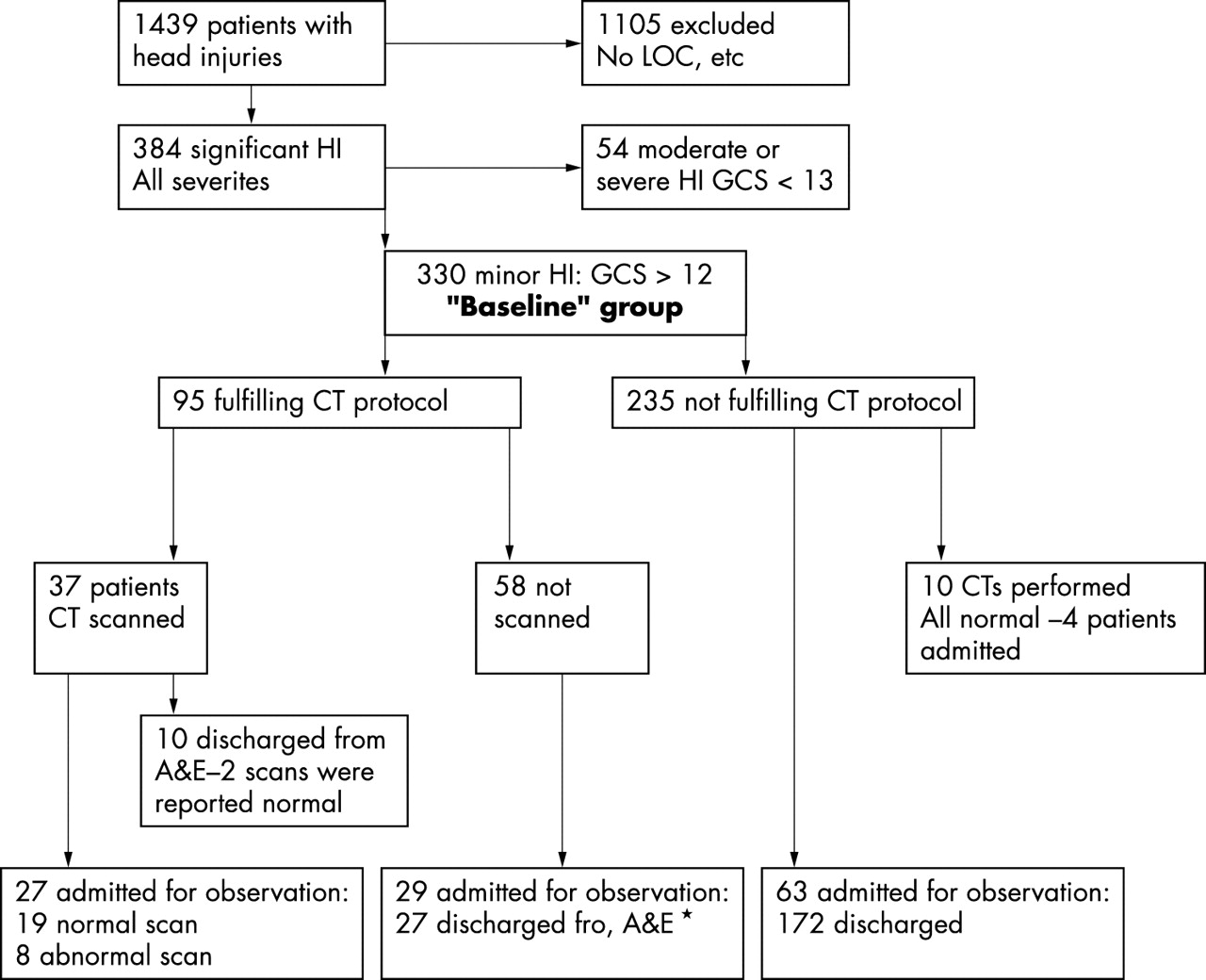
The Addenbrooke’s ED saw 56 614 new patients in 2001 and 58 768 in 2002. The breakdown of all head injury patients presenting during the two trial periods, and their care pathways, are shown in figures 2 and 3. In 2001, 1489 case notes were examined with adequate notes and clear data over a seven month period. Of these, 48 patients were classified moderate or severe head injuries, had a GCS of <13, or another clear indication for CT (for example, unstable vital signs, focal neurological deficit, and seizures) and were excluded. In 1110 patients there was no loss of consciousness, disorientation or amnesia, or any obvious penetrating injury. This left 330 cases that fulfilled the Canadian definition of MHI. For the 2002 period, 1557 case notes were examined over nine months. Altogether 1235 of these had no loss of consciousness and 55 were moderate/severe HI, (GCS of <13). These were excluded as above, leaving 267 eligible patients. Thus, the 330 patients from 2001 and the 267 from 2002 formed the two groups for comparison and statistical analysis.
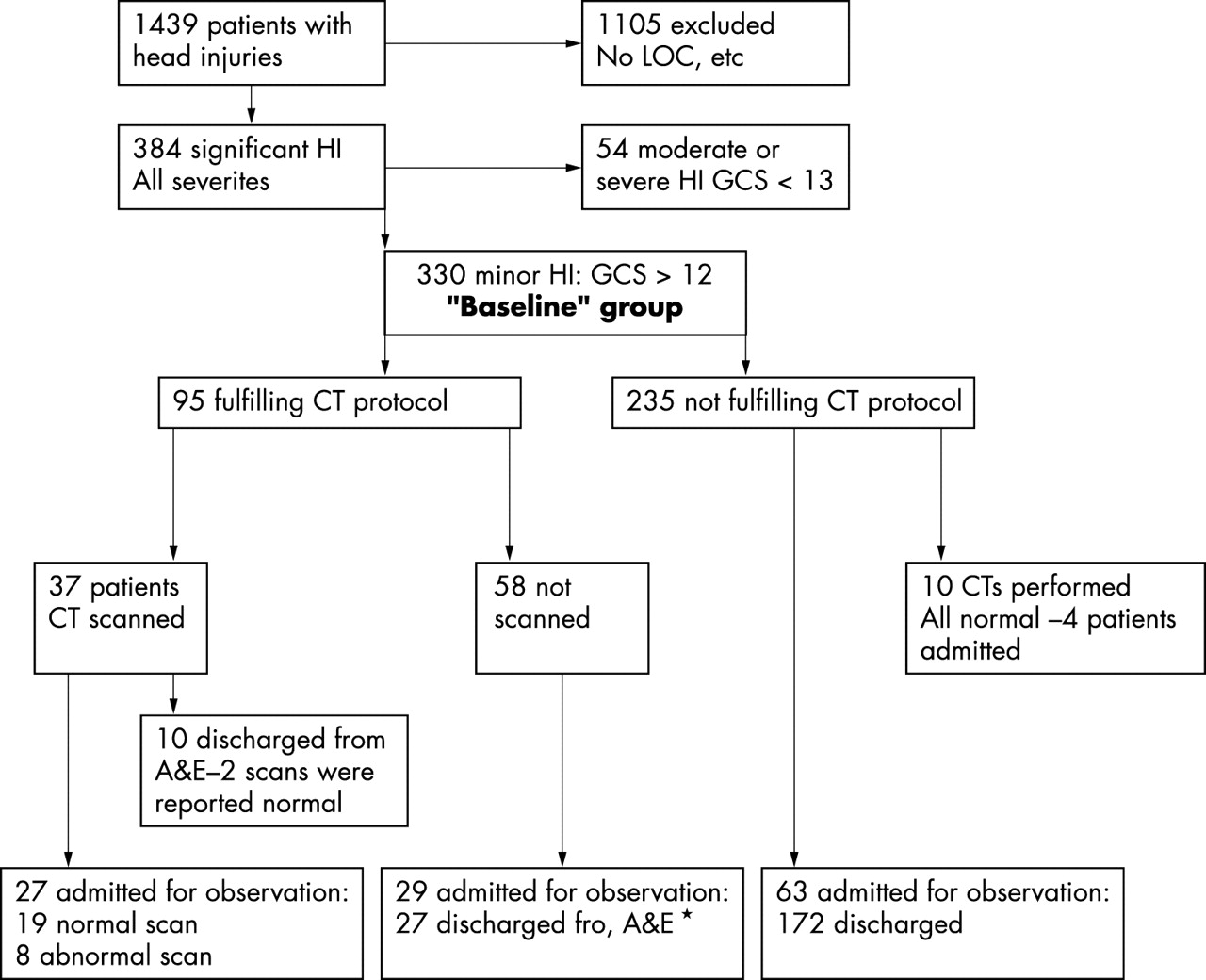
Summary of 2001 data. All patients with head injuries (HI) for the seven month control period are included. Royal College of Surgeons guideline for CT was in operation when the patients were treated. The Canadian CT rule for CT was applied retrospectively to determine how many patients would fulfil it. *Two sets of case notes were not available and could not be confidently include in this part of the analysis.
{kind=link}
{kind=link}
{kind=link}
Summary of 2002 data. All patients with head injuries (HI) for the nine month control period are included. The new protocol was introduced and in operation when these patients were treated. The Canadian CT rules were applied to determine how many patients fulfilled the criteria for scanning.*Two sets of case notes were not available and could not be confidently included in this part of the analysis. †These patients were discharged with written HI advice and relatives told to contact the department or return if the patients deteriorated. None returned.
The radiological investigations performed on MHI patients during the two study periods are summarised in table 1A. We applied the Canadian CT head rule to the MHI in the two groups. The proportion of patients fulfilling the criteria was similar in the groups; the slight increase from 95 of 330 (29%) in 2001 to 91 of 267 (34%) in 2002 was not significant. The total number of head CT scans performed had significantly increased from 47(14%) in 2001 to 58(20%) in 2002. This was attributable to an increase in those that fulfilled the CT rule—37(11%) in 2001 to 42(16%) in 2002—as well as those that did not—10 of 235 (4%) in 2001 compared with 16 of 176 (9%) in 2002. The increased rates of scans in these subgroups, though individually too small to be statistically significant, when combined results in a significantly greater overall CT rate in 2002. Changed GCS and age>64 were the two clinical indications accounting for the increase in CTs among those fulfilling the protocol criteria. The proportion of abnormal CT scans was similar in both years—10 (3%) in 2001 and 8(3%) in 2002.
Comparison of management of minor head injuries in 2001 and 2002: radiological investigations
The total number of skull radiographs performed had fallen dramatically, from 220 (67%) in 2001 to 15 (4%) in 2002, for the MHI patients. In fact the reduction in skull radiography was even more pronounced. In 2001, during the seven month study period a total of 490 of 1489 (33%) skull radiographs were requested on all adult patients with head injuries—some of them did not lose consciousness and were therefore not in the MHI group—compared with 27 of 1557 (1.6%). Review of the individual case notes showed that the radiographs that were performed in 2002 were done in patients with deep scalp lacerations to exclude glass foreign body or underlying depressed skull fracture, or because one clinical assistant was unaware of the protocol for part of the study period. None were performed for the purposes of risk stratification after head injury.
The management of the MHI patients was compared (table 1B). The total proportion admitted for observation increased significantly from 111 (34%) in 2001 to 119 (44%) in 2002. Analysis of subgroups of those admitted for observation showed an increase in admissions among those who fulfilled the CT criteria of our protocol: 56 (17%) in 2001 compared with 68 (25%) in 2002. This was true whether or not they actually received a CT scan. The increase in those scanned and admitted (27 (8%) in 2001 compared with 31 (12%) in 2002) was not significant but it was significant in those not scanned but admitted 29 (9%) in 2001 compared with 37 (14%) in 2002. The admission rates of MHI patients who did not fulfil CT criteria did not change (19% in both years). This suggests that admission for observation was used as an alternative to CT as anticipated by the operation of our protocol during the night time. Interestingly, even when patients did receive a CT scan this did not reduce admission rates. Other reasons necessitated their admission: elderly people living alone, presence of alcohol, or other comorbidities.
Comparison of management of minor head injuries in 2001 and 2002: admission/discharge
No adverse incidents were reported during this period regarding “missed” brain injury pathology. As Addenbrooke’s Hospital is a regional tertiary referral centre for neurosurgery with close links between the two departments we were able to ascertain that no patients who had been discharged without a CT scan subsequently returned, either requiring a scan or requiring neurosurgical intervention.
DISCUSSION
Patients with moderate or severe head injuries are managed by aggressive resuscitation along ATLS guidelines and urgent CT. However, the management of patients with minor head injuries is variable and especially dependent on CT resources in UK hospitals. In 2002, we introduced in Cambridge, the Canadian CT rule slightly modified to our resources and setting. We applied the rule fully during the day and relied on observation at night for those with “medium risk” indications and for the elderly population (aged>64) without high risk indications. The NICE guideline, published in 2003, 18 months after the application of our protocol, is likewise based on the Canadian CT rule. Although we did not formally test the NICE guidelines, our modifications to the Canadian rule meant that for 12 hours of the day the NICE guidelines were in fact in operation. We therefore believe this study is relevant to the discussion on the impact of the NICE guidelines in the UK.
The results show that it is possible to introduce in the UK a system for risk stratification of MHI that does not rely on skull radiography. We are not aware of any other reports describing a similar practice in Britain. The huge reduction in skull radiography was associated with modest increases in CT and admissions rates. The prediction that implementation of the Canadian CT rule (and hence NICE) would result in CT for a third to a half of all MHIs7,8 did not materialise mainly because of the modifications to the rule for the 12 hours of night time. These “low risk” patients admitted overnight were mainly discharged the next day without CT. This common sense modification caused least disruption within the radiology department. Often there were other reasons preventing the discharge of these patients: elderly people living alone, comorbidities, and presence of alcohol and unsafe home supervision. It is difficult to justify CT scans out of hours, as these patients would still require admission. The NICE guideline permits an eight hour delay of CT for patients with “medium risk” indications. We felt that it was safe to observe this subgroup as well as the elderly population with no high risk indications, as long as the appropriate safeguards were in place, namely immediate CT if there were any signs of deterioration. Because the rate of occurrence of surgically significant traumatic haematomas in MHIs is very low, the possibility of missing such pathology in these “low risk” MHI patients is even much smaller. There were no adverse events with missed traumatic brain pathology subsequent to these changes but we have not collected sufficient numbers of patients to show that this approach is completely safe. A very large multi-centred study will be needed to consider this aspect. Until such a study is conducted, we believe that the risk of missing a surgically significant injury in the subgroups described is very small indeed and acceptable if the modifications are accompanied by the precautions.
The other important finding of our study is that the implementation of the protocol did not reduce admissions, as predicted by the Canadian study or the NICE Guideline.6,9 There was no increase in the proportion of abnormal scans to explain the increased admission rate. As explained above there are many reasons why MHI patients with normal CT scans cannot be discharged. This probably reflects an increase in “social” admissions of MHI patients and the caution on the part of junior doctors secondary to increased awareness of MHI management. Thus it does not seem that implementation of the Canadian head CT “5 point rule” will save resources by reducing admission rates as suggested by the detailed cost effectiveness analysis by NICE.9 Although we did not carry out a detailed economic evaluation, our experience shows that overall costs were probably higher after the introduction of the protocol because of the increased rates of admission, as well as the increased rates of CT scan. These costs would not be adequately counterbalanced by the reduction in skull radiography. However, we were able to accommodate these changes within our hospital’s current resources and arrangements. Furthermore, we have continued to use our protocol since its introduction in January 2001 and do not intend to make any further changes after the publication of the NICE guideline.
The above points illustrate the practical difficulties of trying to follow the Canadian rule or NICE guideline, even in a department where head CT is comparatively easily available. In a recent editorial, Yates10 acknowledges the service issues raised by the introduction of the NICE guideline and suggests a phased introduction of the guideline, together with audit of guideline use and effectiveness, to detect potential adverse consequences of guideline implementation early on. Our study supports this and suggests that it may be unrealistic to aim to CT all the patients who fulfil the CT rule within the UK medical framework. Admission of the “low risk” MHIs for observation may be a more feasible alternative, especially in departments with more restricted access to CT. We feel it is likely that many departments will experience significant difficulties in trying to implement the new NICE guidelines until these issues are resolved. Training emergency physicians to interpret CT scans out of hours may be one way in which hospitals with scarce radiology resources may implement these guidelines.
CONCLUSION
This study shows that it is possible to replace the current practice of risk stratification of adult MHIs based on skull radiography, with a slightly modified version of the Canadian CT rule or NICE guidelines. This will result in huge reduction in skull radiography and will be associated with modest increases in CT and admissions rates. Although there were no adverse events subsequent to the introduction of these changes, the numbers of patients recruited were not sufficient to show conclusively that this is completely safe—a large study is needed for this. If introduction of the NICE guideline is to be realistic, this study suggests that it will not be cost neutral. Modifications may be needed for some patient subgroups, and to allow for the resource limitations operating within individual departments.
Acknowledgments
We thank the neurosurgery department for their help with the protocol and their support for its implementation, in particular Professor J D Pickard and Mr P Hutchinson for their useful suggestions about the paper. We are also grateful to those who also contributed to the data collection—AB and Dr L Santarius in 2001 and MP, HYS, Dr F Garbutt, and Dr M Legeyt in 2002. We also thank the EMJ reviewers of the paper for their helpful comments.
CONTRIBUTORS C Maimaris and N Antoun designed and introduced the protocol, CM was in charge of its implementation and in supervising the collection and analysis of data, editing and, revising the paper and acts as the guarantor of the study. AB analysed and interpreted the data and did revisions. HYS and MP assisted in the data collection and all authors contributed to the writing of the paper.
Footnotes
-
↵* These two indications were found by the Canadian study to produce abnormal CT scans but not neurosurgically significant injuries. The NICE guideline recommends that patients with these two indications only can have their CT delayed up to eight hours from injury.
-
Funding: none.
-
Conflicts of interest: none declared.