Article Text

Abstract
A simple algorithm has been produced to assist front line ground ambulance personnel, air ambulance crews, and immediate care doctors attending trauma patients in selecting the most appropriate mode of transport from the incident scene to hospital.
- transport
- trauma
- helicopter
- algorithm
- prehospital care
- ED, emergency department
- RSI, rapid sequence induction
- GCS, Glasgow coma score
Statistics from Altmetric.com
A recent review article1 has raised a number of important practical issues for clinicians attending the scene of a road traffic accident, many of which have been amplified by other correspondents.2,3 One matter that remains unclear, however, is the most suitable mode of transport to move injured patients from the scene to hospital. A retrospective review of 1000 trauma deaths in the UK in 1988 made recommendations that prehospital and hospital delivered care for seriously injured patients should be improved, along with better transport systems to major centres.4 Increasingly, ambulance services in the UK may have the services of an air ambulance available as an additional resource. Police, search and rescue, and military helicopters, with potentially limited medical equipment and clinical resources, may also be available to transport patients in an emergency.
The decision to use a helicopter is not straightforward, and a number of important geographical, physiological, and pathological factors need to be considered.
The transfer of a seriously injured patient by helicopter may be hazardous and transportation by road may often be a safer option.
Other factors, including the clinical skills and experience of the helicopter crews, also need to be considered. Currently only one UK air ambulance, for example, is funded and manned for all its operational hours by a doctor-paramedic team trained in prehospital critical care.5
Knowledge of the resources at and journey times to local district and regional hospitals, and the location of their helipads or nearest landing sites, also needs consideration. A detailed estimate of total transport time from scene to hospital is required to ascertain whether road or air ambulance transfer will offer the fastest mode of transport to hospital. When a helicopter is requested by a ground crew already on scene helicopter mobilisation and flight times may delay transfer times further. Road ambulance transfer is often a faster mode of transport than secondary air ambulance transfer in the UK.6
We have failed to identify in the literature any comprehensive guidance on these issues suitable for field use. A telephone survey of England’s air ambulances by one of the authors (JB) confirmed that air ambulance paramedics usually have to rely on their “professional judgement” to make potentially complex transport decisions.
Our algorithm considers the variables described and attempts to guide decision making in a logical and systematic way.
METHODS
This algorithm has been written after a critical evaluation of the available prehospital care literature after searching Medline, EMbase, the Cochrane Library, the world wide web, and participating in internet trauma discussion groups.7 The authors have consulted ambulance services, immediate care schemes, and hospital medical colleagues in developing this decision tool, and have also used their own prehospital critical care experience and hospital practice to refine this algorithm.
As the clinical priorities of patients at the scene are no different to those in the emergency department (ED) resuscitation room,8 the authors have applied analogous existing best practice transport guidelines for patient intrahospital transfer between departments9,10 (for example, ED to the CT scanner). The risks of adverse clinical outcome in transferring unstable injured patients from the ED resuscitation room to the CT scanner are well known in hospital practice. We have also applied similar existing guidelines used for interhospital transfer of critically ill9–11 and injured patients12 when considering helicopter transfer.
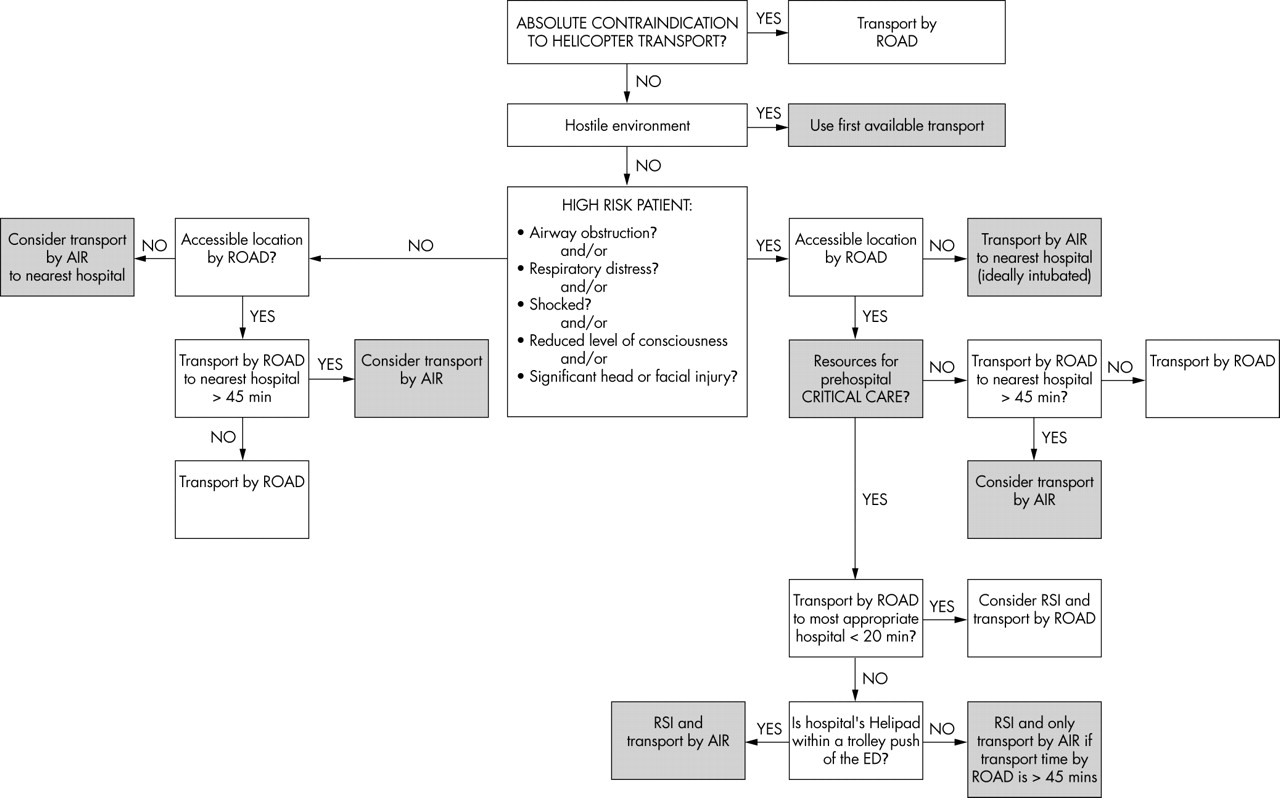
The part of the algorithm relevant to physiologically compromised patients with access to critical care interventions in the field, for example, rapid sequence induction (RSI) and tracheal intubation, is influenced by current transport practice at the helicopter emergency medical service based at the Royal London Hospital (HEMS London) in the UK13,14 and current practice in many European and US emergency medical services. The parts of the algorithm relating to patients without adverse critical signs or injury, and those without access to critical care interventions, has yet to be critically evaluated (fig 1).
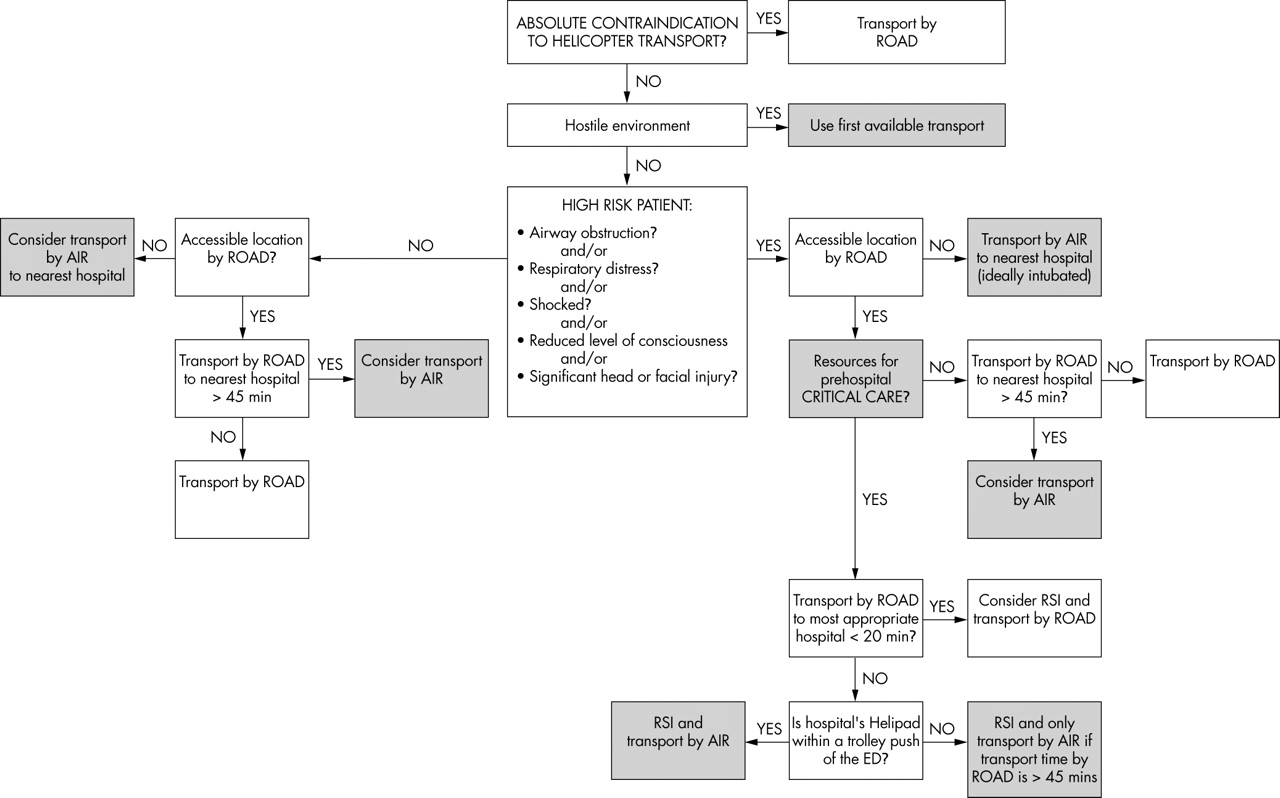
Prehospital trauma transport algorithm.
DISCUSSION
This algorithm has been designed to be widely applicable by using simple physiological values that can easily be determined by ambulance crews, air ambulance paramedics, and immediate care doctors to guide potentially complex transport decision making for injured patients at scene. It is also designed to identify patients with adverse clinical signs and injury patterns that predispose to decompensation and secondary injury during transport. Critical care interventions are performed to reduce the risk of life threatening secondary injury from hypoxia, hypercarbia, and hypotension occurring during transport. It may not be possible to readily identify and effectively manage deterioration in flight.15 Unless there are the clinical resources to deliver critical care at the scene, it may be safer for patients to be transported by road, accepting longer transport times to hospital.
The key factors for determining the most suitable mode of transport are
-
Access to a suitable helicopter/road vehicle
-
Environmental conditions
-
Contraindications to helicopter transport
-
Patient’s physiological status
-
Presence of specific injury patterns
-
Accessibility to the incident location by road and air
-
The availability of resources to deliver prehospital critical care interventions (fig 2), principally rapid sequence induction and tracheal intubation at the scene
-
Total transfer time from scene by road to hospital (blue light ambulance) compared with helicopter (including packaging and loading, flight and transfer time from helipad to the hospital’s emergency department)
-
Resources of local receiving hospital(s).
{kind=link}
{kind=link}
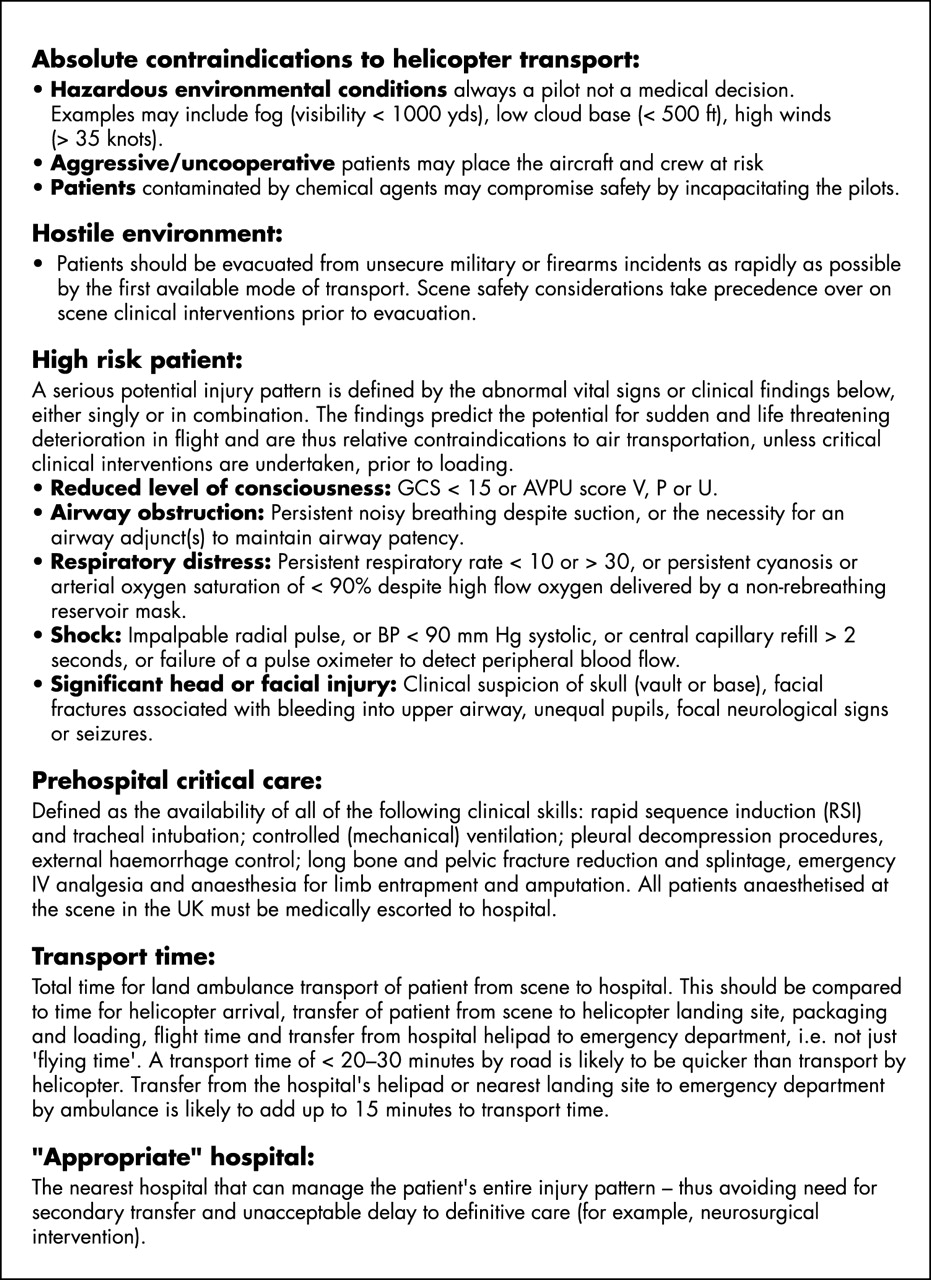
Definitions and notes for use of transport algorithm.
The environment
Poor weather as defined in figure 2 may preclude helicopter transfer. Under these circumstances road transport is usually the only option.
We have emphasised the rare situation of casualty contamination with noxious agents because this situation is an absolute contraindication to air transfer. Of particular concern are chemical warfare agents, agricultural pesticides, and organic solvents, which may contaminate and impair pilots. If there is any doubt patients must be transported by road to hospital.
Cerebrally irritated, aggressive, and uncooperative patients may also jeopardise safety within the limited confines of air ambulance helicopters. In our view these patients can only be safely transported by helicopter sedated, intubated, and ventilated. Many such patients have a Glasgow coma scale of up to 14 or an AVPU score of V. The threshold for securing a definitive airway for helicopter transport in this context is low even though some of these patients may not have sustained life threatening head injury.
Patients being retrieved from a hostile environment (for example, from an unsecured military setting or fire arms incident), may have to be evacuated in extremis by helicopter without prior critical care intervention, even if available.16,17 In such environments, evacuation takes precedence over prior clinical interventions, because of scene safety considerations for rescuers. Patients should be evacuated from these environments by the first available means of transport. This is rarely applicable in the civilian environment.
Adverse clinical signs
Patients who are potentially unsuitable for helicopter transport are identified by abnormal physiological variables, either alone or in combination, in the adverse clinical signs box of the transport algorithm (figs 1 and 2). These findings correlate with the potential for life threatening injury pattern, airway obstruction, failure of oxygenation and ventilation, and exsanguination either at the scene or during transport to hospital. Other authors have validated that derangements of respiratory rate, pulse rate, blood pressure, and conscious level, either alone or in combination, accurately predict serious injury patterns, and justify field triage directly to regional level 1 trauma centres in the USA.18 Reduction in level of consciousness to an AVPU score of P or less predicted an injury severity score (ISS) of >15 with a sensitivity of 93% and a specificity of 85%.18 Similar physiological observations used to derive the prehospital index have been used to justify and validate timely interhospital transfer to a level 1 centre in Canada.19 The ability to effectively and safely manage potentially reversible causes of deterioration will be determined not only by the resources available at the scene (equipment, clinical experience, and skill mix of paramedics/doctors), but also by whether an aircraft or land ambulance is used for transportation. Ideally conditions that may cause critical deterioration during transfer should be dealt with on scene before transport. It may not be possible to safely and effectively undertake these interventions during flight.15 These issues must be considered from the outset by those responsible for triage and transport decisions at scene.
Detection of airway obstruction in flight may not be straightforward because of the noise, vibration, and restricted access to the patient in the aircraft cabin. In-flight treatment of the unintubated, vomiting patient, can be very difficult. Although suction should be available, the patient is likely to be supine, and their spine fully immobilised. Turning, log rolling, or placing patients head down, can be impossible because of securing harnesses, lack of space, and the design of aircraft stretchers.
The use of airway adjuncts (oral and nasal) will contribute to airway maintenance but will not protect against aspiration in compromised patients. Their use, however, does help to predict the need for a definitive airway.20 Establishing a definitive airway in-flight is fraught with difficulties in civilian rotary wing aircraft because of lack of patient access and difficulties in verifying correct tracheal tube placement. For safety and communication purposes flight crew are likely to be wearing helmets, which creates further difficulties in clinical assessment. For these reasons, any degree of airway obstruction is a relative contraindication to helicopter transport unless a definitive airway can be secured before departure. If the resources for prehospital critical care are not available at the scene, but the scene has road access, then it may be safer to transport such patients by land ambulance to the nearest hospital using basic airway maintenance techniques. This algorithm recommends that if the journey time by road is likely to exceed 45 minutes, and there are no resources for on scene critical care as defined in figure 2, then helicopter transport should still be considered. This requires finely balanced clinical decision making. This should be a relatively rare event except in the most remote parts of the United Kingdom. Aggressive airway management in this setting reflects current best practice from the interhospital transport of critically injured patients.9,10,12,21
Respiratory distress, as defined in figure 2, may occur as a consequence of partial airway obstruction, simple or tension pneumothorax, direct lung injury, high spinal cord injury, or metabolic acidosis secondary to shock. This is a valuable predictor of potential deterioration during transport, in both the prehospital and hospital phase.9–11 Ventilatory failure mandates aggressive critical care especially when associated with head injury.21,22 Lack of space will also make performing other necessary lifesaving interventions, for example, pleural decompression procedures, more technically difficult in-flight. This is the reason why respiratory distress is emphasised as an important relative contraindication to helicopter transport unless there are resources for critical care interventions (fig 2). These interventions, including RSI, should be performed at the scene before transport if necessary. Should the patient’s condition deteriorate during transport then interventions may be more safely performed in a (stationary) land ambulance than in the air. A simple pneumothorax not compromising oxygenation in an unventilated patient may not require any intervention in the first instance, and is not in itself a contraindication to helicopter transport provided they are transferred at low altitude that is normal practice for most UK air ambulances.
Shocked patients are also at risk of developing airway obstruction as a consequence of inadequate perfusion. Previous trauma series have shown that up to 30% of severely injured patients from blunt trauma are likely to die from exsanguination within two hours of injury.23 Seventy per cent of similar exsanguination deaths occurring in London in the 1970s occurred within 30 minutes—many of these within 15 minutes.24 A proportion of these patients may have survivable injury patterns, especially with judicious fluid replacement.25 It is therefore essential to establish the presence of shock when considering triage and transport decisions at the scene. Triaging these patients directly to a multidisciplinary trauma hospital should be done if one is available locally—previous studies have shown improved survival in such centres in the USA26 and UK.27 However, less than 5% of severely injured patients arriving at hospital will require emergency trauma laparotomy for haemorrhage control in the first eight hours after admission to the ED.28 For this reason, it may well be justifiable to accept longer transport times by road if there is no critical care skills at scene, even if a helicopter is potentially available. Patients in extremis without access to prehospital critical care, should however be transported to the nearest emergency department as safely and as rapidly as possible—this may well be most appropriately achieved by road particularly if transport times are less than 45 minutes, accepting that many such patients may not have survivable injuries.29,30 Patients in traumatic arrest should not be transported by helicopter to hospital as there is considerable experience demonstrating no survival benefit in this scenario,31 and unrestrained flight crew may be exposed to unacceptable risk.
Life threatening penetrating trauma to the head, neck, and trunk remains comparatively rare in the UK when compared with the USA.32 It most commonly occurs during interpersonal violence in inner cities when road transfer times to adjacent hospitals are usually comparatively short. The major determinant for survival for life threatening penetrating injuries is time to definitive care.33 Penetrating injuries to the head should be managed as per serious blunt head trauma as determined by level of consciousness (see below). Penetrating injuries to the neck (see below), trunk, and extremities should, in the authors’ opinion, be transported to hospital as rapidly as possible with minimal on scene intervention other than supplemental oxygen and external haemorrhage control. Helicopter transport is rarely likely to hasten transport to hospital.34 Prehospital thoracotomy for haemorrhage control and relief of cardiac tamponade may very occasionally be indicated in selected cases of penetrating chest trauma.35,36
High risk injury patterns
Restless and combative patients with head injury may also be extremely difficult to manage safely in-flight without resorting to sedation. This may further compromise the patient unless the airway has been definitively secured. These patients should be anaesthetised, intubated, and ventilated if transported by helicopter.14 The risk of vomiting is increased in the presence of a skull fracture, direct brain stem injury associated with raised intracranial pressure, and intracranial haematoma. Comatose head injured patients (AVPU score P or U, GCS <9) may also be unable to maintain and protect their airways and this is itself an indication for RSI and tracheal intubation.37 For these reasons, significant head injury as defined in figure 2 is a relative contraindication to helicopter transport without a definitive airway, irrespective of whether the airway is compromised or not. Again prehospital critical care reflects current best practice in hospital based guidelines for the interhospital transfer of patients directly to neurosurgical units12 in the UK.
Patients with facial fractures may have significant bleeding into the upper airway. This can be hazardous in patients who are secured supine, especially if there is an associated reduction in conscious level or loss of upper airway reflexes, or both, unless the airway has been definitively secured. Patients with significant head and facial injuries may also have important associated injuries to the neck and thoracolumbar spine, which will also need to be considered during initial management and transport.38
Patients with an inhalation airway burn should be transported to hospital as rapidly as possible. A definitive airway should ideally be secured as early as possible.38 In the absence of prehospital critical care as defined in figure 2 such patients should be transported as rapidly as possible to the nearest emergency department. Burnt patients with significant associated injuries must not be directly triaged to a burns unit unless it is co-located with an on site emergency department with direct access to the other required trauma surgical services.
Penetrating neck injury may result in rapid airway obstruction and this injury is a relative contraindication to helicopter transport without a prior definitive airway.20 This will necessitate RSI and tracheal intubation in salvageable patients.39 In the absence of prehospital critical care, such patients should be transported to the nearest hospital’s emergency department in the authors’ opinion as rapidly as possible to access the required level of care to prevent secondary (hypoxic) injury.
Spinal cord injury is not a contraindication to helicopter transport unless it is associated with airway obstruction, hypoventilation, shock, or significant head or facial injury (fig 1). In the absence of such complications, helicopter transport should be actively considered as the transport mode of choice as it may reduce the potential for secondary spinal injury by providing a smooth and timely transfer to an ED.
Accessibility of incident scene
Patients who sustain serious injury in inaccessible locations, or where a land ambulance is not immediately available, may need to be transported by air irrespective of their clinical state and on scene resources. If a patient’s condition deteriorates in flight, consideration should be given to landing the aircraft immediately and clinically reassessing the patient unless arrival at hospital is imminent. It may rarely be appropriate in certain circumstances to complete the journey by road.
Transfer times
It is necessary to establish the total transport time when air and road transport options are considered. It often takes at least 20 minutes to transfer a patient from scene to helicopter landing site, package, secure, lift, fly, unload, and transfer the patient from helipad to emergency department by air ambulance in metropolitan areas.6 There is consensus that helicopters have a role in transporting critically injured patients over distances greater than 50 kilometres or 30 minutes by road in rural areas in Australia.40,41 Helicopter transport time may be significantly longer than 20 minutes if there is a need for secondary land ambulance transfer from the hospital’s helipad to the emergency department.42 In our experience secondary land ambulance transfer from helipad to the ED may add up to 15 minutes to the total helicopter transport time. The necessity for land ambulance transfer from helipad to hospital may double transport times by air,6 and this may have important consequences for patients who cannot receive advanced airway management until arrival in the ED resuscitation room. Helicopter transport with secondary land ambulance transfer from the helipad is unlikely to be faster than direct transport from the scene by road unless the road transport time is estimated to be >45 minutes, and this is reflected in the algorithm.
This emphasises the necessity of having helipads located at trauma centres in close proximity (a trolley push) to the ED.46
In secondary air ambulance responses, it will be necessary to factor in air ambulance arrival times if not already on scene. It is clearly essential to establish all of this information at the scene before choosing the transport mode, and to carefully balance the risks (secondary injury) compared with the benefits (rapid transport) of helicopter transport, especially in major trauma cases without immediate access to critical care.
Which hospital?
It is also important to consider the local receiving hospital’s resources when considering triage and transport issues. Patients may potentially be delivered to either the nearest hospital’s emergency department or to the most “appropriate” hospital that can manage the patient’s entire injury pattern, often a specialist regional tertiary trauma referral centre in the UK. The UK currently has only six major emergency departments with on site general and orthopaedic surgery, neurosurgery, cardiothoracic, maxillofacial and plastic surgery.32 The average district general hospital in the UK serving a catchment area of 250 000 is unlikely to manage a patient with an injury severity score of greater than 15 more than once a week, and this has an important implication on local trauma team experience and patient outcomes.43 Many studies have confirmed improved outcomes by direct field triage to level 1 trauma hospitals in the United States.26 Rapid helicopter transport may improve patient access to specialist trauma centres if geographically remote from the scene of injury,6 and reduce the need for subsequent secondary interhospital transfer in both urban and rural areas.44,45 An integrated transport system supporting regional trauma centres would facilitate the development of networked National Trauma Service as advocated by the Royal Surgical Colleges in the United Kingdom.27,43,46
As mentioned above it is important to note that some hospitals offering regional surgical services (for example, neurosurgical or burns units) may not have an ED on site or direct access to other surgical teams. These units will clearly not be able to accept unstable multiply injured patients directly from an incident. If patients are triaged from the scene directly to an acute multi-disciplinary hospital, the need for a potentially lengthy interhospital secondary transfer and the demands on the “nearest” hospital will be avoided. Patients will be more likely to maximally benefit from timely specialist surgical treatment,46 for example, evacuation of an intracranial haematoma within four hours of injury, with improved outcome,20 and potentially shortened intensive care47 and hospital stays.47
Prehospital bypass
Depending on local ambulance service policy and circumstances in the UK, the decision to bypass the nearest hospital may only be made by an immediate care doctor, ambulance service officer, or attending paramedic, with local knowledge of neighbouring hospital resources. This may require considerable experience and clinical judgement in the context of severe injury. There are very few bypass policies published in the literature; most are area specific and are based on patient survey systems.48 The most common scoring systems incorporated into these bypass protocols in the past include the trauma score49 and revised trauma score.50 We have not identified any protocols that specify the level of care that should be delivered to enable prehospital bypass to be achieved as safely as possible. We have attempted to address this in this algorithm.
Prehospital critical care
For patients to benefit from timely definitive surgical care, it is essential that secondary neurological injury is avoided, and this may only be achievable in the prehospital phase in the presence of a trained clinician with experience of delivering prehospital critical care at the scene. Flight crew configurations and the range of prehospital critical care skills available vary in different prehospital care systems. There is conflicting evidence in the literature as to which incident type and what flight crew combination (for example, paramedic51 or nurse52 alone, paramedic- paramedic,53 paramedic-doctor,14,54–66 paramedic-nurse,34,58,67,68,70,71 nurse-doctor,52,58,69,72 and nurse-nurse67,68) are best suited to deliver this level of care in the field. A number of different outcomes (for example, patient mortality, critical care procedures undertaken, duration of stay in hospital/ITU) have been used in an attempt to assess this important issue, and all available studies have important limitations. There are very few published data on trauma patient morbidity outcomes, a potentially better marker for the assessment of the effectiveness of therapeutic interventions than mortality. The commonest flight crew configuration in the UK currently is paramedic-paramedic. Although UK flight paramedics do not currently have the skills for prehospital critical care as defined in figure 2, the proportion of their workload that involves managing serious injury (ISS >15) is very small,73 as compared with the paramedic-doctor configuration in London where clinical intervention currently beyond paramedic protocols are used in up 58% of cases attended.44
If prehospital critical care is not available, then physiologically compromised patients with adverse clinical signs and life threatening injury patterns should be transported to the nearest emergency department as rapidly and as safely as possible to access such care in the authors’ opinion. This may be most safely achieved by road transport for reasons alluded to above. Such patients, however, may be vulnerable for a considerable period of time before they reach hospital. Currently, in metropolitan areas in the UK, even using land ambulances operating a “scoop and run” policy, this is on average 45 minutes even in the non-trapped.74 In remote rural areas, if extrication at the scene has been required this may be much closer to two hours.75 Thus the “golden hour”76 that follows serious injury is essentially a prehospital event. Early deployment and timely delivery of hospital based medical teams or accredited immediate care doctors with critical care skills, either by road or helicopter, may improve patient outcomes in physical entrapment scenarios.
Patients with less serious injury patterns (fig 1), without adverse clinical signs or injury, can be transported by road or by air. For consistency we have used a transfer cut off time of 45 minutes by road to guide transport modality decisions. It is important, however, that air ambulances are appropriately tasked, manned, and resourced to deliver the highest standards of care to those patients with the greatest need, and that they should be stood down promptly when not required.
In the UK, the manning of air ambulances, and aircraft specification, varies throughout the country.5 London’s Helicopter Emergency Medical Service is currently the only air ambulance in the United Kingdom that is always manned by at least one doctor and paramedic with training in prehospital critical care that responds to primary trauma missions. Two other part time medically manned HEMS (paramedic-doctor) based in Warwickshire and Middlesbrough were launched in October 2003. All the other UK air ambulances are predominantly paramedic-paramedic manned.5 It is important, therefore, that those making transport decisions at the scene are aware of the clinical capabilities and limitations of the available helicopter and flight crew and consider alternative modes of transport and hospital destinations if necessary.
CONCLUSIONS
Decisions regarding the appropriate mode of transport to hospital for trauma patients are potentially complex and should be determined by the environment and circumstances of injury, the clinical state of the patient, the incident location’s accessibility, the clinical resources at the scene, and the proximity and resources of adjacent hospitals. Critically injured patients, who potentially have the most to gain by rapid transport to definitive care, may not be well served by air transfer where the risk of sustaining secondary injury is increased. In the current UK emergency service infrastructure most air ambulances do not have the crews to provide the necessary critical care clinical interventions to ensure the safe transport of severely injured patients. This level of care is however being increasingly delivered by voluntary, part time, land based critical care schemes at the request of the ambulance service in England.77–79 Although this algorithm may not appear to reflect most current UK air ambulance practice, many other aero medical services in other European countries,62,63,66,72 Australasia,64,65 and North America52,54,58–60,67,68,72 do provide crews with the necessary critical care skills. The evidence for the clinical benefit and cost effectiveness of UK helicopter emergency ambulance services is becoming increasingly strong.5 We hope that our transport algorithm will be a useful guide to those who may be faced with making finely balanced decisions that may have an important impact on patient outcome.
Acknowledgments
The authors would also like to acknowledge the extremely helpful comments of Dr Roderick Mackenzie in reviewing the initial draft of the manuscript. We would like to thank Ms Helen Carter, Clinical Librarian, Health Care Libraries, University of Oxford, for assistance with literature searching, and Oxford Medical Illustration Depart-ment (OMI), John Radcliffe Hospital, for the helicopter transport algorithm art work.
REFERENCES
Supplementary materials
Figure 1 in Colour
The colour figure is available as a downloadable PDF (printer friendly file).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
Footnotes
-
Funding: none.
-
Conflicts of interest: none declared.
Linked Articles
- Primary Survey