Article Text

Abstract
Objective: Access block refers to the situation where patients in the emergency department (ED) requiring inpatient care are unable to gain access to appropriate hospital beds within a reasonable time frame. We systematically evaluated the relationship between access block, ED overcrowding, ambulance diversion, and ED activity.
Methods: This was a retrospective analysis of data from the Emergency Department Information System for the three major central metropolitan EDs in Perth, Western Australia, for the calendar years 2001–2. Bivariate analyses were performed in order to study the relationship between a range of emergency department workload variables, including access block (>8 hour total ED stay for admitted patients), ambulance diversion, ED overcrowding, and ED waiting times.
Results: We studied 259 580 ED attendances. Total diversion hours increased 74% from 3.39 hours/day in 2001 to 5.90 hours/day in 2002. ED overcrowding (r = 0.96; 95% confidence interval (CI) 0.91 to 0.98), ambulance diversion (r = 0.75; 95% CI 0.49 to 0.88), and ED waiting times for care (r = 0.83; 95% CI 0.65 to 0.93) were strongly correlated with high levels of ED occupancy by access blocked patients. Total attendances, admissions, discharges, and low acuity patient attendances were not associated with ambulance diversion.
Conclusion: Reducing access block should be the highest priority in allocating resources to reduce ED overcrowding. This would result in reduced overcrowding, reduced ambulance diversion, and improved ED waiting times. Improving hospital inpatient flow, which would directly reduce access block, is most likely to achieve this.
- ED, emergency department
- EDIS, Emergency Department Information System
- TOPAS, the Open Patient Administration System
- Access block
- Ambulance diversion
- Emergency Department overcrowding
- Waiting times
Statistics from Altmetric.com
- ED, emergency department
- EDIS, Emergency Department Information System
- TOPAS, the Open Patient Administration System
Providing acutely ill patients with rapid access to emergency care is the prime role of emergency medicine. Access block refers to the situation where patients in the emergency department (ED) requiring inpatient care are unable to gain access to appropriate hospital beds within a reasonable time frame, 1 resulting in ED overcrowding and ambulance diversion.
Overcrowding in the ED has been described as “the most serious issue confronting EDs in the developed world”.2 Overcrowding refers to the situation where ED function is impeded, primarily because the number of patients waiting to be seen, undergoing assessment and treatment, or waiting for departure, exceeds the physical or staffing capacity of the ED.1
The effects of overcrowding have been previously reported, and include ambulance diversion, impaired access to emergency care, compromised clinical care, prolonged pain and suffering, and prolonged inpatient length of stay, and has been linked to fatalities.2–7 Ambulance diversion was rare in Perth for most of the 1990s but is now a daily event.
All publicly administered emergency departments in metropolitan Perth use the Emergency Department Information System (EDIS), with continuous electronic capture of ED patient transit through the ED. As the most isolated capital city in the world, there is virtually no leakage of ED patients from Perth to other cities. The combination of excellent information and geographical isolation present a unique opportunity to systematically evaluate the possible causes of metropolitan ED overcrowding and ambulance diversion.
METHODS
Perth’s population of 1.4 million is served by public EDs at four large central metropolitan hospitals (one exclusively paediatric), three smaller outer metropolitan hospitals, and two privately administered public hospitals. In addition, there is one private hospital ED. The capacity of the metropolitan public hospital system to accept ambulances is largely dependent upon the ability of the three main central tertiary hospitals to receive the majority of the ambulance presentations (this was 82% during the study period).
A retrospective analysis of data from EDIS and the Open Patient Administration System (TOPAS) for calendar years 2001 and 2002 was undertaken. EDIS (version 9) is software provide by Hospital Administration Software Solutions and is used in the public metropolitan EDs in Perth. TOPAS is the inpatient administration system used in all public metropolitan hospitals in Perth.
Bivariate and multivariate analyses were performed to illustrate the relationship between a range of variables likely to be correlated with ED overcrowding, access to emergency care, and ambulance diversion at the three main central tertiary hospitals (Fremantle Hospital, Royal Perth Hospital, and Sir Charles Gairdner Hospital). Each episode of ambulance diversion was recorded on a spreadsheet by the ambulance service at the time it occurred. Table 1 lists the definitions of the variables used for analysis. Analysis was conducted using SPSS (version 11.5; SPSS Inc, Chicago, IL, USA).
Definitions of terms and variables examined
RESULTS
Total ED attendances to the three tertiary hospitals remained stable between 2001 (129 011) and 2002 (130 569). Total admissions (mean 42%) increased slightly, from 54 678 in 2001 to 55 481 in 2002.
Total ambulance diversion hours increased 74% from 3.39 hours/day in 2001 to 5.90 hours/day in 2002 (fig 1). Triple diversion requests (when all three hospitals request ambulance diversion) grew from virtually non-existent in the first half of 2001 to every third day in 2002.

Total ambulance diversion time and triple diversion requests.
Total ED occupancy, an index of emergency department overcrowding, was shown to have an almost linear correlation with access block ED occupancy (r = 0.96, 95% CI 0.91 to 0.98, p<0.001; table 2). There was also a significant correlation with admissions and sea surface temperature. Given the dependency of total ED occupancy upon access block ED occupancy, access block ED occupancy was used in preference to total ED occupancy to assess the relationship between ED occupancy, ambulance diversion, and waiting time compliance.
Correlations with total emergency department occupancy, ambulance diversion, and proportion of patients not seen within threshold waiting times
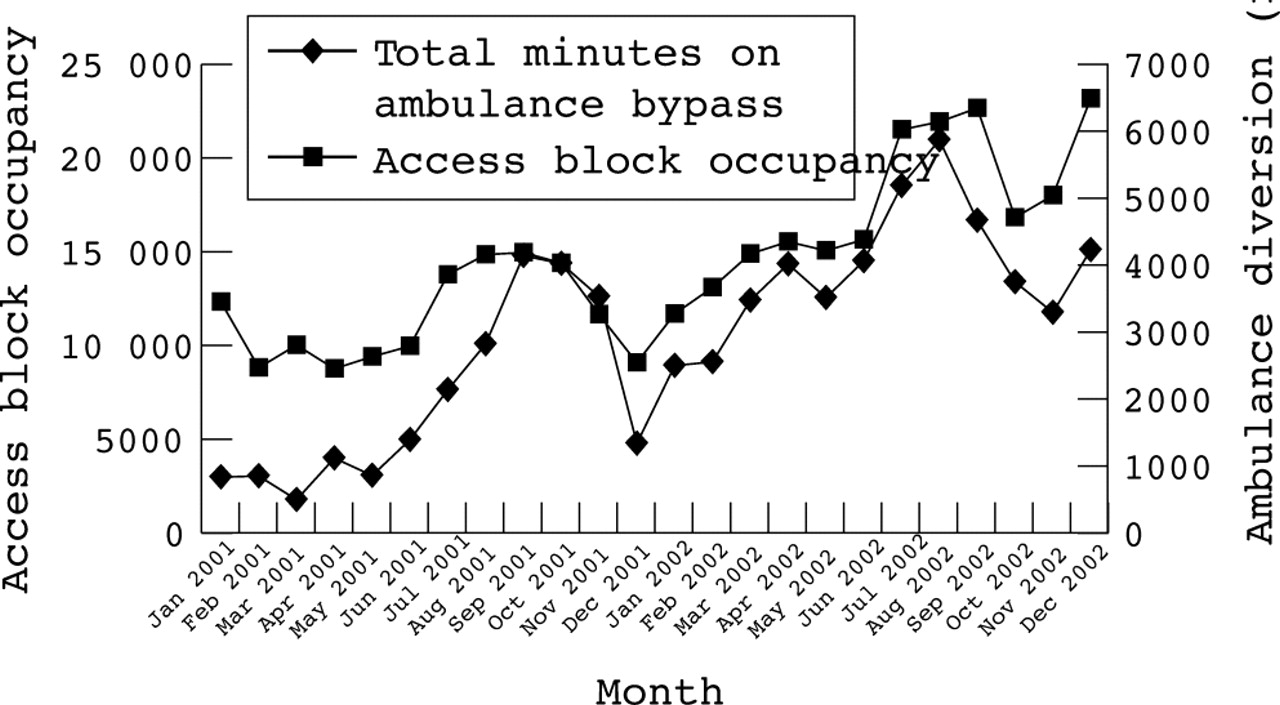
Bivariate analysis indicated that access block ED occupancy has a strong positive correlation with ambulance diversion (r = 0.75, 95% CI 0.49 to 0.88, p<0.001; table 2). Fig 2 illustrates the correlation between the rise in access block ED occupancy and the total number of ambulance diversion hours between 2001 and 2002. Between 2001 and 2002, the proportion of access blocked patients increased from 11% to 16% (45% increase, p<0.001). Sea surface temperature was also shown to have a correlation with ambulance diversion. Total attendances, low acuity patient attendances, discharges, and admissions were not correlated with ambulance diversion (table 2).

Relationship between access blocked patient occupancy and ambulance diversion.
Compliance with recommended waiting time thresholds for care deteriorated from 65% in January 2001 to 50% in December 2002 (15% decrease, p<0.001; fig 3). Access block ED occupancy was highly correlated with deterioration in compliance with waiting time thresholds (r = 0.83, 95% CI 0.65 to 0.93, p⩽0.001; table 4). Admissions and total attendances were also shown to have a correlation with waiting time compliance. Sea surface temperature may be weakly correlated with waiting time compliance; however, low acuity patient attendances and discharges were not correlated with waiting time compliance.

{kind=link}
{kind=link}
{kind=link}
Correlation between access block cubicle occupancy and compliance with waiting time thresholds. ATS 4 patients comprise approximately 40% of total patient attendances. They are categorised as semi-urgent and should be seen by a doctor within 1 hour. Generally, they are ambulant and many are able to wait in waiting rooms. Their admission rate is 20–30% and their waiting times are greatly affected by lack of ED cubicle availability. Ab cub occupancy, access blocked cubicle occupancy.
The use of stepwise regression to develop models for total ED occupancy, ambulance diversion, or waiting time compliance failed to identify a model including any additional variable independent of access block ED occupancy. All other variables tested in the model are those stated in table 2.
DISCUSSION
Our study clearly demonstrates that ambulance diversion and poor ED performance are related to poor inpatient flow. This manifests as the presence of admitted patients in the ED—that is, access block. Despite little change in ED attendances during the study period, we have demonstrated an almost linear relationship between access block ED occupancy and total ED occupancy. Similarly, there was a strong relationship between access block ED occupancy and both ambulance diversion and prolonged ED waiting times.
A winter–spring exacerbation of access block ED occupancy associated with increased ED admissions was identified; however, our attempts at stepwise regression indicated that access block ED occupancy may be used as a single variable to predict the risk of ED overcrowding, ambulance diversion, and prolonged ED waiting times in metropolitan Perth central EDs, regardless of time of year or ED admissions.
Our results concur with other international reports that have found that the presence of inpatients in the ED is the primary reason for ED overcrowding. Schull also found that admitted patients contribute disproportionately to ambulance diversion.8 Ambulance diversion has gradually become standard operating procedure in many cities.9 Trzeciak also reports that the main cause of ED overcrowding is inadequate inpatient capacity.10 Thus, this capacity crisis is now an important public health issue.10–12 Furthermore, patients who experience access block have a longer length of inpatient stay, thus exacerbating the problem,4,13 and this impairs access to emergency care.
A frequent response to this issue in the media is that it is the low acuity patients who are the cause of overcrowding. However, we have found that these "walk-in" patients do not cause overcrowding or ambulance diversion. This is also consistent with the international literature.8 One cubicle blocked by an admitted patient for 8 hours impairs the assessment of 24 low acuity patients (assuming 20 minute assessment times). Removing this admitted patient would improve patient flow within the ED. It is also noteworthy that we found a predictable seasonal increase in the admitted patient burden for hospitals, which should be considered in health planning policy.
It is interesting to note that compliance with waiting times was improving in 2001 against a stable background of access blocked patients, suggesting that EDs were striving to improve performance. However, in 2002 these efficiencies were lost because of the overwhelming effects of access block.
To improve ED performance and decrease ambulance diversion, steps need to be taken to improve patient flow and thereby reduce access block. Possible methods to achieve this include:14,15
-
Increasing the availability of acute care beds
-
Better home care, and urgent nursing home placement of the elderly
-
Better organised and active discharge planning
-
Speedier assessments in the ED, for example, improved turnaround times for laboratories, radiology, and consultants
-
Speedier transfer to wards if admitted
-
Better management of chronic disease in the community to avoid ED attendance
-
Prevention of illness leading to ED attendance.
Prevention strategies are frequently forgotten, such as fall prevention in the elderly. The elderly tend to be complex patients who are potentially long stay inpatients. Conversely, decreasing low acuity patient attendances will have minimal impact on decreasing ambulance diversion and ED overcrowding.
Other solutions include improvements to hospital flow of rehabilitation patients. For example, reducing the length of stay of one rehabilitation patient from 30 days to 15 days creates as many bed days as reducing the length of stay of 30 acute patients by half a day.
There are limitations to our study. We used data summed for whole months, whereas there is variability in the severity of ED overcrowding hour to hour. Other factors may have influenced ambulance diversion, such as the availability of staff in the ED; however, at least one study has shown this to be not significant.8 In addition, we have identified important overall trends, which could assist with strategies for a whole of system approach.
A second possible limitation is that the emergency physicians at each site used different criteria for ambulance diversion. It is possible that their approach may not have been consistent over the study period. However, the staffing was stable, and a large number of episodes of ambulance diversion were studied, hence, we believe that any effect of this was minimal.
Another limitation is that we did not include the impact of the outer metropolitan EDs. However, they represent only 18% of total ambulance presentations and have a different casemix to the major teaching hospitals we studied. In addition, this paper focuses on overcrowding, but other strategies may be useful to address waiting times.
In conclusion, we found that in Perth, reducing access block should be the highest priority in allocating resources to reduce ED overcrowding. This would result in reduced ambulance diversion and improved ED performance. Improving hospital inpatient flow is most likely to achieve this. These results are consistent with other studies.
REFERENCES
Footnotes
-
Competing interests: none declared
Linked Articles
- Correction