Article Text

Abstract
The Cape Triage Group (CTG) convened with the intention of producing a triage system for the Western Cape, and eventually South Africa. The group includes in-hospital and prehospital staff from varied backgrounds. The CTG triage protocol is termed the Cape Triage Score (CTG), and has been developed by a multi-disciplinary panel, through best available evidence and expert opinion. The CTS has been validated in several studies, and was launched across the Western Cape on 1 January 2006.
The CTG would value feedback from readers of this journal, as part of the ongoing monitoring and evaluation process.
- Prehospital
- triage
Statistics from Altmetric.com
INTRODUCTION
The health burden on emergency services in South Africa is enormous – an estimated 60 000 South Africans die of road traffic accidents and homicides each year.1 At least 2.5 million cases of non-fatal injuries require emergency care annually – this translates to about 66 trauma presentations per 1000 population per annum,2 way ahead of trauma levels in other countries. This trauma load is added to the huge burden of illness, with HIV/AIDS and Tuberculosis rife through many parts of the population.
There exists a need to properly prioritise the care of these patients, in both the prehospital and emergency unit setting. Such prioritisation is termed triage – the process of sieving or sorting patients according to need. Many triage tools exist for use in both prehospital and the emergency unit, however, such algorithms have problems preventing their adaptation in the South African setting.
In-hospital triage systems include Manchester Triage,3 the Canadian Triage Assessment Scale (CTAS),4 and the Australian Triage Score (ATS):5 each of these triage tools require extensive training to implement, making their widespread adoption in South Africa problematic. Furthermore, the time taken to triage each patient is too long for most emergency units in the South African setting, where the case-load presenting to many of our emergency units is so large that a rapid system is required.
Prehospital tools are typically generalisable to many different countries, however, they lack the sensitivity and specificity to make them safe for emergency unit use. Furthermore, some are validated only for trauma triage,6–8 whilst others are too detailed to be of roadside use.3–5
The Cape Triage Group (CTG) was convened in Cape Town in 2004 to produce a triage system suitable for local use. The CTG falls under the auspices of the Joint Division of Emergency Medicine of the University of Cape Town (UCT) and University of Stellenbosch. The group is multidisciplinary and comprises doctors, sisters, and paramedics from the state and private sectors, ensuring expertise in all aspects of emergency care from prehospital through to admission from the emergency unit.
The intention of the CTG was to develop a system of triage for use in the Cape.
CURRENT TRIAGE SYSTEMS IN SOUTH AFRICA
A. Prehospital
The prehospital use of triage in South Africa varies from region to region, but is generally categorised into four priorities (represented by colours). The systems in use at selected South African ambulance training colleges are presented in table 1.
Current EMS triage criteria as instructed at colleges throughout South Africa
Such triage typically uses instability of vital signs to differentiate high from low priority patients, following the recommendations of MacMahon.9 Discrepancies in triage appear when personnel of differing levels of medical experience and qualifications classify patients, as there are no clear definitions of ‘unstable’ physiology. Without objective clinical parameters, such variations in patient assessment are inevitable. To complicate matters further, classifications such as ‘stable red’ or ‘unstable yellow’ patients confuse the true severity of the patient’s clinical profile. The terms ‘stable’ and ‘unstable’ are poorly understood and fail to accurately reflect the patient’s clinical condition.
Triage must be rapid to undertake whilst being easy to use. The current system of triage fulfils both these criteria but lacks sensitivity and specificity (as well as consistency).
B. Emergency Unit
Public sector emergency units are under enormous pressure with large patient numbers, high case severity, understaffing and poor resources. GF Jooste hospital is a typical example, seeing over 4500 patients per month in the emergency unit but staffed to see around half of this number. This unit deals with the current top four epidemics in South Africa in equal proportions: HIV/AIDS, non-HIV related infectious diseases (tuberculosis), traumatic injuries, and diseases of lifestyle (hypertension, diabetes, etc.).10 Roughly 35% of these cases require immediate to urgent attention, whilst only 25% are considered non-urgent.11 This leads to long waiting times and, more importantly, poor management of clinical risk. These pressures are not unique to the state sector, with some of the busier private units seeing more patients of higher severity than they are resourced to deal with. Private units (such as Milnerton Mediclinic) see over 2000 patients per month, including polytrauma and medical emergencies, with insufficient staffing to avoid the need for triage. However, no formal triage systems are in place, relying rather on the “eyeball” assessment of a nurse.
In order to maximise efficiency of the use of resources, and to minimise risk to the patient, an effective triage system with high sensitivity and specificity is required.
METHODS
The CTG endeavoured to design and test a simple, effective triage tool. This instrument had to fulfil the requirements of being easy to use by all levels of prehospital providers, nursing staff and doctors - from the roadside through to the EU. A universally accepted and utilised objective triage system would avoid discrepancies in patient classification. Thus, for example, ‘red’ would mean ‘red’, and ‘yellow’ would mean ‘yellow’ to all, despite different levels of experience and qualifications. The CTG reviewed existing triage instruments and developed a new combined CTG triage system and scoring sheet. Each of the following factors was considered in developing the system:
-
Physiological derangement
-
Discriminators
Mechanism of injury
Symptom complexes
Discriminators
Senior Health-Care Personnel’s Opinion
-
Nomenclature
Physiological derangement
Triage is dynamic: a patient’s status can change at any time and so their triage category may also change. This important ability to change priority12,13 is exclusive to physiological assessment. It was felt essential that the triage system contains physiological assessment. The Revised Trauma Score, based on Glasgow Coma Score (GCS), Systolic Blood Pressure and Respiratory Rate, has been successfully used to identify seriously injured trauma cases presenting to an emergency unit (systolic hypotension was found to be a particularly useful sign of serious injury).14 However, this score may not include sufficient clinical parameters to differentiate between medical cases. Previous research has focussed on developing criteria for identifying medical in-patients at risk of deterioration. Acute dyspnoea has been found to be particularly useful as a physiological marker of imminent arrest.15,16 The Medical Early Warning Score (MEWS) uses physiological parameters such as systolic blood pressure, heart rate, temperature, respiratory rate and AVPU level of consciousness. MEWS has been used to successfully identify physiological deterioration of medical in-patients17 – in this study, MEWS scores of five or more were associated with increased risk of death, ICU and High Dependency Unit admission (approximately 25% combined outcome). The MEWS score is a ‘simple, practical method of using routine physiological measurements to flag, from among the mass of admissions, patients who should not be ignored’.18
In 1997 the Audit Commission in the UK considered the issue of critical care outreach services to medical wards to consult on medical in-patients who were deteriorating. This led to the development of Intensive Care Outreach Services (ICORS) whereby intensive care consultation in medical wards was identified prior to the need for ICU admission. Summarising abnormal physiology into the MEWS score was found to be a particularly useful tool in this process.18 Using the MEWS as an ICORS referral tool led to decreased admission rate to ICU and shorter length of stay.19
A triage system that incorporated the MEWS score had been implemented at GF Jooste hospital in March 2004 and its substantial success initially alerted the CTG to the possibility of its use as a triage tool. The EU saw a considerable improvement in patient flow, and a significant reduction in mortality. However, the MEWS score is flawed with respect to triage in that it has a medical bias. Trauma patients (who are generally previously healthy and therefore have more physiological reserve) may have severe injuries and yet have a low MEWS score if they have stable physiology. The addition of both a mobility parameter and trauma factor were felt necessary to increase the severity score for trauma cases. This modified MEWS score was renamed the Triage Early Warning Score (TEWS). The TEWS scoring system has the following advantages:
-
It requires a comprehensive assessment of the ill patient early on.
-
It translates parameters that can be easily measured in both the prehospital and emergency unit setting, by even the basic trained levels of staff, to an equally easy and interpretable triage score.
-
It encompasses both trauma and medical patients, in both the prehospital and emergency unit setting.
-
By using this system, health care providers will be able to classify patients similarly, allowing for transparency of communication between medical staff and with more appropriate transfer of patients.
Despite the in-hospital success of the MEWS, it has not been formally validated as a triage tool. The TEWS score has been validated as part of a Masters degree,20 in addition to another Masters dissertation21 and a PhD thesis,22 involving the prospective assessment of almost 25,000 patients in both the public and private settings. A pre-hospital study will commence in 2006.
Discriminators
a. Mechanism of Injury
Mechanism of injury scores have been shown to be highly sensitive at identifying casualties with severe trauma. However, they have also been shown to have high rates of overtriage.23 Mechanism of injury was included but limited to high energy transfer.
b. Presentations
Triage systems often use presentations as core elements: examples of these include level of consciousness, haemorrhage and pain. We deliberately avoided long lists that would lead to long algorithms or a bulky triage tool. Although there are some specific diagnoses in the triage algorithm (e.g. burn – face/inhalation), most are presentation types such as chest pain.
c. Pain
Pain is an important part of the assessment of patients in the EU. The CTS includes an assessment of pain as part of the triage decision making process.
d. Senior health-care personnel’s opinion
There is evidence that experienced health care professional can improve the triage process by adding their opinion to other parameters.22 However, this is experienced based and it would not be appropriate for more junior staff to triage by this “gut feel”. In the CTG protocol, the senior health care provider involved with the patient may alter the triage coding.
Nomenclature
The CTG considered whether a colour-coded or ‘Priority’ (e.g. P1–P4) nomenclature was more practical. Due to the fact that colours are more readily identifiable to both medical staff and patients (considering practical points such as colour-coded stickers on folders and even coloured zones in emergency units) it was felt that a colour-based system was preferential.
Many triage systems use a 5-tiered approach (UK, Canada, Australia). Due to the problems of the ‘stable red’ and the ‘unstable yellow’ patients, a fifth category, orange, has been introduced into the South African system. The triage categories chosen by the CTG are:
-
Red - resuscitation/physiologically unstable patients
-
Orange - serious cases with potentially unstable physiology or potentially life/limb threatening pathology
-
Yellow - ‘physiologically stable’ cases with reasonably serious medical or trauma problems
-
Green - minor injuries/illness
-
Blue - those who are clearly dead
Most of the cases referred to an emergency unit fall into the orange or yellow category (44% of all attendees at GF Jooste11). The orange category essentially reduces the number of patients in the very large yellow category (38% in the previous four colour system at GF Jooste) whilst limiting the red category (26% in previous system at GF Jooste) to resuscitation or acutely unstable cases.
RESULTS
The final CTS is a 5-colour coding system comprising the following:
-
TEWS score
-
Discriminators
Mechanism of injury
Presentation
Pain
Senior health care professional’s discretion
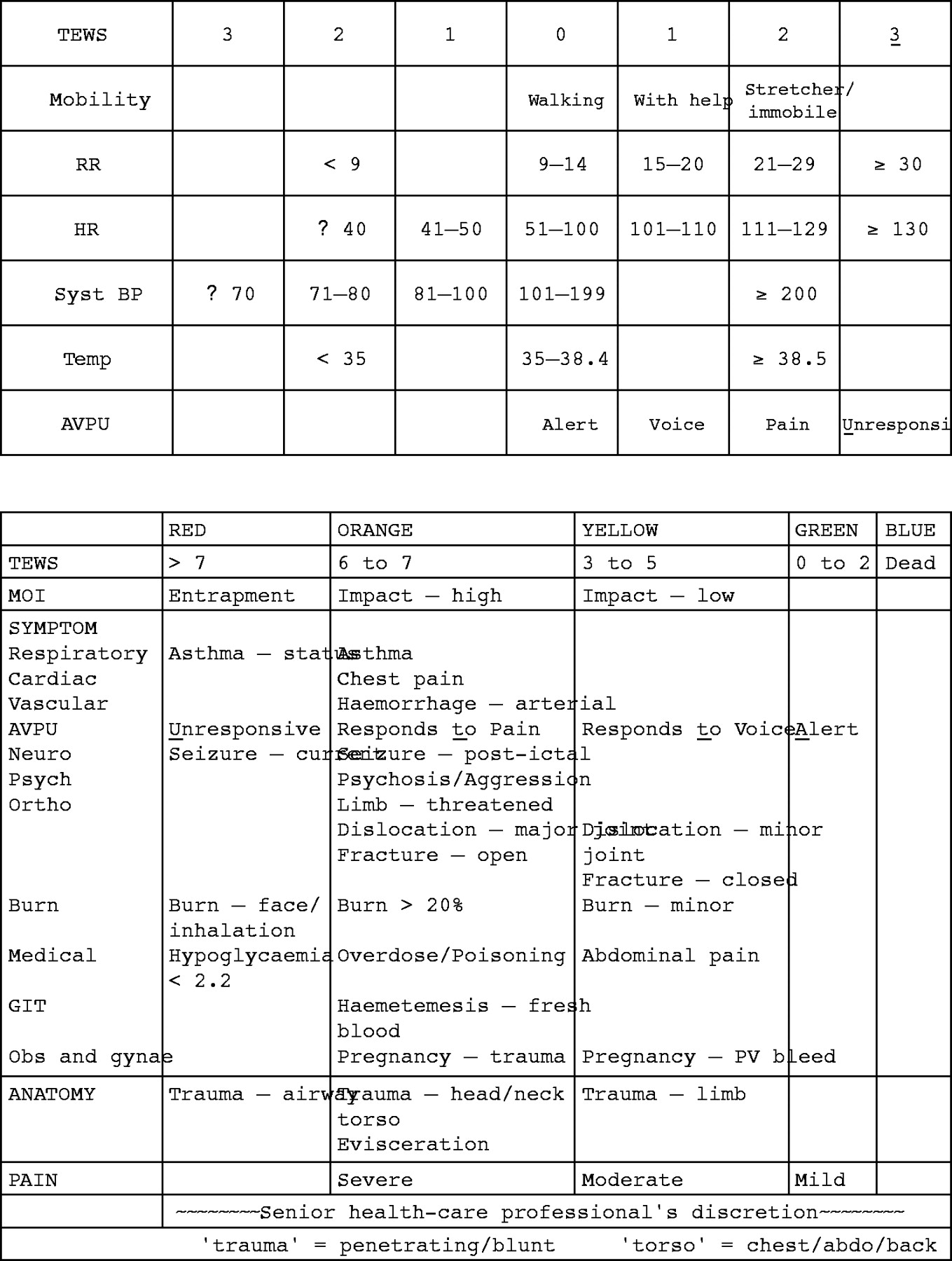
The CTS is printed on posters and credit card sized keycards, which can then be used by medical personnel from the roadside through the EU (figure 1). Poster sized versions will be available in EUs to facilitate triage.
{kind=link}
Cape Triage Group Triage System
There are three versions: adult, child, and infant. The adult version is intended for patients aged over 12 years, or taller than 150 cm. The infant version is for children under three years, or less than 95 cm, and the child version is for other children (three to 12 years, 95 to 150 cm). The adult version is shown below, and the child and infant versions are available on the web.
Use of the CTS
The use of the TEWS score encourages the healthcare professional undertaking the triage to actually measure physiological parameters, a step that is worthwhile not only for the purposes of triage. This is the first step in the triage process, with the recorded physiological values being awarded a score from the TEWS sheet: these are totalled and the resulting value is read off from the first line of the triage coding chart.
It is important to emphasise that it is not necessary to “tick all the boxes” for triage of individual patients – if a patient’s TEWS score make them orange then they are orange, unless there is an obvious other problem that would make them red. A current seizure, for example, will triage the patient red regardless of his TEWS score.
DISCUSSION
The CTS was rolled out across the Western Cape on 1 January 2006, following an extensive training programme. The CTS is fully supported by the provincial Department of Health. Experience at GF Jooste21 suggests that even inexperienced staff can learn the triage system following only a brief teaching period. It is accepted that there will be a “bedding in”period as staff become familiar with the system. There will be ongoing evaluation and assessment of the CTS, which will determine any modifications that need to be made to the system.
A request has been made to form a national Triage Group from 2006, with a view to taking the CTS nationwide.
Clearly the CTS is not intended for mass casualty situations: it is standard practice to use a simple triage method for a mass casualties situations and a more complex protocol on a day-to-day basis. Such mass casualties systems must be easy to learn and to use, fast to undertake and accurate.25 Examples of such systems include the Triage Sieve25 (used throughout the UK, Netherlands, Sweden, parts of India and Australia, and NATO military organisations), Careflighf26 (Australia) and START27 (USA).
While South African EMS providers are likely to be involved in mass-casualty situations on a more frequent basis than most ambulance services (around 10 such calls per week in the Cape Town Metropole), such events are still comparatively rare: around 0.1–0.2% of Metro Western Cape’s workload (personal communication, Dr W Smith Metro EMS, 2005). A two-triage system approach for South Africa is still entirely appropriate, although a mass casualty system does not yet exist in the Western Cape (where the same protocol is used as is used for single patients). It is not part of the remit of the CTG to develop a mass casualty triage tool.
CONCLUSION
There is a clear need for a simple yet robust triage instrument for use in the South African medical arena. All role players, from prehospital to the emergency units, must use whatever system is implemented. The “buy in” of all key role players is therefore essential.
As with any tool, the development of this new triage instrument is a dynamic process. Whilst the science behind the CTS has been demonstrated in several studies, the CTS is a living tool and must be monitored and evaluated. If changes are necessary, they will be made. As part of the ongoing evaluation, we wish to receive the input or as varied an audience as is possible in order to ensure that CTS evolves as a propery structured triage scheme. We value feedback from the readers of this journal (positive or otherwise) – either through the journal or direct to the authors.
CONTRIBUTION
All authors contributed equally to the article, on behalf of the Cape Triage Group. Dr L Wallis is the guarantor of this paper.
REFERENCES
Footnotes
-
Funding: none
-
Competing interests: none declared