Article Text

Abstract
Background: Until recently South Africa had no triage system for emergency department (ED) use. The Cape triage group developed a triage scale called the Cape triage score (CTS). This system consists of a basic physiology score, mobility score and a short list of important discriminators that cannot be accurately triaged on a physiological score alone. Highest priority is given to a red colour code, followed by orange, yellow and green.
Aim: The purpose was to evaluate the components of the CTS and identify amendments that would improve the quality of the scale in terms of its accuracy to identify patients more likely to require admission or at high risk of death in the ED.
Methods: Data were prospectively collected over a 4-month period. Data captured included the parameters of a basic physiological score (respiratory rate, pulse rate, systolic blood pressure, temperature and a simplified score measuring level of consciousness), mobility, a list of selected clinical conditions (discriminator list), final clinical diagnosis and final outcome in the ED (admission to hospital or death).
Results: 798 patients were triaged and analyzed. The CTS undertriaged 24% (overtriage 25%) of cases who required admission. By altering the colour code parameters, amending the discriminator list as well as the addition of a trauma factor, undertriage was reduced to 12% (with an overtriage of 45%).
Conclusions: The amended CTS has an acceptably low undertriage rate and is capable of predicting patient disposal over a wide spectrum of ED presentations.
Statistics from Altmetric.com
There are currently approximately 45 million people in South Africa, with an average life expectancy of 52 years.1 The health needs of the majority (84%) are served by an under-resourced public health service with an annual health budget just 23% that of private health expenditure.2 Central to the health crisis lies the country’s so-called quadruple burden of disease, responsible for premature mortality and emergency department (ED) overcrowding. Using global burden of disease indicators, the contribution to years-of-life-lost in South Africa is divided as follows:1 3 group I (communicable diseases, eg, tuberculosis), 25%; group II (non-communicable disease, eg, hypertension, diabetes mellitus), 21%; group III (injuries), 16%; HIV/AIDS (technically group I, but calculated separately for South Africa), 38%.
As in most developing countries, triage in South African ED has been non-existent until recently. Even though ED triage scales have been widely researched in developed countries, such triage scales may in fact not be valid in a developing country setting.4 Poor record keeping, lack of resources, different disease profiles and skill mix all have significant effects on presentation, treatment and outcome.4 The Cape triage score (CTS) was therefore designed as a new triage scale for local use.5
Using a three-stage stepwise approach, Subbe’s modified early warning score (MEWS) lies at the basis of the scale as step one (table 1).5–7 The designers concurred with Cooper et al8 that triage without physiological measurements may inadequately reflect patient urgency. The inclusion of physiology also follows a developing world triage scale design trend.4 Furthermore, the MEWS has been shown to identify medical inpatients at risk of deterioration and death accurately and its use is increasingly advocated.9–13 Step two involves the addition of a basic score of mobility (0, independently mobile; 1, mobile with assistance; 2, requires stretcher). The MEWS with the mobility score is also called the triage early warning score (TEWS). Finally, step three utilises a list of recognisable signs, called triage discriminators (table 2). The discriminator list allows appropriate triage by acting as a safety net in cases that do not necessarily present with abnormal physiology (eg, trauma). This is an important consideration as the MEWS on its own would not be robust enough.14 15 The triage category is reflected by a colour code indicating the urgency of care required. A senior healthcare professional is able to override this when applicable. We have previously described the CTS.5
The objective of this study was to evaluate the use of the CTS as a suitable scale for prioritising the delivery of emergency care to patients presenting to an urban public hospital ED. To do this, we evaluated the three components of the CTS: the MEWS as an appropriate physiological scoring system; the mobility score; the discriminator list as part of the CTS.
In addition, we sought to identify amendments to the CTS that would further enhance its quality.
This study was undertaken before the launch of the final version of the CTS; it constituted a key part of the development of that scale.
METHODS
Setting
The setting for the study was the GF Jooste Hospital, a 200-bed acute hospital situated in Cape Town that serves approximately 1.3 million people. The ED consists of a 50-seat reception area, 14 beds, four resuscitation bays and a patient holding area used for patients awaiting either admission, review or discharge (another 14 beds and 20 seats). The ED deals with almost 4500 consultations per month, with approximately 13% of patients requiring formal admission.
The serviced area has a higher than average burden (years-of-life-lost) as a result of group II (non-communicable diseases, 36%) and group III (injuries, 22%) compared with the rest of South Africa, and carries a significant burden of group I (communicable diseases, 20%) and HIV/AIDS (22%).16 17 With approximately 41% of the labour force unemployed, 51% of households living in informal dwellings and 44% of inhabitants living under the poverty line, it is also the poorest community in Cape Town.17 18
Study design
Data were prospectively collected over a 4-month period from 1 December 2004 to 31 March 2005. The resulting database was used to evaluate the CTS and simulate the effect of the identified amendments.
Selection of subjects
Patients were eligible for inclusion if they were 12 years or older and all fields were completed on the data capture sheet. Data capture was performed on weekdays between 08:00 and 17:00 hours. Data were captured separately to blind the triage doctor to patient outcome.
Triage process
A triage station was set up in the patient reception area. Figure 1 shows the strategy employed for data collection. A data sheet captured the MEWS parameters, mobility of the patient, any option selected from the discriminator list and the priority colour code assigned by the triage doctor (SRB). Additional data included the final ED diagnosis and outcome of the ED visit.

Outcomes
Primary endpoints were admission from and death in the ED. The hypothesis was that colour code red and orange patients indicated a higher risk of admission or death (endpoint reached) and that colour code green patients indicated likely discharge from the ED (endpoint not reached). Overtriage and undertriage were calculated to prove the hypothesis. Overtriage assumed that an endpoint was indicated by the scale (colour code red or orange) but not reached (discharge from ED) and undertriage that an endpoint (admission or death) that was not indicated by the scale (colour code green) was in fact reached. In keeping with the American College of Surgeons Committee on Trauma (ACSCOT) guideline, threshold indicators for overtriage would be acceptable up to 50% and 10% for undertriage.19
Data analysis
Data were entered into a Microsoft Access database. Mean, median, range, standard deviation and 95% CI were calculated using Statistica version 7 software. The χ2 test was used to compare categorical data. A p value of 0.05 or less was regarded as statistically significant.
RESULTS
Demographic data
Of the 1000 patients entered into the trial, 798 (80%) had complete datasets used for analysis. The mean (SD, 95% CI) age of the study cohort was 39 years (15, 37.9 to 40.1). Of 798 patients, 59% were women; 56% of consultations were medical, 32% surgical, 8% trauma and 4% were psychiatric.
Outcomes
A total of 330 (40.1%) patients included in the study reached an endpoint. Of these, 327 patients required admission and three patients died. As a result of this small number of deaths, these cases were not included further in evaluations or the endpoint definition.
Evaluation of the CTS
Red, orange, yellow and green colour codes were assigned to 6.5%, 20.6%, 50.3% and 22.6% of patients, respectively. The CTS components were evaluated individually as follows.
Step 1: MEWS
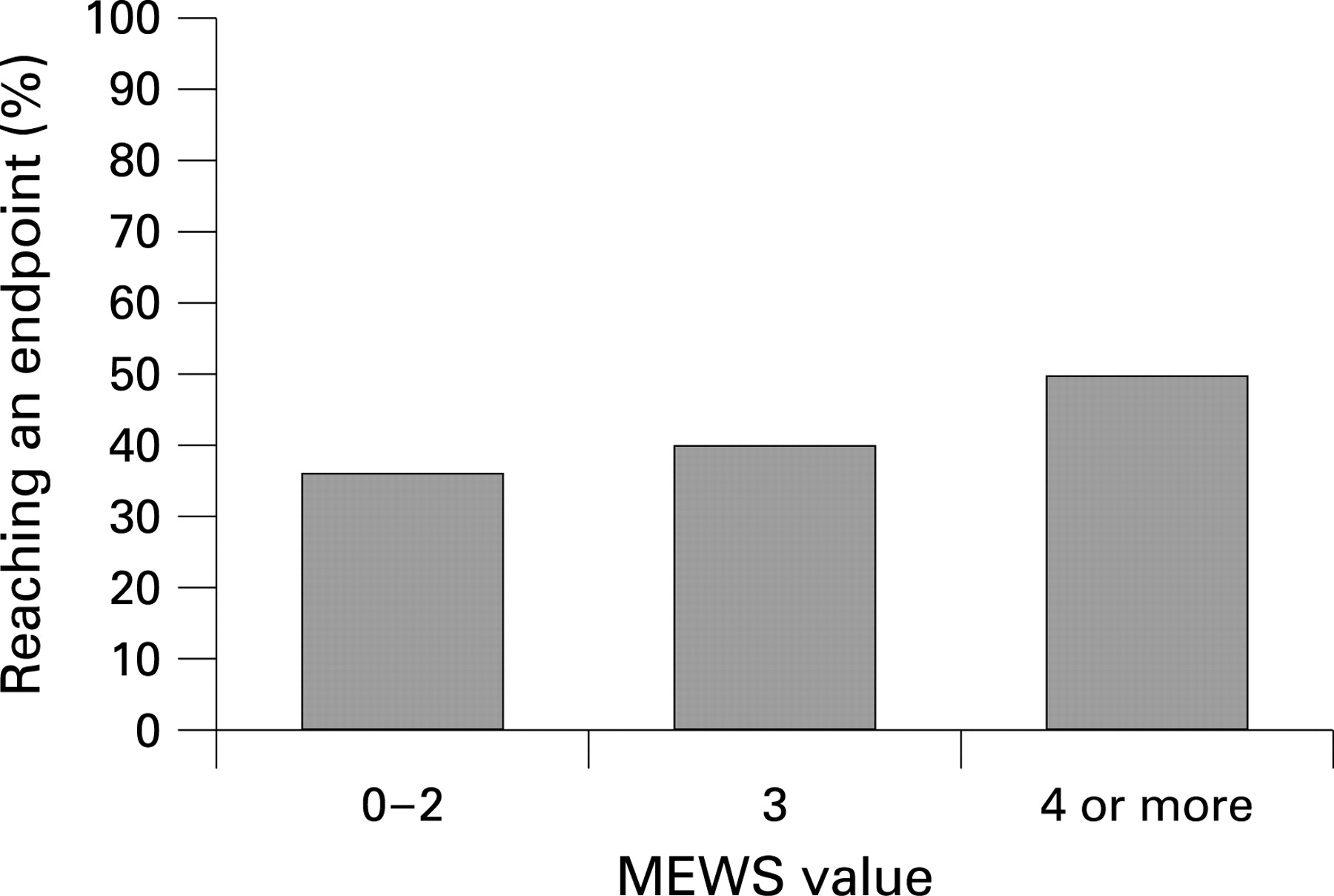
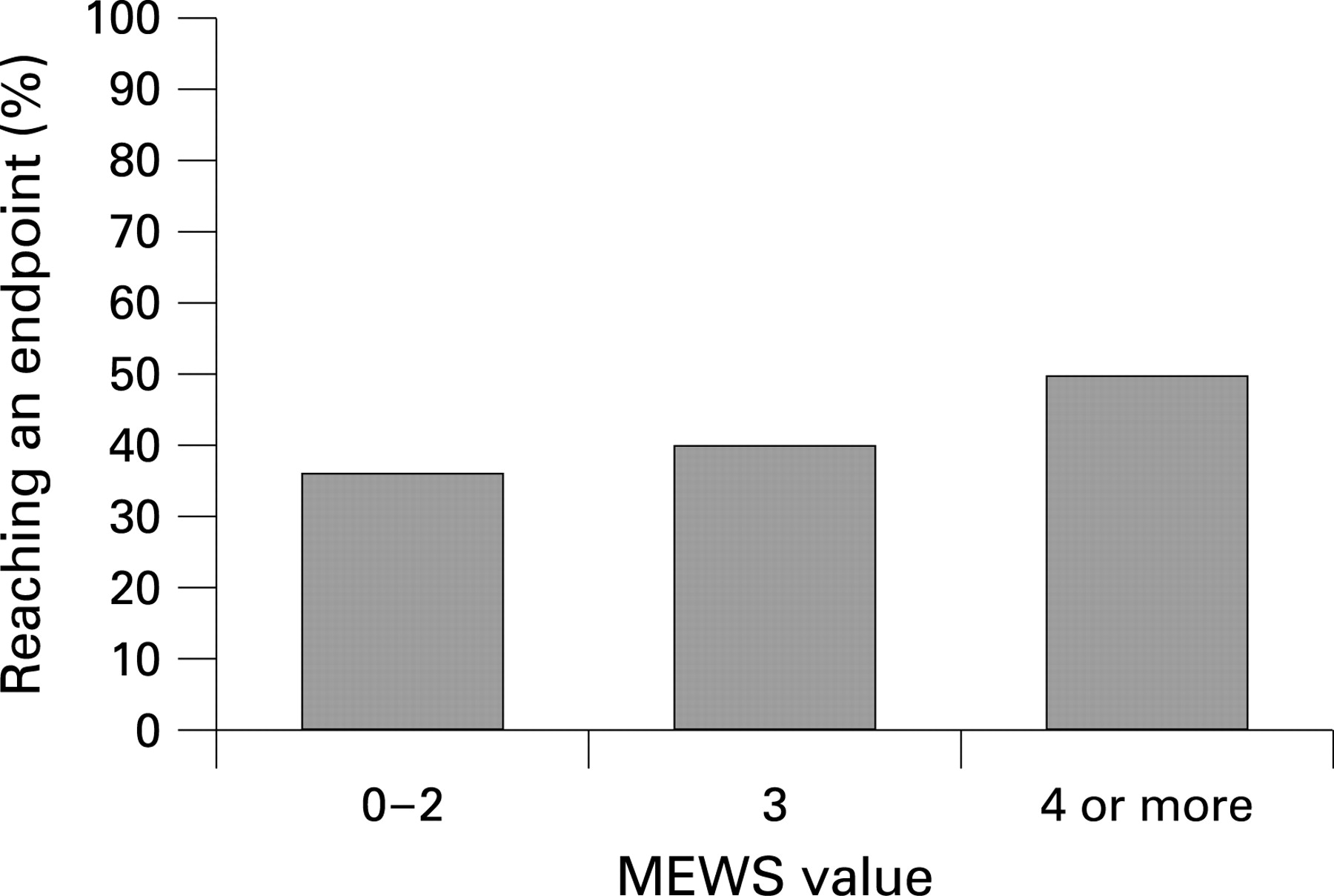
Figure 2 shows the relationship between the MEWS and likelihood of reaching an endpoint. Physiological parameters differed significantly between patients who reached an endpoint and those who did not (table 3). The most significant differences were observed for pulse and respiratory rate. There was no significant age difference between patients reaching an endpoint and those who did not. The MEWS on its own overtriaged 10% and undertriaged 43% of patients.
{kind=link}
{kind=link}
Step 2: Mobility score
A near-perfect Pearson correlation (r = 0.98) was found when the MEWS was compared with the TEWS. The only significant difference to be found was between the MEWS and TEWS of medical patients (p = 0.03); no difference was found for trauma or surgical patients. Overall, 35% (210 of 602) of walking patients (mobility score of zero) reached an endpoint compared with 61% (119 of 196) of patients unable to walk independently (mobility scores one or two). The addition of the mobility score marginally improved overtriage and undertriage (12% and 38%, respectively).
Step 3: Discriminator list
Specific discriminators were necessary for the triage of 356 patients (45% of total). By adding the discriminator list to the TEWS, the number of patients triaged green and reaching an endpoint decreased from 38% to 24% (p = 0.001). Conversely, the number of orange and red patients reaching an endpoint increased from 15% to 22% (p = 0.02) and 4% to 8% (p = 0.05), respectively. Overall, the CTS overtriaged 25% and undertriaged 24% of patients.
Identified CTS amendments
Based on these results, a number of amendments to the CTS were identified and evaluated by performing simulations on the CTS database. First, the mobility score did not appear to make a significant contribution to the CTS in this patient group and was therefore not used in any of the simulations.
The second was a change in the priority colour code assignment to patients achieving a given MEWS. A significant increase in the likelihood of achieving an endpoint was observed between patients achieving a MEWS of 3 compared with 4 (fig 2). The simulation subsequently used scores of 0–1 to triage green (CTS 0–2), 2–3 to triage yellow (CTS 3–5), 4–5 to triage orange (CTS 6–7) and a score of more than 6 to triage red (CTS more than 8).
Third, the discriminator list was amended to include three additional orange colour code discriminators not consistently picked up by the MEWS. These included diabetic ketoacidosis, stroke and haemoptysis.
Finally, a trauma-factor of 2 points was added to the MEWS of all patients presenting with physical injury (trauma). For the simulation, all trauma-related discriminators were removed from the discriminator list. Table 4 shows the main simulation findings resulting from the identified amendments when compared with the CTS.
DISCUSSION
A total of 82% of data sheets were retrieved with all fields completed. The sample size was sufficient to allow significant results. The demographics were a reasonable reflection of current South African society.
The CTS has already been shown to reduce waiting times significantly.20 Despite this achievement, high undertriage remains a concern. By evaluating each component of the CTS, potential amendments were identified and their relative contribution to improving the accuracy of the CTS was evaluated. The amendments identified included re-evaluation of the utility of the mobility score, colour code amendment, discriminator list amendment and the addition of a trauma factor. Including these amendments through simulation resulted in an improved undertriage rate (24–12%) resulting in the unavoidable but acceptable increase in overtriage (25–45%). It is agreed that an overtriage rate of up to 50% may be required to maintain an acceptable level of undertriage.19 Although it may be argued that undertriaging more than 10% of patients is unacceptable, it has to be understood that when an acceptable sensitivity (and thereby an acceptable rate of undertriage) is finally reached, specificity may be so low that triage would no longer be useful.21 Prolonged stays in the ED after diagnosis (up to 48 h) were responsible for the slightly raised undertriage rate.
As the first validation trial of the CTS, it was expected that fine-tuning of the MEWS translation to a priority colour code would be necessary. It was important to get the basis of the tool to function optimally. The amendment produced similar over and undertriage rates to the CTS, with the aid of a discriminator list.
A higher MEWS in this population related to a rise in admissions, but with medical bias. This bias was further skewed by the mobility score. The latter’s original purpose was to improve the MEWS to prioritise trauma adequately.5 This finding allowed its exclusion. Its minor contribution was emphasised by the near perfect correlation between the MEWS and the TEWS.
The MEWS has previously been shown to indicate critically ill patients in the ED comparable to the Manchester triage scale.14 It undertriaged 43% of patients in this population, however, necessitating the use (as predicted) of the discriminator list. This improved undertriage to 24% (and 12% with the amended version). This amended version could include stroke through use of the Cincinnati prehospital stroke scale and haemoptysis based on the history.22 Diabetic ketoacidosis could be accommodated by including finger prick blood glucose during triage followed by a urine dipstick if raised. Even though all of these were mostly triaged correctly by the MEWS, it was thought that no undertriage would be acceptable.
The most profound improvement to the MEWS followed the addition of the trauma factor. Adding the difference between the mean medical MEWS and the mean trauma MEWS to the MEWS of all trauma-related cases resolved their undertriage and permitted simplification of the discriminator list through removal of its entire trauma content (47%, 16 of the original 34 discriminators). Although the CTS discriminator list increased triage priority in 23% of cases, it was only required in 12% of cases when used with the trauma factor (trauma content of list removed). This effectively improved the existing MEWS triage capability whereas over and undertriage was not sacrificed. Including identified amendments as suggested should improve a potentially useful triage scale for local use in South African ED.
Limitations
The number of trauma cases evaluated was small, limiting the interpretation of the value of the mobility parameter or the inclusion of a trauma factor.
This study was performed at a single public sector ED and included no patients from the private sector. The external validity of this study therefore requires investigation in a separate healthcare setting and such a study has recently been undertaken.
The principal investigator as triage doctor was a potential, although unavoidable, source of bias. He was, however, blinded to the final outcome of patients in an attempt to limit this bias.
CONCLUSION
Given the high volume of patients accessing the South African public health service, it is clear that a triage system is required in South Africa. As triage scales currently used elsewhere may not be appropriate for use in developing countries, a triage scale is needed for local use.4 The CTS, including the identified amendments, is a simple system capable of dealing with large patient volumes and capable of predicting an admission endpoint over a wide spectrum of ED presentations. The acceptable overtriage and undertriage rate of the CTS when used with the amendments shows promise in South African ED service delivery. Several works are currently in progress to evaluate the value of the identified amendments. Meantime, the final version of the CTS is now in use throughout much of the country. By inclusion in the national trauma database its already significant impact on emergency care could be further evaluated.23
Acknowledgments
The authors wish to acknowledge the central committee of the Cape triage group as well as GF Jooste Hospital’s executive committee for their support of this project.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: The study was approved by the Research Ethics Committee of the University of Cape Town.
Contributors: SRB had the original idea, collected the data and wrote the first draft. All authors contributed to the final draft. SRB is the guarantor of this paper.
Linked Articles
- Primary survey