Article Text

Abstract
Introduction The delivery of high quality emergency medicine ideally involves input from senior doctors 24 h a day. This study aims to assess the influence of ‘real-time’ senior clinician supervision on patient disposition from a UK emergency department.
Methods The study was set in a UK teaching hospital with 24 h senior cover. Patients were initially seen by a junior doctor who completed a plan for the patient before seeking senior advice. Primary outcome measures were a change in patient outcome of discharge, admit, telephone speciality for opinion or outpatient follow-up.
Results 556 patients underwent senior review during the study period. Review reduced inpatient admissions by 11.9% (95% CI 7.2% to 18.2%) and specifically reduced admissions to the acute medical assessment unit by 21.2% (95% CI 13.5% to 30.8%). Inappropriate discharge was prevented in 9.4% (95% CI 6.2% to 13.7%) and appropriate use of outpatient facilities resulted in a rise of 34.6% in appointments.
Conclusions Senior doctor input in patient care in the ED adds accuracy to disposition decisions, impacting on patient safety and improving departmental flow.
- Emergency Department
- clinician
- clinical governance
- admission
- clinical assessment
- emergency care systems
- advanced practitioner
- management
- risk management
Statistics from Altmetric.com
- Emergency Department
- clinician
- clinical governance
- admission
- clinical assessment
- emergency care systems
- advanced practitioner
- management
- risk management
Introduction
The current model of staffing within UK emergency departments (EDs) results in junior doctors delivering the majority of care. The College of Emergency Medicine, however, states that the delivery of high quality emergency medicine now requires a senior doctor to be available 24 h a day.1
EDs see a large volume of cases of varying complexity. Studies of the performance of junior doctors in EDs show they are seeing fewer patients than their predecessors2 and feel less confident in their clinical skills.3 To address educational and service needs, the speciality is undergoing an expansion in consultant numbers, the effect of which can be measured in terms of patients seen and specific objectives such as achieving the 4 h target. However, the added quality value of ‘shop floor’ senior emergency physicians is more difficult to quantify. Published studies have looked at specific aspects of care. In a study of blood tests in the ED, Knott and Meyer failed to show any association between medical seniority and a change in disposition or correctly identifying those patients whose outcome might be altered by the blood test result.4 While this was a small study, the results were unexpected.
An observational study in March 2003 investigated measures taken to improve departmental waiting times.5 Many departments had increased senior doctor hours in addition to numerous other factors. The data gathered failed to show a performance benefit from increased senior doctor input. This, however, contradicted results published from New Zealand following a review of practice during the junior doctors' strike in 2006, which showed that one senior doctor covered the workload of 2.6 juniors and that both waiting times and length of stay in the ED were reduced.6
The aim of our study was to assess the influence and effect of ‘real-time’ senior clinician supervision on patient disposition from a UK ED.
Methods
The Tayside region of Scotland has a population of approximately 450 000 and is served by two EDs, one in Ninewells Hospital, Dundee and the other at Perth Royal Infirmary. Senior medical staff consists of six consultants, one associate specialist and nine whole time equivalent middle grades (specialist trainee (ST) 4 and above) providing cover to both departments. There is a 24 h middle grade presence in Ninewells Hospital, with consultant presence between 08.00 h and 00.00 h on weekdays and between 08.00 h and 18.00 h at weekends. Outside these times, consultants are on call for both departments. The department operates a policy whereby no patient is referred to another speciality for admission or review without prior discussion with a senior ED clinician. All referrals are made to speciality doctors of ST3 grade or above. Together the departments see approximately 75 000 new attendances per year, with a typical case mix (66% minors, 22% majors, 11% resuscitation, 18% paediatrics and 23% admitted). During 2007, 48 044 new patients attended the ED at Ninewells Hospital resulting in 10 742 admissions to inpatient beds, of which 45.5% (n=4891) were to the acute medical assessment unit (AMAU) and 14.8% (n=1585) were to the orthopaedics department. ED referrals to AMAU represented 37% of their overall admissions, the remainder being admitted directly from primary care. From all admissions to AMAU, 15% of patients are discharged within 24 h. NHS Tayside encourages the direct admission of patients from general practitioners to inpatient specialities, without going through the ED unless clinically indicated.
The ED includes eight observation beds for problems such as head injury or overdose where inpatient admission is not required. Patients are discharged from these beds within 24 h.
This study was conducted in the ED at Ninewells Hospital twice weekly between February 2008 and August 2008. The study times were based on the availability of the research nurse. Following their assessment of a patient and before consultation with a senior clinician, junior medical staff (Foundation Year (FY) 2 or ST1/2) completed a form documenting a provisional diagnosis and proposed management. Four outcome options were available: discharge, admit, telephone speciality for opinion or outpatient follow-up. Following review, the senior doctor then documented his/her diagnosis and disposal using the same options. Patients requiring immediate emergency management were excluded.
During the study period a research nurse circulated in the department recording the number of patients attending and encouraging form completion. Additionally, the nurse reviewed attendance cards for all recorded patients ensuring appropriate form completion where applicable.
At the end of the study period all patients who had a change of disposition from admission to discharge by the senior doctor were reviewed. The ED computer system (Symphony) and the hospital administration database (TOPAZ) were interrogated for any repeat attendance or admission in the 7 days following discharge.
Based on an initial pilot study, a required sample size of 483 review patients was calculated to test a 24.3% difference (99% confidence level). The results were analysed using Microsoft Excel 2007. The primary outcome measure was a change in the disposition decision for the patient.
Results
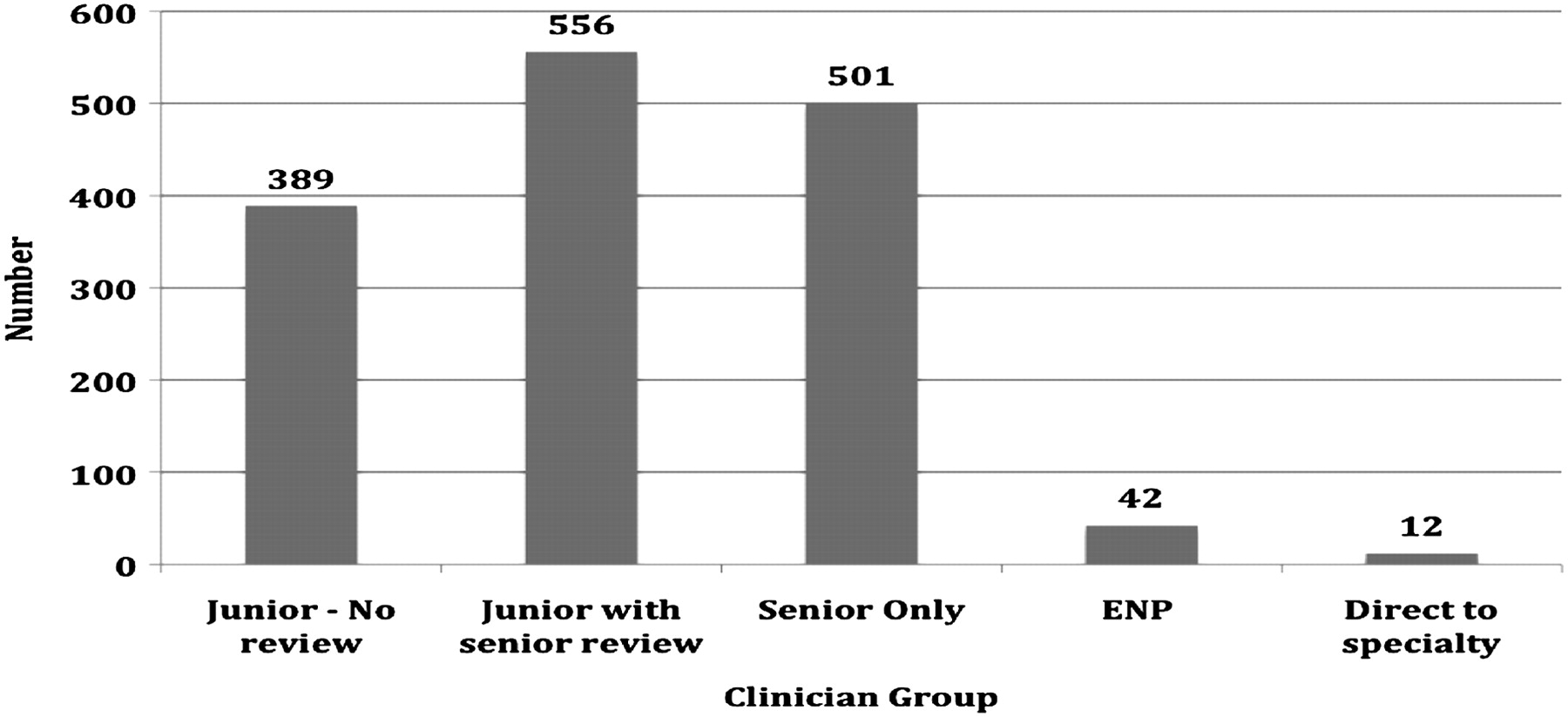
Between the 25 February 2008 and 4 August 2008, a total of 1500 patients attended during 46 data collection periods. Five hundred and fifty-six patients seen by junior clinicians were subject to review by a senior clinician. Form completion was 99.6% with two forms lost and untraceable. The senior doctor changed the primary outcome plan in 155 patients (percentage change 27.98% (95% CI 24.4% to 31.8%)). Senior doctors were directly involved in the care of 1057 patients (70.5%). Figure 1 shows the breakdown of the personnel involved with patient care in the ED.

{kind=link}
Bar chart showing number of patients seen by each clinician group. ENP, emergency nurse practitioner.
Following senior review, 26 of the proposed 165 patients to be admitted were immediately discharged with no follow-up, representing a reduction in admissions of 15.8% (95% CI 10.8% to 21.9%). Of those 26 patients, two were readmitted within a week, one with a repeat overdose (observed in ED and discharged) and a patient with pericarditis with increasing chest discomfort. The pericarditis had not been diagnosed at first attendance and resulted in admission to cardiology. Of the proposed 85 admissions to the AMAU, 25 were prevented, corresponding to a reduction in admissions of 29.4% (95% CI 20.5% to 39.7%).
Some of the patients initially recommended for discharge, follow-up in the outpatient department or discussion with a speciality doctor were identified by senior review as requiring inpatient admission or short-term observation in the department. Table 1 shows the net figures for admission following all reviews.
Net changes to admissions
From the 233 patients recommended for discharge by junior trainees, the senior review process identified 22 (21 with no follow-up, one with follow-up in the outpatient department) as being inappropriate. Ten of these patients required immediate admission, with outpatient department follow-up being arranged for the remaining 12. Of the 10 admissions, 7 were to the AMAU with unrecognised unstable angina (two patients), symptomatic bradycardia, coagulopathy, transient ischaemic attack and reduced mobility (two patients). This represented a 9.4% (95% CI 6.2% to 13.7%) prevention in inappropriate discharge. Overall, patients being discharged with no follow-up or back to primary care rose by 52, equivalent to an increase in discharged patients of 22.3% (95% CI 17.3% to 28.0%).
Senior review prevented unnecessary speciality referral for review or opinion in 64 patients, equating to a referral reduction of 61.5% (95% CI 51.9% to 70.5%). In addition, the senior review process prevented speciality referral and potential admission by appropriately using outpatient department follow-up in a further 18 cases (percentage increase 34.6% (95% CI 22.7% to 48.2%)).
Table 2 shows the proposed management of patients by junior trainees, with the subsequent effect of the senior review process.
Comparison of patient disposition
Discussion
Patients attending the ED are different from those seen in admission wards, general wards and outpatient clinics. They tend to be an undifferentiated patient group who have had no screening by primary care. Emergency physicians are trained to make patient discharge decisions on the basis of a focused clinical assessment and limited use of other investigations, in contrast to other specialities who deal with a different cohort of patients requiring admission for more complex investigations. As such, experienced emergency physicians have a unique skill set that is suited to performing a risk assessment and making decisions with less information to hand. They have an important role in overseeing the work of less experienced doctors as part of their job plan.7
Clinical supervision centres around key steps in the patient care pathway: focused clinical assessment, relevant investigations, initial treatment and correct disposition.8 Effective supervision of junior doctors should improve the quality of patient care, the accuracy of decision-making and the flow of patients through the ED. This study examined the effect of ‘real-time’ or ‘shop floor’ supervision in the ED on discharge decisions.
Senior doctors in the ED at Ninewells Hospital are directly involved in the care of 70.5% of patients. This study clearly highlights the effects of their involvement both on patient care and management, ensuring appropriate management, referral and disposition, and from a risk management perspective, prevention of inappropriate discharges. In addition, their involvement significantly influences the ED-generated workload of hospital subspecialities with a contact reduction of 61.5%. Perhaps one of the most striking findings was a 21.2% net reduction in admissions to the AMAU which, in common with all other UK hospitals, receives the majority of inpatient hospital admissions. At a time when UK departments continue to see rising admission rates and hospitals struggle to manage capacity, the presence of a senior emergency medicine decision maker on the shop floor can have a significant effect in reducing hospital admissions. This may be due to a number of reasons:
Clinical knowledge, experience and training resulting in improved risk assessment and management.
Clinical judgement.
Confidence in clinical assessment.
Knowledge and appropriate utilisation of alternative sources of care (eg, outpatient clinics, primary care services).
Real-time senior review of cases ensured that patients were referred to the correct speciality or to the correct outpatient clinic. This approach appears to improve the accuracy of disposition decisions made in the ED. When admitted, the patient is referred to the most appropriate speciality, thereby improving the patient journey and reducing consequent transfers between inpatient wards. The combination of real-time review and direct admission rights reduces the admission time lag and bottle neck associated with the traditional model of ED care in which a patient is assessed by an ED clinician, referred to and subsequently reviewed by a speciality who then arranges admission. Specialities are telephoned regarding patients where an admission decision has already been made and, in these cases, it is a basic courtesy call for the transfer of patient details and will usually be undertaken by a member of the nursing staff. Senior review prevented 61.5% of telephone calls to speciality for advice, so reducing the time spent by junior doctors on the telephone and improving their turnover of patients. There is also an advantage for the inpatient speciality as their on-call teams are not disturbed so frequently, allowing them to concentrate on their duties in an admission ward or elsewhere.
Perhaps more important than the effects on admissions and telephone calls is the effect on inappropriate patient discharge by inexperienced trainees. This study demonstrates the clinical governance benefit of real-time senior review where the prevention of inappropriate discharges has potentially significant implications for patient safety. While the exact impact on patient safety is difficult to measure, the literature relating to missed abnormalities on x-ray supports the view that real-time supervision of junior staff reduces errors in diagnosis and clinical decision-making.9
Jayne et al looked at improving night-time supervision in the ED by a distant specialist registrar covering multiple sites using the facsimile and telephone.10 They compared management plans by the SHO and SpR and found a change in clinical care in 47% of face-to-face consultations. They concluded that economic savings from remote senior supervision would include avoidance of outpatient appointments and inappropriate investigations and admissions. The cost implications and possible bed days saved following senior review requires further investigation.
This study had limitations. Both junior and senior doctors were fully aware of the study periods and may have altered their practice in view of the increased attention, with junior doctors possibly not wishing to ask as often and senior doctors eager to make changes. Reassuringly, the figures compare well with the pilot study and with other published data.10 The senior doctors were not blind to the junior doctors' management decisions, but this was a real-time study and the authors do not believe the junior opinion would influence the senior to the extent of introducing unacceptable bias.
Based on the pilot data, a sample size of 483 was calculated. This figure was reached earlier than expected, realising a potential bias from junior trainees asking more questions as it was towards the beginning of their emergency medicine attachment. The study was therefore continued for a full junior doctor attachment term, thereby including the final months when they were arguably able to demonstrate more independent practice.
This system of review requires a sufficient number of senior doctors to be directly available for consultation. It is difficult to predict the exact number of senior clinicians required to sustain this effect, however this department's previous work on the 4 h target demonstrates the increased availability of senior doctors impacts on improved flow. This is an area for further research.
Conclusion
Over the coming years the number of emergency medicine consultants is likely to increase owing to strategic decisions made to produce a trained workforce.1 It is important that this change is seen to benefit patients and hospitals in general. This study lends evidence to the suggestion that senior doctors add accuracy to disposition decisions. The presence of consultants on the shop floor in increasing numbers should improve patient safety, training of juniors and significantly assist capacity and flow issues faced by all major institutions.
Summary box of key results
Real-time senior review reduced AMAU admissions by 21.2%.
Inappropriate discharge was prevented in 9.4%, adding to patient safety.
Appropriate utilisation of outpatient facilities resulted in 34.6% increase in appointments.
Acknowledgments
The authors gratefully acknowledge and appreciate the administrative support provided by Research Nurse Susan Henderson.
Footnotes
Competing interests None.
Ethics approval Neither ethics approval nor patient consent was required for this study as there were no changes to normal department practice. However, all doctors involved provided verbal consent with the understanding that all forms were anonymised.
Provenance and peer review Not commissioned; externally peer reviewed.