Article Text

Abstract
Objective To determine the causes of emergency department (ED) crowding and to identify evidence-based solutions.
Design The review used a ‘conceptual synthesis’ approach to identify knowledge and opinion around the issue of ED crowding, not just effective interventions. Recommendations from the literature were classified according the quality of evidence and the extent to which they were under ED control.
Data sources SCOPUS and ISI were searched for studies of ‘ED’ AND ‘crowding OR overcrowding’ and backward citation retrieval was undertaken. To help identify systematic review evidence of effective interventions, the Cochrane Database, the National Institute of Health and Clinical Excellence (NICE) and NHS Evidence were searched. A Google search was included to identify relevant grey literature.
Eligibility criteria Papers were included if they added to substantive knowledge of ED crowding. Empirical studies, studies from the UK and studies of physical space were privileged in the review.
Results There is an established international literature on ED crowding. It suggests consistently that crowding has significant negative consequences. However, the literature offers limited practical help to practitioners for a number of reasons, such as a lack of shared definition and measurement of crowding and lack of evaluation of interventions. Many studies are single case studies from the USA.
Conclusions While current evidence is poor, this does not justify maintaining current practice which risks lives. Building up an evidence base is critical, but requires agreed definitions, measures and methods, which can be applied to systematic evaluation of plausible solutions.
- Emergency care systems
- emergency departments
- emergency care systems
- effieciency
Statistics from Altmetric.com
Introduction
Emergency department (ED) crowding is of international concern as crowding is associated with significant negative outcomes, including unnecessary deaths.1–6 In Australia, for example, ED crowding and access block (defined as waiting for an inpatient bed for over 8 h) have been estimated to result in a ‘20–30% excess mortality. This equates to approximately 1500 deaths per year…similar to the road death toll’.7
Concerns about the negative impact of crowding have lead to papers and reports which seek to identify effective interventions,1 8 9 but there is currently no common guidance for practitioners and policymakers. Some report single case studies.10 11 Others focus on particular aspects of emergency care, such as strategies to reduce attendance,12 best practice for delivery of pre-hospital emergency care,13 or strategies designed to reduce ED waiting times.12 14 The report from the Alberta Heritage Foundation for Medical Research, Strategies to reduce emergency department overcrowding, reviewed interventions with quantified outcomes.8 However, in doing so it may have excluded studies that had substantive merit but were either poorly designed or where outcomes were difficult to measure.15 While these reports make a welcome contribution, none provide a comprehensive conceptual or evidence base from which to proceed.
This paper reports findings from a broad review of existing literature on ED crowding and is designed to provide an assessment of what is currently known about ED crowding: its impact, causes and consequences. It is organised around a conceptual model of crowding found in the literature. The review aims to provide a critical evaluation of the available evidence on effective solutions to crowding and to consider their feasibility. It is intended to provide a review of the evidence base and to inform future research and evaluation.
Methods
We reviewed the literature on ED crowding. We performed a ‘conceptual synthesis’,16 designed to identify and synthesise existing knowledge and debate around the problem of ED crowding rather than seeking to identify effective interventions only. This ensured the literature search was comprehensive, covering both conceptual and empirical literature, as well as addressing the emergency care system.
Searches were conducted to identify papers relevant to crowding or overcrowding in EDs. We searched SCOPUS and ISI for studies of ‘ED’ AND ‘crowding OR overcrowding’. We then undertook backward reference tracking to identify related work.17 Empirical studies from the UK were proactively sought and included. New papers were included in the review if they added new information to the existing body of knowledge. To increase the confidence that the search had identified any systematic review evidence of effective interventions, we also undertook targeted searches of the Cochrane Database, National Institute of Health and Clinical Excellence (NICE) and NHS Evidence for any guidance. We included a Google search to identify relevant grey literature.
The retrieved literature was organised around the following themes: conceptual issues, causes, consequences of crowding and solutions. Evidence on interventions was graded using a standard evidence-based medicine methodology18 in order to assess the quality of the design and the level of recommendation. Potential solutions were also assessed as to whether or not they fell under the control of the ED.
Main findings
Definitions
The review revealed several definitional issues which are relevant to practice. There is a lack of definition of what constitutes crowding.8 19–22 The issue is sometimes referred to as ‘crowding’ and other times as ‘overcrowding’.2 There is no agreement whether ‘boarding’ or ‘access block’, both terms used to describe the practice of keeping a patient who requires admission in the ED while they wait for an inpatient bed, is a cause,23 24 a consequence25 or a measure of crowding.26 The same problem arises around waiting times and whether they result from crowding,27 28 are a measure of crowding or lead to crowding.5 25 29
Hwang and Concato stress the need to have some conceptual discipline because ‘(s)eparating factors that cause overcrowding from the phenomenon itself can assist in the development of interventions that ease overcrowding’.19 This lack of clarity also makes drawing conclusions about effective interventions more difficult, as studies do not compare like with like.8
Effects of crowding
The negative consequences of ED crowding are a recurrent theme in the literature.1 2 4–6 12 Delays in diagnosis and access can result in unnecessary death and disability.4 8 Crowding can also lead to delays in administration of antibiotics and thrombolytics,6 and increased errors such as mislabelling radiology and pathology request forms.28 In the USA it is estimated that ‘50% of the sentinel events causing serious injury or death occur in emergency departments and one third of these are related to overcrowding’.1 ED crowding is associated with higher proportions of patients leaving the ED without being seen, many of whom need medical care.6
Crowding also impacts on patient experience, with patient satisfaction impaired as waiting times increase.12 It is also claimed that as patients grow more frustrated with waiting, violence towards staff increases.28 30 Delays in treatment due to crowding can also cause prolonged pain and anxiety.2 28 31 Crowding may also inhibit open discussions between patients and the staff,2 as well as undermine patient privacy, confidentiality and dignity.2 32
The literature also suggests that crowding impacts directly on ED staff, reducing productivity and effectiveness.6 28 Crowding is also thought to contribute to staff burnout and high staff turnover.33–35 This leads to greater use of less experienced staff who are less able to provide high quality emergency care.33
A problematically crowded ED has consequences for an entire hospital and health system, challenging infection control36 and the ability to respond to major incidents.37 Ambulance diversion or bypass provides a solution for one ED by adding to the burden of others.1 5 28 33 34 In general, longer ED stays are associated with longer hospital stays independent of acuity.34 37 This makes meeting elective care targets even more challenging as competition for inpatient beds from unplanned admissions increases further.38
ED crowding is also associated with ‘boarding’; this is where patients remain in the ED while waiting for an inpatient bed to become available. Critical care patients who ‘board’ receive suboptimal nursing which may contribute to longer inpatient stays.1 2 Boarding patients will also be subject to additional moves; each move is estimated to add a day to the hospital stay.39
Conceptual models
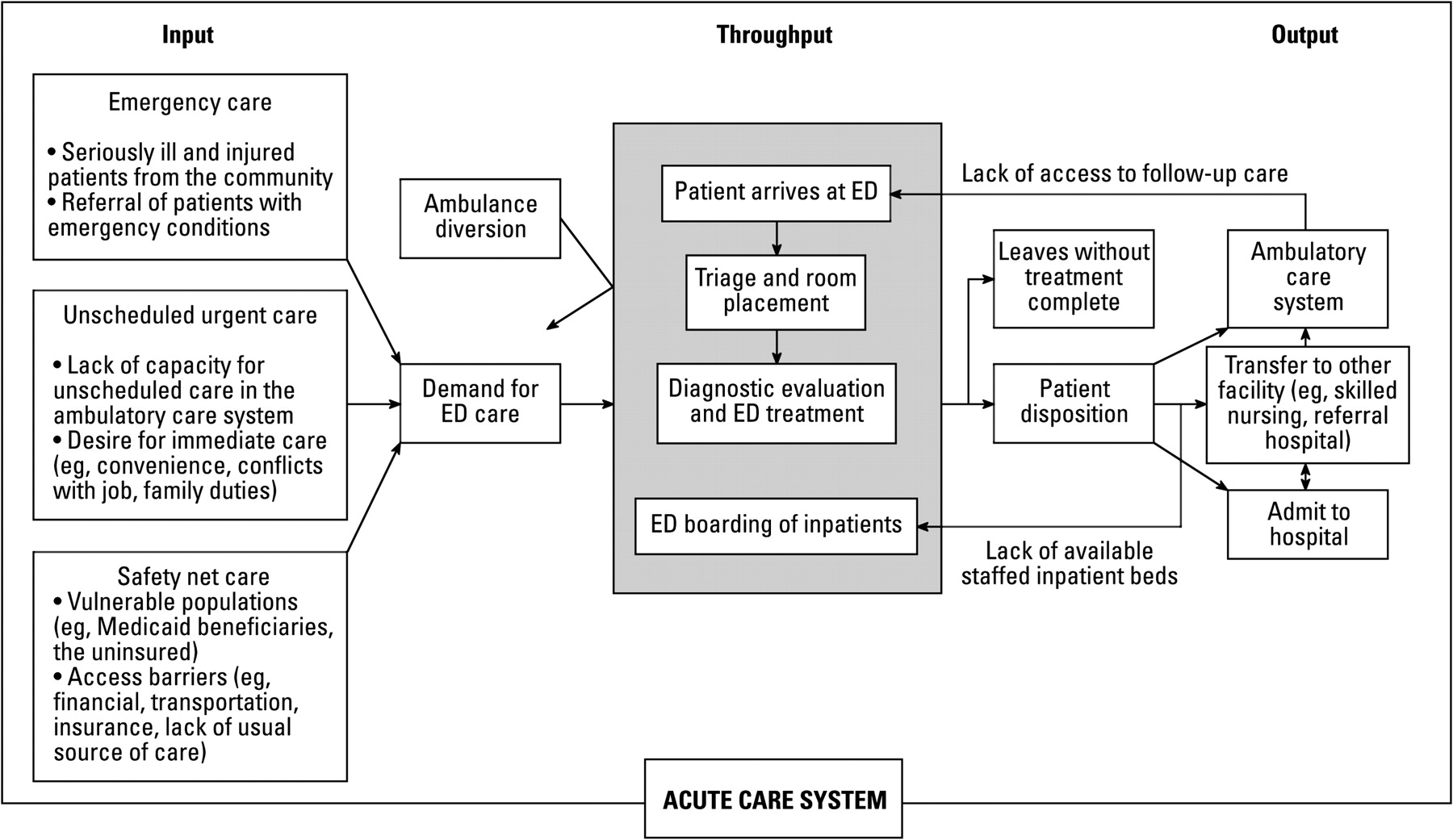
The effects of crowding underline EDs' position as part of a complex healthcare system and it can be helpful to ‘model’ the crowding process to help understand causes and to identify appropriate solutions. Three overlapping conceptual models have been identified,10 29 40 all of which have limitations. We used the model of Asplin et al40 as an organising framework because it focuses on the health system relevant to emergency care rather than processes within the ED. This model is presented in figure 1.

{kind=link}
Model from Asplin et al40 of the crowding process in emergency departments (EDs).
The model has three interdependent components: inputs, throughputs and outputs. Input factors relate to the volume and type of patient attending. Throughputs are the factors that influence the ED's response to process patients efficiently and effectively. Output factors are those that limit the ED's ability to discharge patients, and are probably better regarded as constraints to desired outputs. This way of modelling the demand and supply of emergency care provides a useful way of linking causes of ED crowding with likely solutions.
Causes of crowding
The largest cause of crowding is the flow of patients into the department. This is influenced by the volume and nature of the demand.9 41 In the USA particular attention is given to the uninsured.34 40 Internationally, demand for care has increased due to population ageing, but is not just about increasing numbers. ‘Older people typically need more care in the emergency department, so a small increase in the number of elderly patients creates a large increase in demand’.42
Demand is also influenced by wider provision. In England, rises in the numbers of ED attendees since 2004 are partly explained by the retraction of primary care services.41 43 The time-based 4 h standard in the UK has also probably increased flow into EDs, by making access more available.43 The 4 h standard has led to significant activity in the last 20 min of a patient's stay in an ED. There are concerns that the standard is set too high, does not benefit patient care and may distort clinical priorities.44 45
Conceptually, input into an ED need not cause crowding if the department has capacity and capability to deal with the flow; the issue is the pressure caused by the back-ups which occur when the ED cannot cope with the demand. How patients are processed in the ED relates to throughput factors. For example, shortages of nurses, junior medical staff and specialty doctors impact heavily on crowding.5 34 46 One official report in England estimated that 27% of waits over the official 4 h target were due to patients waiting for a specialist opinion.47 Studies also show that often staffing levels do not match patient flows.35 Boarded patients reduce the ED staff available to treat new patients and slows down movement through the ED further, increasing crowding in turn.38
Numerous other factors that hinder the ability of the staff to process patients are associated with crowding. Poor physical design and shortage of physical space,5 23 28 48 equipment and computers,12 35 difficulties in accessing medical notes,40 46 tests, results and ancillary services,5 28 29 33 34 46 49 and time spent on discharging or arranging follow-up appointments are all thought to contribute to crowding.40
Lack of inpatient beds which force EDs to keep patients who are ready for discharge is the most mentioned output constraint.28 29 33 37 38 40 49 50 Lack of inpatient beds was reported to result from general lack of provision, delays in cleaning,38 40 lack of staff to care for new patients,40 delays in inpatient discharge,40 or increased demand for beds.41 In the USA, it is argued that financial incentives serve to prioritise elective surgery over emergency admissions.33 49 As patients waiting for inpatient admission tie up staff and space, their waits impact further on all patients in the ED.51 Constraints are also found in discharging patients safely into the community. Lack of community and psychiatric care and poor access to transport hamper discharge and contribute to ED crowding.28 33 47 52
Interventions
Input solutions
Interventions relating to input typically attempt to divert patients out of EDs. Some of these aim to discourage use13 53 and include co-payment54 and policies to encourage self-care.55 ‘Gate keeping strategies’, such as telephone triage48 or GP referral to an ED as in Denmark,54 aim to filter out ‘inappropriate’ users. Some question the underlying premise that many more patients use emergency services unnecessarily.5 56
Some of the diverted patients are expected to make use of alternative services. Emergency care practitioners provide pre-hospital care to patients to avoid the patient being taken to hospital. This is expected to reduce the number of ambulance journeys and saves money,57 but evidence of success is as yet unclear46 and there have been questions over the safety of emergency care practitioners.57 A major evaluation of this role found that emergency care practitioners were probably cost effective, but that the effect varies across settings. The role is relatively nascent at present.58
In England, NHS walk-in-centres also appear to have failed in their aim to reduce to demand for ED services and probably address previously unmet need.59 There is a substantial literature which questions the efficacy and appropriateness these sorts of interventions,12 with many UK ED attendees having tried to seek alternative care before arrival at the ED.60
Another potential solution to reducing demand for emergency care is the provision of better injury and disease prevention.48 Much of this is focused on elderly patients as the largest group of users of emergency care.42 Related interventions include active case management for patients with chronic disease, but the challenge of providing such services is significant and the benefits unclear.12 15
Ambulance diversion is used to force patients to another hospital; this is common outside the UK, but occurs rarely in the UK outside the major urban centres.
Throughput solutions
Throughput solutions focus on managing staff, space and processes within the ED better. Many throughput solutions have been suggested, based on engineering approaches that help practitioners analyse and redesign their systems22 35 54 61 in order to cut out unnecessary steps or to better match staff to patient flows.1 5 31 62 63
A number of potentially wasteful processes are identified in the literature. One study suggested that 75% of the time spent by a typical patient in an English ED is spent waiting.35 Triage is seen by some as a ‘non-value adding task’, particularly when beds are available.10 One study found that high level triage (consultant triage) reduced average waiting times, particularly for people in lower triage categories.64 However, the study questions the sustainability of the approach due to the intensity of patient contact, and the cost effectiveness of the approach was not assessed. Streaming is recommended as a way of dealing quickly with patients who require simple interventions.47 65 Bedside registration for trolley patients may also speed up processing and allow tests to be ordered more quickly.10 22 63 Faster access to diagnostic services and specialist care should also reduce wait times and queues.28 47 Use of protocols for common conditions, such as asthma, are recommended to improve the throughput of some patients.22 48 For instance, Eitel et al cite a study using algorithms to treat asthma which reported reductions in ED length of stay by 50 min, in hospital admission rate from 31% to 23%, and in revisit rates from 16% to 7%.22
Other solutions to crowding identified in the literature include using different staff and using staff differently. For example, emergency nurse practitioners are increasingly and efficiently used throughout the UK.46 Scribes for documentation are advocated in the USA,1 where it is estimated that emergency physicians spend between 90 and 120 min per 8 h on documentation.1 Other suggestions include the use of mental health nurses to provide specialist support,52 social workers to help facilitate timely discharge,66 and patient flow coordinators to coordinate diagnostic results, admission, and so forth.63 While plausible solutions, these roles and service are underdeveloped in practice and single case study evaluations show little impact.
There is some discussion in the literature on making more use of the understanding of individual and organisational behaviour to bring about improvements in practice, particularly in the context of change. This can mean understanding motivations and expectations, and designing systems that support behaviour change,1 10 but may also include monitoring of staff performance.67
A UK report examining waiting times found that the management behaviour of the lead clinician had an important effect in influencing waiting times. Specifically, waiting times were shorter in EDs where the lead clinician was proactive and adopted a participative style. The report also showed that waiting times were shorter in EDs that had good collaborative working with primary and inpatient teams.14
The literature included recommendations for changes to infrastructure to help ease crowding. Expansion of physical space is an obvious solution. However, most case studies seem to conclude that increasing capacity of an ED is unlikely to be helpful if flow problems are not taken into account.63 For instance, the Albert Einstein Medical Centre in Philadelphia was nearly doubled in size, but reported that this had little impact on the level of ambulance diversion (their measure of crowding).63 Observation wards and clinical decision units are considered useful when used properly,5 47 54 62 but may be less helpful when they compete for the same physical space as the ED itself. Some describe the use of such facilities as ‘dumping grounds’68 or ‘breach avoidance units’ for would-be boarders. Combining specialty admission units staffed by specialists in the ED has been shown to reduce admissions.69
Output solutions
The aim of output solutions is to reduce the delay in getting patients home or into the hospital when they no longer require emergency care. Suggestions for expediting community discharge include improved access to transport, better integration of coordination of care for patients who need community-based support35 47 and use of a hospital discharge lounge.31
A number of interventions have been proposed for improving output from the ED into the hospital; most obviously increasing capacity,48 and improving utilisation of and discharge from inpatient beds.1 31 37 The risk is discharging patients too early and thus facing readmissions.70 Admitting patients to wards before all investigations are completed and without assessment by specialists is common in the UK, but proposed as a solution in the US literature.34 Cancelling elective care can create extra capacity,1 38 but has negative implications for the wider hospital. It is also helpful for in-patient teams not to admit elective patients at peak times and again match inpatient resources to demand by offering a 24/7 operating schedule.1
Admitting boarded patients to already full wards is controversial but the majority of the literature seems to argue that being on the ‘wrong’ ward is better for the patient and the hospital than being in the ED.1 63 71 Dignity, infection control and increased burden on staff time required to care for ‘outliers’ are potential issues.
Environment and physical layout
The role of the physical environment beyond basic size is not well covered in the literature and all studies represent opinion.
One report by NHS Estates concluded that many EDs ‘could have been better designed to support the functionality of the department’.72 The report offers a number of recommendations found elsewhere in the literature, such as designing rooms and spaces flexibly to allow the same room to be used by multiple patient types,63 73 and designing space that helps patients, visitors and staff circulate and exit easily and appropriately.11 73 The NHS Estate report brings attention to trade-offs: ‘surveillance’, the ‘degree to which patients are overseen by staff members’, can compromise privacy, and circulation space substitutes for treatment space. Despite the relative lack of literature on environment and physical layout, many of the solutions to overcrowding proposed in the literature require physical space to be added or changed, for example adding observation units, a separate minors stream, or a interview room for a mental health nurse. Many of the case studies reporting improvements to overcrowding in a particular ED feature changes to physical layout.10 11 One paper concludes that any physical redesign should only follow a process analysis and redesign to avoid reproducing inefficient behaviour and processes in a physically larger department.
Quality of evidence
The review identified a large literature on crowding in EDs, including suggestions of what practitioners could do to ease crowding. Knowing what they should do, however, is more difficult. The poor quality of evidence was a common concern in the literature6 53 and we did not find evidence-based recommendations from NICE or similar organisations. We aimed to evaluate the evidence we did find and grade the recommendations coming from the research, but found most research to be poor quality as measured by formal measures.18 Nearly all the research on interventions was based on either single descriptive case studies or expert opinion, and therefore does not provide a good formal basis for recommendation. Few were before and after studies.64
This may reflect the difficulty of imposing formal evaluation criteria designed for drug trials on health service delivery which is much more complex and multi-faceted. Some are concerned about the lack of randomised control trial (RCT)-style interventions,12 while others argue that EDs might not be appropriate environments for RCTs.15
However, there are also features of the literature which do not conform with formal standards. For example, some make unsubstantiated references to interventions having ‘led to universal improvements in patient throughput in EDs in the UK’ without presenting any actual evidence of change.74 Even the term ‘systematic review’ appears to have been employed loosely in most instances, and many ‘systematic reviews’ do not conform with strict definitions of systematic review common in healthcare.5 12 75 76 Many of the reviews also derive from the same primary studies and there is therefore a risk of over-interpretation.
Feasibility of solutions
There appears to be some consensus in the literature around the view that ED crowding is influenced by the wider healthcare system and that many solutions are systems-wide.37 40 62 We therefore sought to identify which interventions were under the control of the ED themselves. The majority of input solutions are either not under the control of the ED—for example, providing better community support for patients with chronic illness2 12 77—or only partly under its control as the interventions involve providing alternative provision. For example, an individual ED may control ambulance bypass, but fail in their duty to provide care to a community. The same is true of output solutions where discharging patients rely on actors in the wider health system: EDs cannot cancel elective care, add more inpatient beds, or improve access to community transport.
EDs have greater leverage over throughput solutions which relate to how the ED is organised and managed. These include decisions around protocol use and procedures, staffing roles, and levels and aspects of performance management, and some control over use of physical space and equipment. In addition, EDs are likely to have a primary role in increasing awareness of crowding issues and engaging proactively with other parts of the system to enable change.1 67 78
While ED crowding is an international issue, not all solutions are equally applicable to all countries. Most of the studies we identified came from the USA, and the US healthcare system is different to that in the UK. For instance, financial incentives are prominent in the US literature, and the detail may or may not be relevant in the UK context.
There also appears to be a lack of literature not on what works, but how. This can lead to difficulties in implementation but also interpretation. For example, in England the introduction of the 98% 4 h wait target has reduced the amount of time that patients spent in EDs and reduced crowding.44 45 This relatively short wait has lead other countries to cite England as a model of good practice.53 However, in England there are concerns that the target has lead to gaming79 and could compromise quality of care.80
Discussion
This paper aimed to provide a review of potential solutions to ED crowding, attempting to grade the evidence associated with each intervention. This is intended to provide a critical base from which to help emergency practitioners focus their efforts to develop future practice and research. We found considerable consistency across the literature on the consequences of crowding. However, the literature on solutions to crowding is comparatively less well developed and therefore less useful to practice. For example, the lack of consistency in definitions of crowding hinders distinguishing between the causes of crowding, crowding itself and the consequences of crowding, and few ‘solutions’ are backed up by evidence. EDs have most control over throughput factors—that is, how they treat patients, but less over input and output factors. This means that they are likely to struggle with the issue of boarders without support from other parts of the healthcare system.
The review also identified two significant gaps in this literature. One is the relative lack of discussion about the influence of physical space on crowding which was only addressed as part of an individual case study or in the grey literature. The second relates to the absence of analysis of why and how particular interventions work. As such, links between intervention and outcome remain implicit, untested and difficult to replicate.
A strength of the study is its comprehensiveness. Including grey literature found work on design and physical space, for example. Including literature on all aspects of crowding—not just solutions—allowed a more critical assessment of solutions by making explicit potential causal links between causes and solutions. A weakness of the literature in general, but reproduced in this review, is that many papers making recommendations build on the same original primary studies, which are limited in number. Attempting to grade the quality of the literature exposed major weaknesses and potential lessons for future research and practice. This is a literature rich with ideas and aspirations for improved patient care, but as yet, not one that is sufficiently robust to guide policy and practice when judged from the perspective of formal evidence-appraisal criteria.
This study has identified evidence gaps. We propose that a consensus-based definition of ED crowding is developed. This would help the evidence to advance in a more structured manner. The greatest gain from research evaluations is likely to come from interventions that either reduce input or improve output. Interventions around throughput are likely to have relatively minor effects. Wherever possible, we recommend that any evaluations use controls to improve methodological rigour.
Nevertheless, we believe that the lack of existing evidence does not justify maintaining current practice where this could forgo benefits to patients. This reflects Yach et al's observation in the context of public health, suggesting that tobacco control interventions were not ‘evidence-based’ when introduced but ‘represented sound judgement at the time’.81 Sound judgement was translated into interventions which were testable, and in time practice could be supported by an evidence base.
Critical to advancing practice, therefore, is understanding what represents ‘sound judgement’, what is feasible and acceptable in the context of ED crowding, and using this to change practice in a deliberate and considered way. Key elements of this will be to agree and use a shared definition of crowding to facilitate the development of interventions and their evaluation. The research and practitioner community needs to agree on what constitutes ‘robust enough’ evidence for effectiveness and, more importantly, produce evidence to this standard by systematically evaluating the outcomes of these changes to practice.
Acknowledgments
The authors wish to thank Professor P John Clarkson, Director of the Engineering Design Centre at the University of Cambridge, who provided financial supportto ZSM and KB to carry out the work.
References
Footnotes
Funding The review derives from work undertaken at the Engineering Design Centre funded by the UK Engineering and Physical Sciences Research Council (EPSRC), grant reference EP/E001777/1. The views or opinions presented expressed in this paper are those of the authors and do not necessarily represent those of EPSRC, its associates or its sponsors. The role of the EPSRC was to provide funding for ZSM's post-doctoral position and partial funding for KB's PhD training.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.