Article Text

Abstract
This prospective observational study aimed to determine the rate of success of reduction of dislocated hip prostheses using conscious sedation. In 101 consecutive patients presenting to the emergency department between August 2000 and February 2003 with a dislocated hip prosthesis, reduction was attempted using conscious sedation. The outcome measures of the study were (a) rate of success of the attempted reductions (b) rate of complication of the sedation or the procedure, and (c) rate of success in the three subgroups (based on degree of dislocation). The overall success rate was 62% (95% CI 53% to 71%). There were six complications: five related to sedation and one was a mild foot drop. The mean time to attempted reduction using conscious sedation was 1.83 hours and for an equivalent group who were excluded and subsequently required general anaesthesia the mean time was 10.9 hours. Reduction of isolated unilateral prosthetic hip dislocation using conscious sedation in the emergency department is safe and has a reasonable success rate. Prosthetic hip reduction can be attempted more quickly using conscious sedation than when awaiting general anaesthesia.
- conscious sedation
- emergency department
- manipulation
- total hip replacement
Statistics from Altmetric.com
Reduction of dislocated hip prostheses is usually performed under general anaesthesia. Often there are significant delays waiting for theatre and controlling patients’ pain in the interim can be difficult. A comprehensive literature search failed to identify any studies whose primary outcome was the rate of success of reduction under sedation. A single case report1 was found in which etomidate was used to facilitate reduction instead of “narcotics”.
An pilot study2 conducted in our department (1998–99; unpublished) demonstrated a success rate of 67% was possible using conscious sedation. Our aim in the present study was to prospectively establish the rate of success, and the nature and frequency of complications when reducing prosthetic hip dislocations using conscious sedation.
METHODS
We included adult patients presenting to the emergency department with an isolated, unilateral dislocation of a prosthetic hip between August 2000 and February 2003. Exclusion criteria were American Society of Anesthesiologists (ASA) score >2; neurovascular deficit; dislocation >12 hours; previous failure using sedation; inability to consent; refusal; only one doctor on duty or when it was considered “too busy”.
It has been the usual practice within our accident and emergency department to attempt reduction of dislocated hip prostheses under sedation for the previous 15 years. Since this study was an attempt to establish the rate of success and nature and frequency of complications, and it did not involve introduction of a new practice, ethical approval was not obtained.
Patients’ demographic details were recorded contemporaneously on a proforma and the patients were given intravenous morphine to control their pain. Patients were examined fully and specifically for any neurovascular deficit of the affected leg. All patients had an anteroposterior x ray of the hemipelvis. We calculated the degree of dislocation based on the contact between the femoral head with the acetabulum:
-
Grade A: more than 50%
-
Grade B less than 50%
-
Grade C none
These degrees of dislocation were arbitrarily decided upon as no classification could be found in the literature.
We then sedated all patients according to the guidelines for intravenous sedation for non-anaesthetists issued by the Royal College of Surgeons.3 Almost all patients received morphine for analgesia and intravenous midazolam for sedation. We performed all reductions in the resuscitation room with full monitoring and supplemental oxygen. Complications were defined as: desaturation to <92%; apnoea; Glasgow Coma Scale (GCS) score <9; systolic blood pressure <100; or aspiration. Once the patient was adequately sedated, the Allis technique4 was used to reduce the dislocated hip.
In this technique the patient is placed in the supine position while an assistant firmly holds the pelvis down by applying pressure to both anterior iliac crests. The operator stands on the trolley above the patient and flexes both the hip and knee to 90°. Axial traction is then applied to the distal femur and gradually increased while the femur is slowly externally rotated.
All doctors were advised to squat over the patient and then attempt to stand with their backs always straight to avoid having a back injury. Following successful reduction the hips were abducted, a pillow placed between them and a check x ray taken. All patients were referred to the orthopaedic team for admission.
Statistical analysis
A power calculation was performed based on the results of the pilot study (42 patients, success rate 67%). To detect a difference between grades A, B, and C we surmised that 33 patients would be required in each group, giving a sample size of 100.
We analysed the data using SPSS for Windows Version 10,CIA (Confidence Interval Analysis) and Excel 2000. The significance level was set at 5%. The main results are presented with 95% confidence intervals. Between group comparison of percentages was done using the χ2 test for association, and Fisher’s exact test was used when cell sizes were small. Comparisons of means was done using the independent samples t test.
RESULTS
A total of 204 patients were entered in the study between August 2000 and February 2003, of which 98 were excluded based on criteria given in the Methods section. Of the remaining 106 patients, one patient had a spontaneous relocation and four patients had incomplete data, leaving 101 patients for analysis.
Primary outcomes
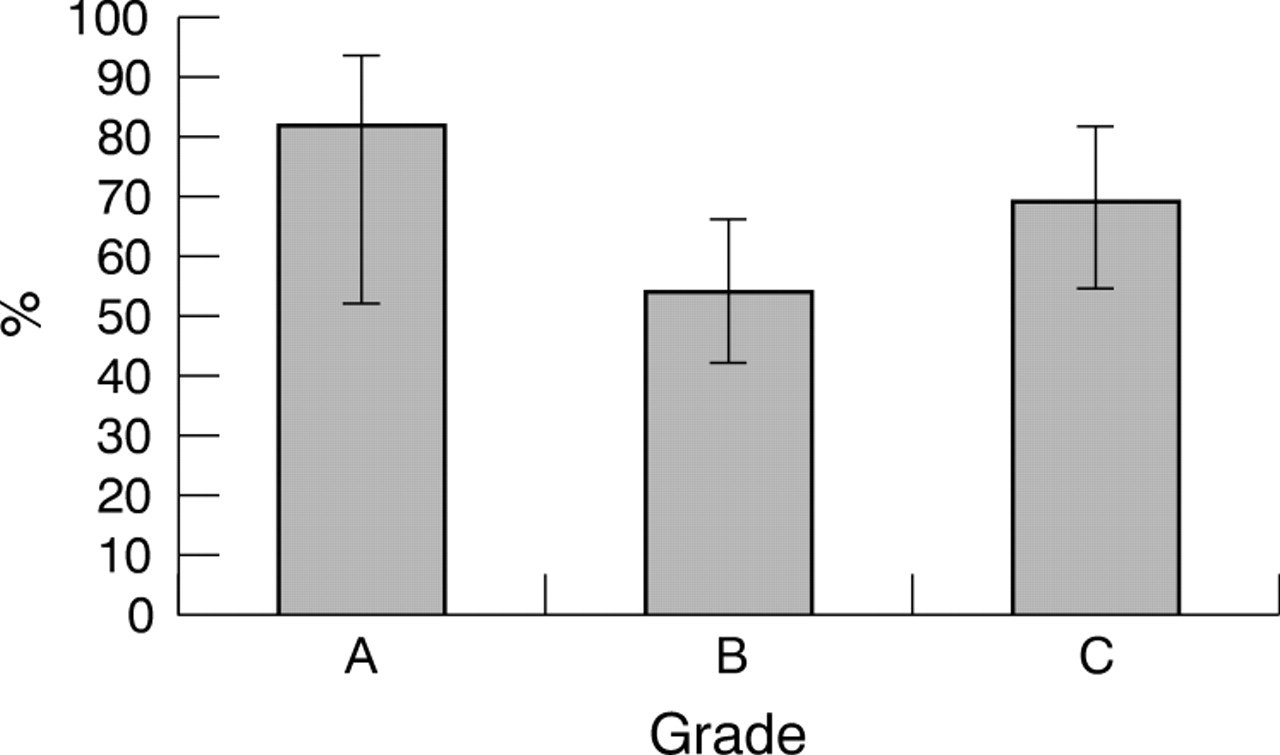
The overall rate of success was 62% (63/101) (95% CI 53% to 71%). The success rate for grade A was 82% (95% CI 52% to 95%), for grade B 54% (95% CI 41% to 66%), and for grade C 69% (95% CI 53% to 82%) (p = 0.12) (fig 1).
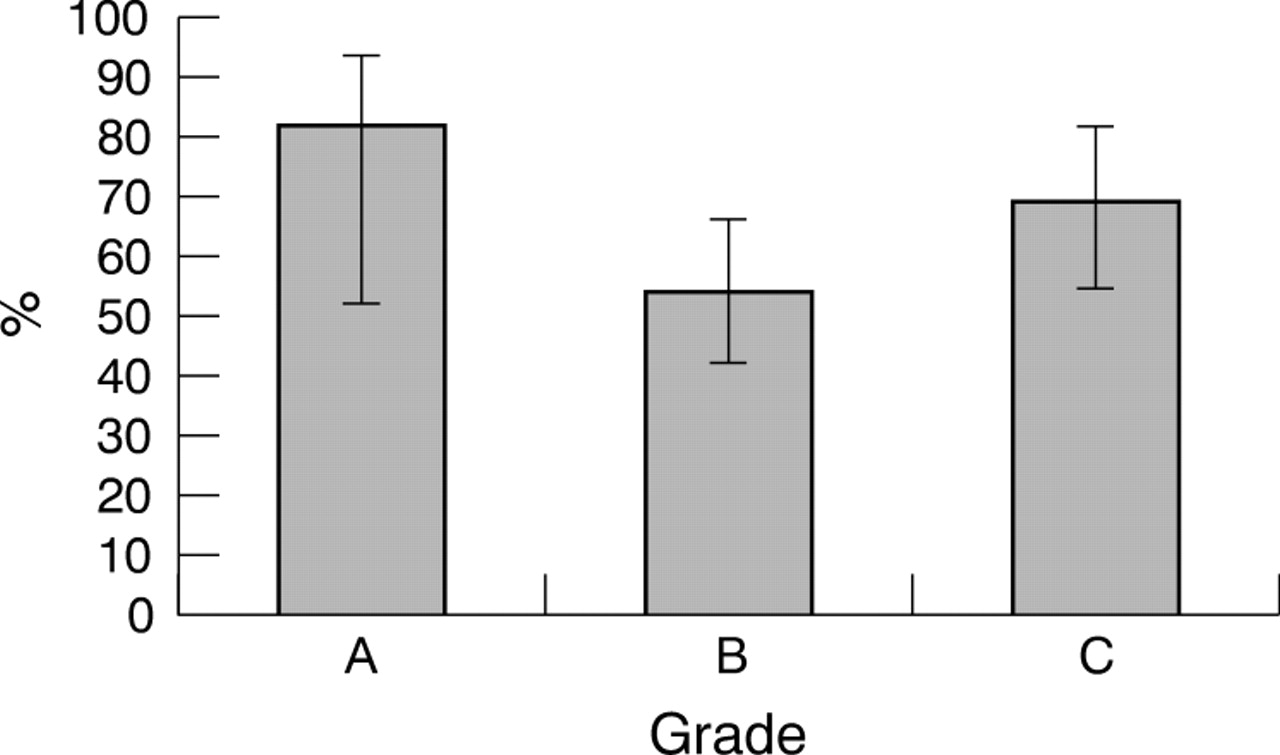
Rate of success (%) for each grade of dislocation (p = 0.12). See text for explanation of grades.
There were 6 (6%) complications: 5 were related to intravenous sedation and 1 to the attempted reduction. One patient experienced desaturation to oxygen saturation of 90% while on oxygen because of partial airway obstruction due to opiate excess. This required a simple chin lift and administration of naloxone rapidly returned the oxygen saturation to 100%. The patient made an uneventful recovery. Three patients were oversedated, resulting in a GCS <9. All of these patients had received 5 mg of morphine and 4 mg or 5 mg of midazolam. One patient also experienced transient mild hypotension requiring the trolley to be placed head down. Two were given flumazenil and all three patients recovered fully without further complications. One other patient became mildly hypotensive but this resolved without any treatment. Another patient developed a mild foot drop after the attempted reduction, which may have been present before the attempted reduction. The patient required treatment with a splint and physiotherapy.
There were no knee injuries and no femoral shaft fractures.
Secondary outcomes
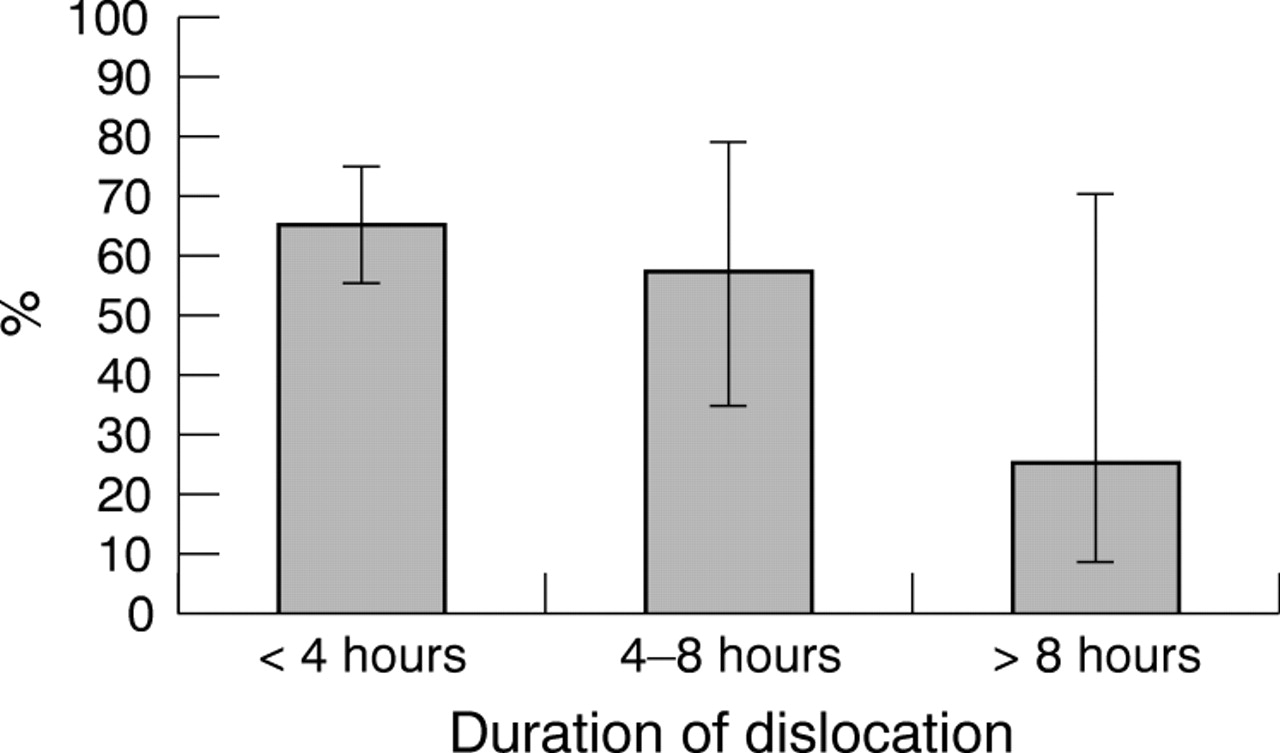
The rate of success for first dislocations was 50% (95% CI 34% to 66%) and for recurrent dislocations 69% (95% CI 57% to 79%) (p = 0.11). With regard to duration of dislocation the rate of success was 65% for <4 hours (95% CI 54% to 74%), 57% for 4–8 hours (95% CI 33% to 79%), and 25% for >8 hours (95% CI 5% to 70%) (fig 2).

{kind=link}
{kind=link}
Rate of success (%) by duration of dislocation (p = 0.27).
Other outcomes
The rates of success by grade of doctor were: senior house officer 62% (95% CI 46% to 75%) and senior doctor 63% (95% CI 51% to 74%) (p = 1.00).
We also calculated the time taken from arrival in the emergency department to attempted reduction of the joint. This was recorded in 83 patients and ranged from 0.37 hours to 5.68 hours (mean (SD) 1.83 (1.08) hours). In 47 patients, who were excluded from analysis, although not for medical reasons, the range was from 0.77 hours to 25.12 hours (mean time to induction 10.88 (6.59) hours).
DISCUSSION
Our results suggest that dislocations of the prosthetic hip can be successfully reduced using conscious sedation without serious complications. In our sample, the rate of success rates was highest in patients with grade A or recurrent dislocations, although none of the differences were statistically significant and these hypotheses would need to be tested in larger samples. Our results also show that the success rate was not dependent upon the grade of doctor performing the sedation/reduction.
One patient had a foot drop possibly due to the procedure. This is acceptable as sciatic nerve injury occurs in 10–14% of dislocated native hips due to either the initial trauma or during relocation.5 Three were oversedated with consequent deterioration in their conscious level and one partial airway obstruction secondary to opiates. Clearly this is important, as the consequences can be serious. We would stress that such patients are placed in a resuscitation area with full monitoring and all equipment to hand to manage a respiratory arrest. Our doctors are instructed to comply with the guidelines of the Royal College of Surgeons on intravenous sedation for non-anaesthetists.
Our subgroup analysis did not show significant differences in success rates between first versus recurrent dislocations, however, overall the former was more successful. The advantage of reducing the hip in the emergency department are many and include:
-
almost immediate pain relief for the patient
-
less need for continued morphine or patient-controlled analgesia devices
-
reduction in the length of time the soft tissues surrounding the joint are distorted
-
elimination of the need for a general anaesthetic and its inherent risks in elderly people.
CONCLUSION
Reduction of isolated unilateral dislocations of the prosthetic hip using conscious intravenous sedation in the emergency department is safe and has a reasonable rate of success. Reductions of prosthetic hips can be attempted more quickly using conscious sedation than awaiting general anaesthesia.
Acknowledgments
We would like to thank C Quaddy for her help with analysing the results; Professor P Thomas for the statistical analyses; Mr R Middleton for his support of the project and training the medical staff in the Allis technique, and all the staff of the Accident and Emergency Department of Poole Hospital.
AUTHORS CONTRIBUTIONS S Frymann carried out the study, collected the data, and helped write the paper. G Cumberbatch designed the study and helped write the paper. A Stearman provided the idea and the results of his study to allow statistical calculation of the sample size used.
Footnotes
-
Competing interests: none declared