Article Text

Abstract
Objective To determine the analgesic efficacy and safety of intravenous single-dose paracetamol versus morphine in patients presenting to the emergency department with renal colic.
Methods A randomised double-blind study was performed to compare the efficacy of intravenous paracetamol (1 g) and 0.1 mg/kg morphine in patients with renal colic. The efficacy of the study drugs was measured by a visual analogue scale and a verbal rating scale at baseline and after 15 and 30 min. The adverse effects and need for rescue medication (1 μg/kg intravenous fentanyl) were also recorded at the end of the study.
Results 133 patients were eligible for enrolment in the study, with 73 patients included in the final analysis (38 in the paracetamol group and 35 in the morphine group). The mean±SD age of the subjects was 30.2±8.6 years and 51 (70%) were men. The mean reduction in scores at 30 min after study drug administration was 63.7 mm (95% CI 57 to 71) for paracetamol and 56.6 mm (95% CI 48 to 65) for morphine. The difference between pain reduction scores for the two groups at 30 min was 7.1 mm (95% CI −18 to 4), demonstrating no statistical or clinical significance. Two adverse events (5.3%) were recorded in the paracetamol group and five (14.3%) in the morphine group (difference 9%, 95% CI −7% to 26%).
Conclusion Intravenous paracetamol is effective in treating patients presenting with renal colic to the emergency department.
Clinical trials registration no ClinicalTrials.gov ID number NCT01318187.
- Neurology
- statistics
- cardiac care
- ECG
Statistics from Altmetric.com
Introduction
Acute severe colicky flank pain associated with the passage of renal calculi is termed renal colic. This condition is commonly diagnosed and treated in the emergency department (ED). Renal colic is an intensely painful condition requiring rapid analgesic treatment.1 Both parenteral opioids and non-steroidal anti-inflammatory drugs (NSAIDs) are commonly used to provide relief from renal colic, and both can have adverse effects.2 Although opioids are effective and provide rapid analgesia in renal colic, hypotension, nausea, vomiting and dizziness are not uncommon after narcotic administration.
Paracetamol is commonly used as an analgesic and antipyretic and is available internationally in oral, rectal and intravenous formulations. It is well absorbed orally with an onset of action of approximately 45 min. However, if given by the intravenous route, time to onset of analgesia can be shortened to <10 min with maximum analgesia reached in just 15 min.3 This is potentially significant for severely painful conditions.
The relatively recent development of intravenous paracetamol offers the advantage of fewer adverse effects than with other NSAIDs used for acute pain relief. The efficacy of intravenous paracetamol has been studied in postoperative pain and in renal colic with favourable results.2 ,4–7
The objective of this study was to determine the analgesic efficacy and safety of intravenous single-dose paracetamol compared with intravenous morphine in patients presenting to the ED with renal colic.
Methods
Study design and setting
A single-centre prospective randomised double-blind clinical trial was performed between December 2010 and March 2011 in a tertiary care hospital ED with an annual census of approximately 37 000 visits. The efficacy of intravenous paracetamol and intravenous morphine was compared for reducing pain in patients presenting with renal colic.
Selection of participants
Patients aged 18–55 years with flank pain were potentially eligible for the study. Individuals were enrolled consecutively 24 h a day, 7 days a week, if they had a clinical diagnosis of acute renal colic and complained of moderate to severe pain according to the 4-point verbal scale. Patients were excluded if they refused to give informed consent; used any analgesics within 6 h of their ED visit; presented with fever or were haemodynamically unstable; had signs of peritoneal irritation or cardiac failure; had a history of renal failure, hepatic failure or a prior known allergy to paracetamol or morphine; were pregnant or suspected of being pregnant; and had known vision problems. Patients thought to have renal colic but ultimately diagnosed with a renal abscess, renal infarction or renal vein thrombosis were also excluded from the study.
Although the treating physicians varied, the senior resident on shift who was familiar with the protocol was consulted to decide patient eligibility. The ultimate diagnosis of renal colic was confirmed using ultrasonography or CT to identify the stone. Ultrasonography was the first choice for detecting a renal stone, and CT was performed if a stone was not detected by ultrasonography. After CT, patients not having urolithiasis or found to have pathologies other than renal colic were excluded from the study.
Interventions
Study subjects were randomised to receive a single intravenous dose of either paracetamol (Perfalgan, Bristol Myers Squibb, Itxassou, France; 1 g in 100 ml normal saline) or morphine (0.1 mg/kg in 100 ml normal saline) in a blinded fashion. Both drugs were given as a bolus infusion within 2–4 min. The identities of the study drugs were recorded in a document, folded four times and then covered for allocation concealment. When a patient was enrolled in the trial, a study nurse retrieved one of the drugs from a box. The medication was prepared by the study nurse and administered by the second nurse who was blinded to the purpose of the investigation. Because the study drugs were identical in colour and appearance, the treating physicians and patients were also blinded to their identity. Subjects who required rescue analgesia due to inadequate pain relief received fentanyl 1 μg/kg intravenously.
Methods of measurements
Subjects reported pain intensity on both a 100 mm visual analogue scale (VAS; ranging from ‘no pain’ at one end to ‘the worst pain’ at the other end) and a 4-point verbal rating scale (VRS; no pain, mild, moderate or severe pain) just before drug administration and at 15 min and at 30 min after the study drug was given.8 ,9 The demographic features of the subjects and adverse effects (nausea, vomiting, dizziness, vertigo, headache, hypotension, altered mental status, allergic reaction, itching, urinary retention, thoracic rigidity, respiratory depression and dry mouth) were recorded.
Outcome measures
The primary outcome measure was pain reduction documented on the VAS at 15 and 30 min after medication administration. Secondary outcome measures were changes in the VRS at 15 and 30 min, the need for rescue analgesia and the presence of any adverse event.
Primary data analysis
The study was planned as a superiority trial. The study data were analysed by MedCalc software 11.0.4. Continuous variables were expressed as means (SD), ordinal variables as medians (IQR) and categorical variables as rates. Normality analysis was performed using the Kolmogorov–Smirnov test and the variables were represented as means or medians accordingly. If a difference of 20 mm in VAS is accepted as clinically significant and the SD is accepted as 25 mm, then 33 patients were needed in each group to achieve a power of 90%. The differences in VAS scores between time intervals within each study drug group and between the two groups, together with statistical significance, were expressed by 95% CIs. All tests of significance were two-sided.
Althugh we planned to perform intention-to-treat analysis, the VAS scores of four patients were not measured due to intractable pain and vomiting. We therefore performed a sensitivity analysis to establish an intention-to-treat analysis by assigning the maximum and minimum VAS reductions at 30 min in the dataset of these four patients and recalculated the mean VAS reductions.
Results
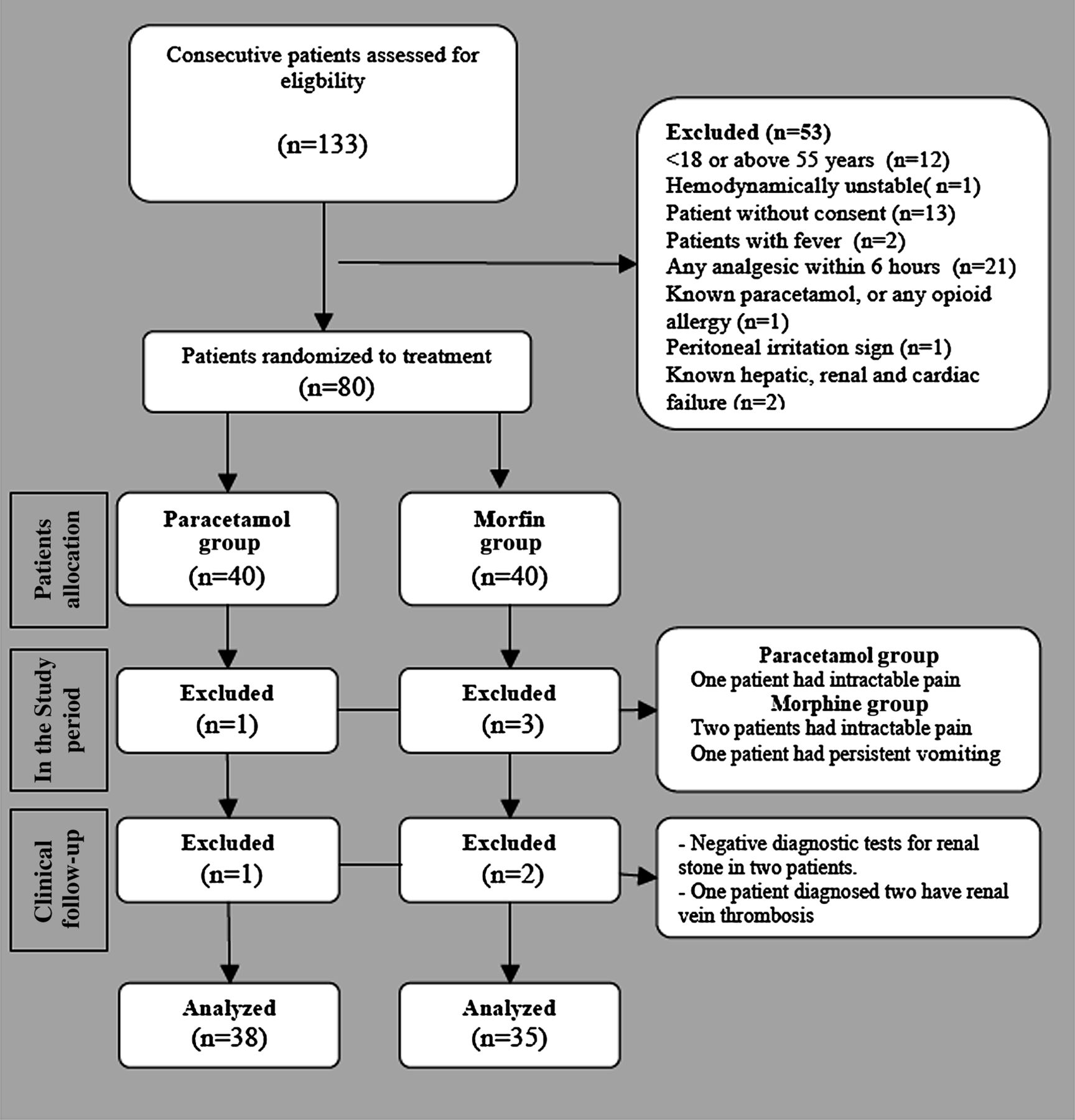
One hundred and thirty-three patients were initially evaluated for study enrolment. Fifty-three patients were excluded for the reasons shown in figure 1, leaving 80 patients who agreed to participate. Seven of these patients were ultimately excluded (three with intractable pain, one with persistent vomiting, two with failure to detect a stone and one diagnosed with renal vein thrombosis). This resulted in 73 patients who completed the study, 38 in the paracetamol group and 35 in the morphine group.
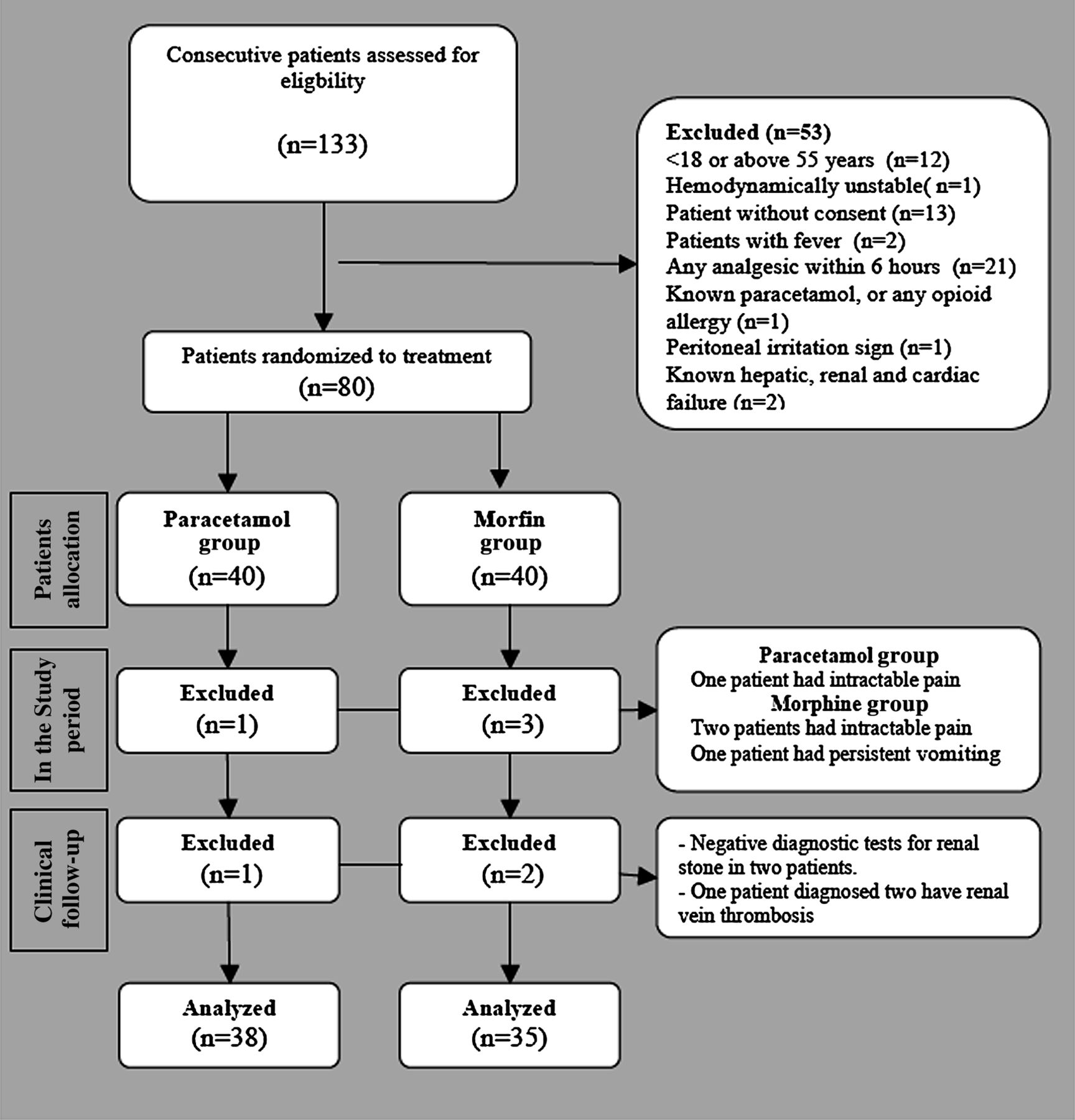
Patient flow chart.
The study subjects had a mean age of 30.2±8.6 years and 51 (70%) were men. The demographic features of the study subjects are shown in table 1. The mean reduction in VAS pain intensity score at 15 min was 33.8 mm (95% CI 26 to 41) for paracetamol and 39.4 mm (95% CI 30 to 49) for morphine. The mean reduction at 30 min was 63.7 mm (95% CI 57 to 71) for paracetamol and 56.6 mm (95% CI 48 to 65) for morphine (figure 2). The difference in pain reduction scores at 30 min between the two groups was 7.1 mm (95% CI −18 to 4). Pain reduction as recorded by the VRS at 30 min was similar to the VAS scores (tables 2 and 3).
Baseline characteristics

{kind=link}
{kind=link}
Reduction in mean visual analogue scale (VAS) scores.
Pain outcome measures (mm)
Reduction in pain scores and differences between groups at 15 and 30 min time intervals
There were two adverse events (5.3%) in the paracetamol group and five (14.3%) in the morphine group (difference 9%, 95% CI −7% to 26%; table 4). Thirteen patients required rescue analgesia, six (15.8%) in the paracetamol group and seven (20%) in the morphine group (difference 4.2%, 95% CI −15% to 24%).
Adverse effects
The sensitivity analysis performed to determine the effects of four patients excluded during the study period revealed a score of 62.3 mm (when the excluded patient assigned minimum VAS reduction) and 64.6 mm (when the excluded patient assigned maximum VAS reduction) for the paracetamol group and 52.5 mm (when three excluded patients assigned minimum VAS reduction) and 59.6 mm (when three excluded patient assigned maximum VAS reduction) for the morphine group.
Discussion
Pain management is one of the most important concepts in emergency care.10 The ideal analgesic treatment should provide rapid and effective pain relief, have a low incidence of adverse effects and no significant interaction with other pharmacological agents.4 Ketorolac and opioids are the most prescribed medication for renal colic by emergency physicians in the USA.11 Both NSAIDs and opioids are effective in treating renal colic. However, a Cochrane meta-analysis showed that NSAIDs are more effective than opioids in reducing the pain from renal calculi and are associated with fewer side effects when patients were assessed 30 min after drug administration.12
Intravenous paracetamol is a safe and effective drug for acute pain management, although its mechanism of action is still controversial. Some of the theories explaining the efficacy of intravenous paracetamol include inhibition of cyclo-oxygenase isoenzymes, interaction with the endogenous opioid pathway, activation of the serotonergic bulbospinal pathway, involvement of the nitric oxide pathway and an increase in cannabinoid/vanilloid tone.13 Regardless of the mechanism of action, intravenous paracetamol has been studied in many types of pain and found to be as effective as opioids. These studies were performed mostly on patients with postoperative pain following orthopaedic, cardiac and dental surgery.4–7 ,14 ,15 Although intravenous paracetamol has been available for more than 20 years in many European countries, it has not been used commonly in clinical practice until recently.10
In addition to investigations in postoperative pain, studies have also been conducted of the effectiveness of intravenous paracetamol in different types of pain in the ED.2 ,10 Craig et al reported no difference between intravenous paracetamol (1 g) and intravenous morphine (10 mg) in acute limb pain at 15, 30, 45 and 60 min. In addition, patients in the paracetamol group experienced fewer side effects.10
Renal colic is one of the most important causes of pain requiring immediate intervention in patients presenting to the ED. Intravenous paracetamol may be a suitable alternative for treating renal colic. It appears to have a rapid onset of action and fewer side effects than NSAIDs and opioids. A double-blind randomised placebo controlled study by Bektas et al compared the effectiveness of intravenous paracetamol and intravenous morphine in patients presenting with renal colic to the ED.2 Both drugs were more effective than placebo in reducing renal colic at both 15 and 30 min. Although changes in VAS from baseline were similar at 30 min for paracetamol and morphine (median 41.5 mm and 43 mm, respectively), intravenous paracetamol had a more pronounced effect than morphine at 15 min (median change in VAS from baseline 44.5 mm and 30 mm, respectively). In addition, fewer side effects were reported in the paracetamol group than in the morphine group (24% vs 33%).
A study by Grissa et al compared intravenous paracetamol and intramuscular piroxicam but did not use a double-blind methodology. They reported better pain relief with intravenous paracetamol. Their results showed a 50% decrease in the VAS score from baseline at 90 min with paracetamol (80% vs 48%). Only one side effect occurred in each group (rash in the piroxicam group and vomiting in the paracetamol group).16
The present study shows that both intravenous paracetamol and intravenous morphine are similarly effective in reducing renal colic at 15 min and 30 min. In contrast to the study by Bektas et al,2 paracetamol was not better than morphine at 15 min. Paracetamol was also found to have fewer side effects than morphine in our study.
Intravenous paracetamol was well tolerated in clinical trials, having an adverse effects profile similar to placebo. Additionally, rates of adverse reactions associated with the use of intravenous paracetamol are extremely low (<1/10 000).17 In our study, nausea and vomiting were the only adverse effects seen in the paracetamol group (5.3%), which is similar to results reported in other studies.2 ,4 ,7 Bektas et al reported a higher incidence of nausea and vomiting (15%), but Grissa et al reported vomiting in only one patient (2%).2 ,16
Opioids such as morphine may be associated with respiratory depression, excessive sedation, biliary spasm, depression of gastrointestinal motility, nausea and vomiting, and confusion, particularly in older patients.5 In the present study, patients in the morphine group had more adverse events than those in the paracetamol group (15.3% vs 5.3%). This is similar to the findings of Bektas et al (33% vs 24%).2
Study limitations
Given this study was planned as a superiority trial, a larger sample size would be needed to conclude that intravenous paracetamol and morphine are equally effective in relieving the pain of renala colic (an equivalence trial). Although we planned an intention-to-treat analysis, one patient in the paracetamol group and two in the morphine group were excluded from the study because of intractable pain, and one patient was also excluded from the morphine group because of persistent vomiting. Because we thought that early reduction of pain in renal colic is important, we measured the VAS at 15 and 30 min only. Pain relief after 30 min was not measured but might be of interest for future investigation. Some adverse events such as nausea and vomiting may be due to the renal colic rather than study drugs. The number used to calculate the dose for morphine administration was obtained from patients asked to estimate their own weight.
Conclusion
We conclude that intravenous paracetamol may be a safe and effective alternative to morphine for the treatment of renal colic in the ED.
References
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by the local ethics committee.
Provenance and peer review Not commissioned; internally peer reviewed.
Linked Articles
- Primary survey