Article Text

Abstract
Introduction While the benefits of regional analgesia (RA) for preoperative pain relief in hip fracture (HF) in elderly patients are well recognised, this service is yet to be established in many UK emergency departments (EDs). We set out to discover how widely RA is adopted in the UK EDs.
Methods In April–July 2010, we conducted a postal survey of 218 UK EDs, followed up with fax reminders for non-respondents.
Results A total of 147/218 (67%) EDs completed the survey. Sixty five (44%) respondents reported use of RA blocks for HF. The commonest stated reasons for not using RA were lack of trained staff (36%) or appropriate equipment (22%). RA users practiced femoral nerve block most widely (60% of EDs) followed by fascia iliaca compartment block (FICB) (22%).
Discussion It is more a lack of trained staff and suitable equipment that prevents RA blocks being widely adopted in the UK. We advocate FICB in HF patients, which is an easy landmark-based block that can be safely performed by ED doctors. Our survey initiated multidisciplinary consultation and development of a protocol for preoperative FICB in HFs in our teaching hospital ED.
Conclusions RA for HFs is not widely used in UK EDs, proving that there is room for improvement .The finding that RA blocks are performed by the ED medical staff in 84% of the responding EDs practising RA was reassuring for developing the service in our hospital. FICB should be considered as an alternative to parenteral analgesia in adult patients with HF.
- analgesia/pain control
- fractures and dislocations
- emergency department management
Statistics from Altmetric.com
Introduction
Fracture of the neck of femur (or hip fracture, HF) is the most common serious injury in the elderly, and UK annual incidence is around 76 000.1 The establishment of the National Hip Fracture Database in 2007 reflected a renewed focus on improving the care of UK HF patients, and the National Institute of Health and Clinical Excellence has recently published its guideline on the management of adult HF.2 ,3 Emergency Departments (EDs) are usually the first port of call for HF patients and are important players in achieving the ultimate goal of excellence in clinical care.
Part of good clinical care is to provide adequate analgesia for patients in pain.4 ED Quality Indicators in the NHS National Outcomes Framework 2013–2014 include patient experience of ED services. Patient experience of the service will be significantly improved with timely, effective and safe analgesia.5 The severe pain that often results from a HF means that clinicians commonly administer parenteral opioids as first-line analgesia.3 These patients, however, are often elderly and frail, thus rendering them more susceptible to the adverse effects of opioid medication, such as delirium, sedation and respiratory depression.6 An alternative method of analgesia for these patients that avoids the aforementioned opioid side effects and can be easily and cost-effectively administered by ED staff could provide a positive contribution to improving their clinical care. Regional analgesia (RA) techniques are frequently used by anaesthetists prior to surgery on the lower extremity, and varieties of techniques aiming to achieve femoral nerve block are used by emergency physicians in the treatment of femoral neck or shaft fracture.7
The results of our initial informal local survey of the Oxford region, which we conducted when we considered implementing RA service for HF in our hospital, were not encouraging. None of the hospitals in the Oxford region offered this service. It was considered to be an expensive modality requiring additional equipment, that is, ultrasound and/or peripheral nerve stimulator (PNS) and complex training for the ED staff. To facilitate the development of this service in our teaching hospital with approximately 500 HF admissions per year, we set out to discover how widely RA is adopted in the UK EDs. If they are using RA, then which techniques are used, how they are applied and who performs them and the level of satisfaction in those EDs who practice RA for HF. Where RA is not used, what were the reasons for not using it.
Method
A postal survey of 218 UK EDs was conducted in April–July 2010. A list of contact addresses (last updated in 2009) was obtained from the College of Emergency Medicine and a search of the NHS Choices website confirmed, which trusts still had fully functioning EDs.8 ,9 The formal questionnaire (figure 1) was addressed to the ED Clinical Director. A stamped, addressed envelope was enclosed to encourage a response. The initial mailshot was followed by three rounds of faxed reminders for those EDs that had not responded by the end of May. To facilitate completion process, the ‘box ticking’ method was used and in some questions more than one box could be ticked.
Survey questionnaire.
Results
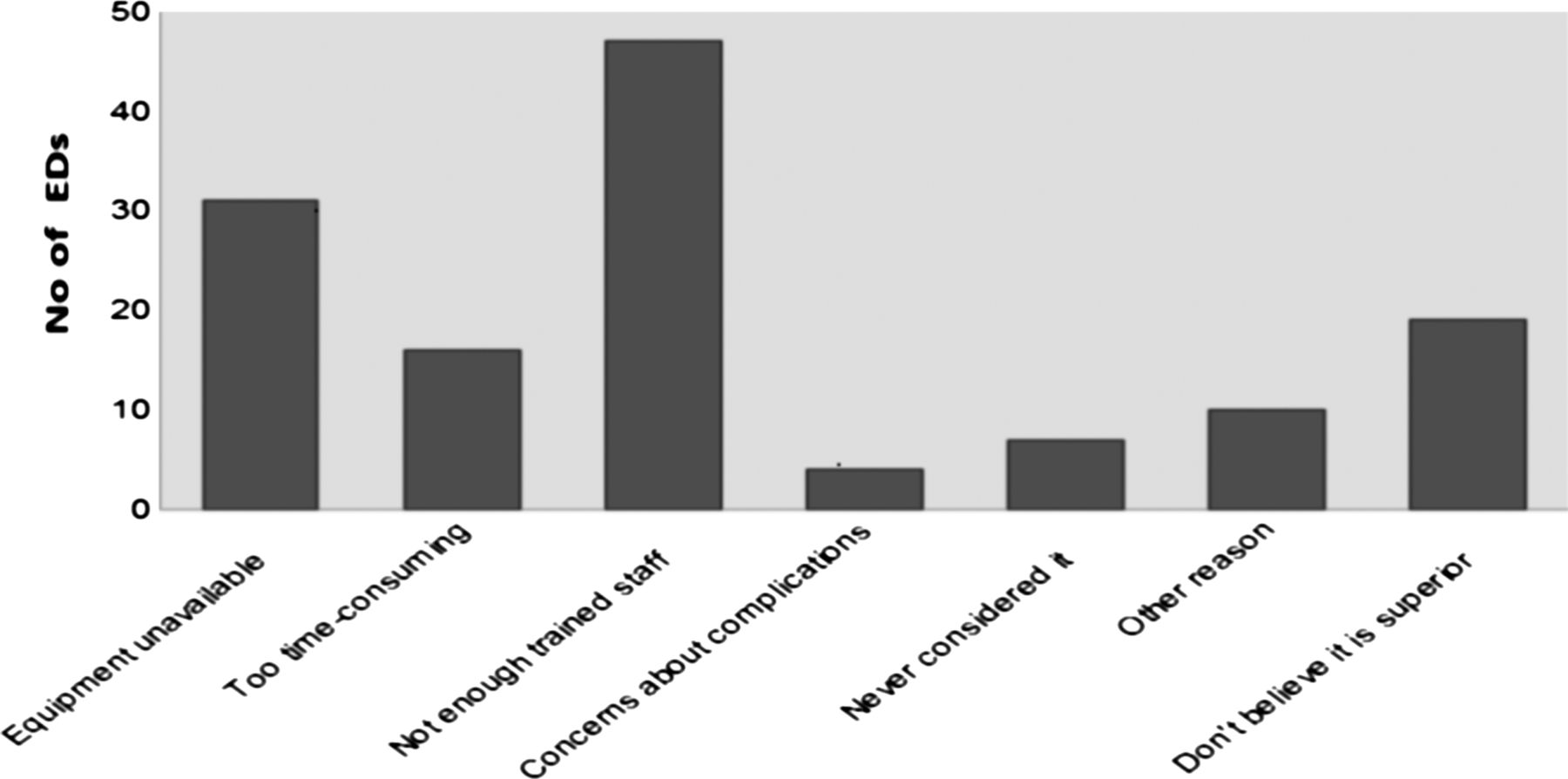
A total of 147 out of 218 (67%) EDs completed the survey. Sixty five of 147 (44%) of the respondents reported using RA blocks for HF. The commonest stated reasons for not using RA were lack of trained staff (36%) or appropriate equipment (22%) (figure 2). In 64/65 EDs providing the service, RA blocks were performed by ED doctors. In seven, EDs’ anaesthetists, and in four, non-physicians, also performed the blocks. RA users practiced femoral nerve block in 60% of EDs providing the service, fascia iliaca compartment block (FICB)—22%, both in 12%, ‘3-in-1’ block in 6%. The landmark technique was the most popular, used in 43/65 (66%) EDs; landmark ± PNS was used in another 7 EDs (11%); ultrasound ± PNS in 28 EDs (43%). Lignocaine and/or bupivacaine were/was used in 38/65 EDs providing the service, bupivacaine in 20/65 and levobupivacaine in 7/65. Hundred per cent of current RA users replied that they intended to continue using RA for the foreseeable future.

Reasons for not offering regional analgesia. EDs, emergency departments.
Discussion
Out of the 67% EDs that responded, only 44% were using RA for HF. The response rate (67%) to the survey makes it difficult to generalise the results. But, even if we assume that all non-responders were using RA, it will still be only 62% (136/218) of the EDs providing RA. If we assume the worst that the EDs did not respond because they were not providing RA, the picture will be very bleak. Our survey indicates that RA techniques are not widely used in UK EDs despite good evidence that RA can provide good pain relief and reduce opioid use in often frail, elderly patients. It is more a lack of trained staff and suitable equipment that prevents such techniques being adopted, than a fear of complications or lack of efficacy of RA techniques (figure 2).
In the authors’ opinion, the simplest regional analgesic block in ED setting is the FICB. This block, originally described by Dalens in 1989, involves localisation of the fascia iliaca compartment using a combination of anatomical landmarks and tactile feedback through the needle.10 Local anaesthetic is then injected into the compartment, hoping to block the femoral and obturator nerves, and the lateral cutaneous nerve of the thigh. While blocking the lateral cutaneous nerve of thigh is not important for preoperative analgesia, blocking the femoral nerve and obturator nerve will provide analgesia by blocking part of the sensory supply from the femoral neck as well as by reducing the muscle spasm in the quadriceps and adductor muscles.
Though nociception from fracture of the femoral neck is mediated by sciatic, obturator and femoral nerves, it is accepted that the femoral nerve block alone is efficacious in providing good analgesia; however, it requires infiltration of local anaesthetic in close proximity to the femoral nerve and adjacent vessels, and therefore, the use of either ultrasound guidance ± a PNS is advocated for optimum efficacy and patient safety. Using the PNS will stimulate the muscles and will be uncomfortable for the patient as this will result in movement of the fracture site.11–15 The FICB, conversely, does not require a needle to be brought close to the femoral nerve and vessels, and therefore, seems to represent a much simpler and possibly safer technique requiring only a needle and syringe for administration of local anaesthetic. The available literature on the use of peripheral nerve blocks in HF suggests that, FICB is a simple technique, which is easy to learn and which provides a superior level of analgesia with a more favourable side effect profile when compared with parenteral opioid analgesia.16–24 FICB has also been shown to reduce the incidence of delirium in these patients. FICB is likely to be well suited to a busy ED, as it does not require additional specialist equipment, and mastery of the technique does not require a great deal of training. Its simplicity and associated low cost also make it a more attractive prospect in the current economic recession.
Our survey initiated multidisciplinary consultation and the development of a protocol (figure 3) for providing preoperative FICB in HF in our hospital ED. A ‘Hip Block Box’ was developed to standardise equipment and local anaesthetic usage. The FICB protocol was implemented following a period of training and competency attainment among senior ED doctors. Further staffing improvements have led to the appointment of a Trauma Nurse Consultant who will be, in addition to the senior ED doctors, using the FICB as part of their treatment modalities. Registered nurses without anaesthetic background have been performing FICB after receiving sufficient training to successfully provide pain relief for HF in other UK hospitals.21 The Association of Anaesthetists of Great Britain and Ireland in its recent position statement has agreed that FICB can be considered as a ‘local anaesthetic’ and not a ‘regional anaesthetic’ technique, because when the correct technique is used, the needle trajectory is not likely to encroach on nerve trunks or major blood vessels.25 They also agree that non-medically trained registered health professionals can perform FICB if they have been appropriately trained and are following agreed clinical governance procedures.

{kind=link}
{kind=link}
{kind=link}
Emergency department fascia iliaca compartment block protocol.
Conclusion
The reported limited use of RA in EDs in the UK necessitates improvement. Our survey finding that RA blocks are performed by the ED medical staff in majority of EDs practicing RA was reassuring for developing the service in our teaching hospital. FICB should be considered as an alternative (or adjunct) to parenteral analgesia in adult patients with HF. When introducing the new service, strict safeguards such as a protocol, a ‘Hip Block Box’ and auditing are highly advisable to ensure sustainability of the new service. Medical staff in the EDs should be instructed on the safe and effective administration of FICB, thus ensuring that eventually most (if not all) ED doctors are capable of performing the blocks appropriately and safely.
References
Footnotes
-
Contributors AR, EB and SG conceived the survey and designed the questionnaire. EB collected and analysed the data with support from all the authors. EB and LF designed the FICB protocol. All authors revised and edited the paper. All authors had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. AR is guarantor.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.