Article Text

Abstract
Objective Glomerular filtration rate (GFR) is part of routine medical practice for clinical assessment of kidney function in health and disease conditions, and is determined by measuring the clearance of creatinine (Cl-Crn) or estimated (eGFR) from equations using serum creatinine (Crn) or cystatin C (Cyst C). Crn and Cyst C methods obviate the need for urine collection but their reliability under non-resting conditions is uncertain. This study compared GFR determined by Cl-Crn, Crn and Cyst C methods under the conditions of rest and after exercise.
Methods Twelve young male subjects performed a 30 min treadmill exercise at 80% of the maximal oxygen capacity. Venous blood samples and urine collections were collected before and after exercise and after recovery period. GFR rates were calculated from serum Crn and Cyst C equations, and Cl-Crn measured from serum and urine Crn output. Albumin was also determined for all samples.
Results Under resting conditions, eGFR from Crn and Cyst C did not differ from Cl-Crn (p=0.39). Immediately after exercise, GFR decreased significantly, regardless of the method, but more so for Cl-Crn (−30.0%; p<0.05) compared with Crn (−18.2%) and Cyst C (−19.8%). After the recovery period, GFR determined by Cl-Crn was returned to initial values whereas Crn and Cyst C remained reduced. Although eGFR methods accurately estimate GFR at rest, those methods underestimated the change in GFR after acute exercise.
Conclusions These results indicate that exercise-induced changes in GFR should be determined by Cl-Crn method.
Statistics from Altmetric.com
Introduction
The evaluation of healthy kidney function is determined by the measurement of glomerular filtration rate (GFR) and the urine excretion of proteins (mainly serum albumin). Clinically, chronic kidney disease (CKD) is defined by the presence of functional abnormalities such as a reduced GFR and the presence of serum albumin in urine by the National Kidney Foundation.1 The measurement of endogenous creatinine clearance (Cl-Crn) using timed urine collections is regarded as an accurate estimation of GFR. However, complete urine collection is more difficult with ambulatory patients and/or during conditions involving exercise. Therefore, several researchers have used an estimated GFR (eGFR) based upon serum creatinine (Crn) measurement without the need for urine collection.2 ,3
The eGFR from serum Crn values is part of routine medical practice for clinical assessment of kidney function. Calculation of eGFR has been supported by ‘gold standard’ methods, such as inulin, iodothalamate, isotopes (51Cr-EDTA, 99Tc-DTPA) in humans at rest.2 ,4 Several publications showed that, under resting conditions, the different formulae to predict Crn clearance need to be corrected for age, sex, race and body size.5,–,7 A few years ago, the National Kidney Foundation concluded that serum Crn should not be used as the sole means to assess the level of renal function.8 Recently, a group of scientists developed a new evaluated equation (CKD-EPI) to accurately validate eGFR for routine clinical purpose.7 In addition, the use of enzymatic sensor for serum Crn improves the validity of Crn measurements.9
Over the last decade, cystatin C (Cyst C) has received particular attention and has appeared to be a promising alternative to serum Crn to evaluate GFR.1 ,2 ,10 ,11 Cyst C is a non-glycated basic protein with a low molecular weight (13.3 kDa) that is freely filtered by the glomerular membrane, reabsorbed and catabolised in the proximal tubule, with no tubular secretion and minimal extrarenal elimination.12 Its validity as a marker of eGFR in healthy adults has been validated by several publications.10 ,11 ,13 Moreover, a few publications emphasise the combination of serum Crn and Cyst C equations to better predict GFR.14 ,15 In addition, Stevens and Levey proposed standard urine Cl-Crn as a confirmatory test for eGFR.4
In previous studies, we showed that in healthy subjects strenuous exercise had a major effect on kidney function, namely reducing GFR and enhancing albumin excretion rate.16,–,19 We emphasised the importance to accurately evaluate GFR in exercising healthy individuals using both Crn serum concentration and urine Crn output,17 from children20 to seniors.16 Also, we stressed the importance of GFR evaluation in diabetic patients,17 ,21 heart and kidney transplant recipients22,–,24 involved in exercise training sessions. Indeed, strenuous exercise induces haemoconcentration, while reducing urine output and postexercise return to basal state is related to a half-time decline of about 1 h.25 A few publications did apply the eGFR technique in resting athletes using either Crn22 ,26 ,27 or Cyst C28 serum markers. However, Hostetter et al pointed out concerns pertaining to the validity of using eGFR under certain non-steady state conditions, such as rapidly changing GFR.29 As acute intense exercise involves dynamic changes in GFR, the use of eGFR from serum markers during exercise may not accurately reflect the change in this important renal parameter. The validity of using eGFR to measure GFR during acute exercise has not been assessed.
The purpose of the present study was to compare the estimated methods of GFR, using equations of serum Crn and Cyst C, with traditional clearance methodology based upon the measurement of serum Crn and urine Crn excretion in healthy individuals during strenuous acute exercise.
Materials and methods
Study population
Twelve white, young, male physical educators (mean±SE; age: 25±5 y; weight: 76.5±2.0 kg; height: 1.82±0.02 m; body mass index: 23.1±0.7 kg.m−2; body surface area (BSA): 1.98±0.03 m2) were enrolled in this study. All subjects had no signs of abnormal kidney function. The informed written consent of the subjects was recorded after full explanation of the whole investigation. This study was approved by the Medical Ethical Committee of the Academic Hospital and the conduct of this project was in accordance with the guidelines of the declaration of Helsinki of 1975 as revised in 1976.
Exercise protocol
Before the analysis of renal function, the subjects were first tested on a treadmill for the determination of their maximal oxygen consumption (VO2 peak) by stepwise increase of speed (2 km/h) every 1 min, starting at 6 km/h, until stable oxygen consumption with usual criteria (RQ, ventilation and heart rate) were achieved. Pulse rate was recorded throughout the exercise protocol. After 1 or 2 days, the subjects came back to the laboratory on the morning after having voided their bladder about 2 h before the test (figure 1).

Experimental protocol for blood and urine sample collections, and water intake. Alb, albuin; Crn, creatinine; Cyst C, cystatine C.
They noted precisely the time of voiding. Before starting the exercise protocol, the subjects emptied their bladder and total urine volume was measured. A venous blood sample was taken from the forearm and the subjects drank 250 ml of plain water. According to previous experiments and publications, we applied a constant 80% of maximal intensity during a medium time of 30 min to induce an optimal postexercise proteinuria and reduction of GFR.25 ,30,31,32 The exercise workload on treadmill was adjusted in order to reach 80% of the VO2 peak within 5 min. The required treadmill speed was maintained for another 25 min and during this period, a steady state heart rate was obtained. At the end of the 30 min run, the speed was reduced to walking within 1 min and a second blood sample was collected. Immediately after the exercise, the subjects were given 250 ml of plain water while maintaining a seated posture at rest. Thirty minutes after stopping the exercise, the third blood sample was collected and the bladder was completely voided. The third urine collection was obtained 60 min after stopping the exercise. The blood and urine samples collected before exercise were used for Rest analysis. The blood and urine samples collected immediately and 30 min after exercise, respectively, were used for postexercise analysis. Finally, the blood and urine samples collected 30 and 60 min after exercise, respectively, were used for recovery analysis (figure 1).
Biochemical analyses
All measurements were performed on the Roche Modular Analytics P automated clinical chemistry analyser from Roche Diagnostics (COBAS) using commercially available methods from the same company (Roche Diagnostics, Mannheim, Germany). Briefly, this analyser measured Crn using a rate-blanked Crn/Jaffé compensated kinetic method, Cyst C with a particle enhanced immunoturbidimetric method, serum albumin with a bromocresol green dye binding method. The interassay coefficients of variation for the measurements of all components were under 3%.
Estimated GFR calculations
Different equations have been used to estimate GFR (eGFR) based on serum Crn1–,4 ,6 ,7 or serum Cyst C determination.2 ,11 Most of these eGFR have been validated by comparison with, ‘gold standard’ techniques, such as inulin, iodothalamate, ioexhol and 51Cr-EDTA. Thus, we decided to apply the new serum Crn equation developed by Levey et al7 named the CKD-EPI equation, whose values appeared closer to our measured Crn results (see below). Moreover, for the same reason, we choose the Grubb et al14 ,33 to estimate GFR by serum Cyst C equation:
CKD-EPI equation for eGFR (ml/min): 175×serum Crn (mg/100 ml)−1.154×age (years)−0.203.
Grubb equation for eGFR (ml/min): 89.12×Cyst C (mg/l)−1.675.
Crn GFR determination
The Crn GFR was determined using the usual definition of kidney clearance, namely urine concentration/serum concentration ratio multiplied by the urine output, for the three appropriate blood and urine samples.
Statistical analyses
Before comparing each dependent variable, the normality of the data was confirmed with the Kolmogorov–Smirnov test. The serum values of Crn, Cyst C and albumin before (rest) and after exercise (postexercise) and following the recovery period (recovery) were compared by one-way analysis of variance (ANOVA) with repeated measures (time). Changes in GFR determined by Cl-Crn, Crn and Cyst C at rest, postexercise and recovery periods were compared by a two-way ANOVA with repeated measures (method×time). When a significant main effect was found with an ANOVA, Tukey post hoc test was used to identify the significant differences among the selected means. The Bland–Altman statistical method was applied to assess the level of agreement between two measurement methods (serum Cyst C vs Crn clearance; serum Crn vs Crn clearance).34 The level of statistical significance was set at p≤0.05 for all comparisons. Values are expressed by mean±SD in the text and table 1, and as mean±SEM in figure 2.
Data obtained at rest and after exercise on serum and urine samples (mean±SD)
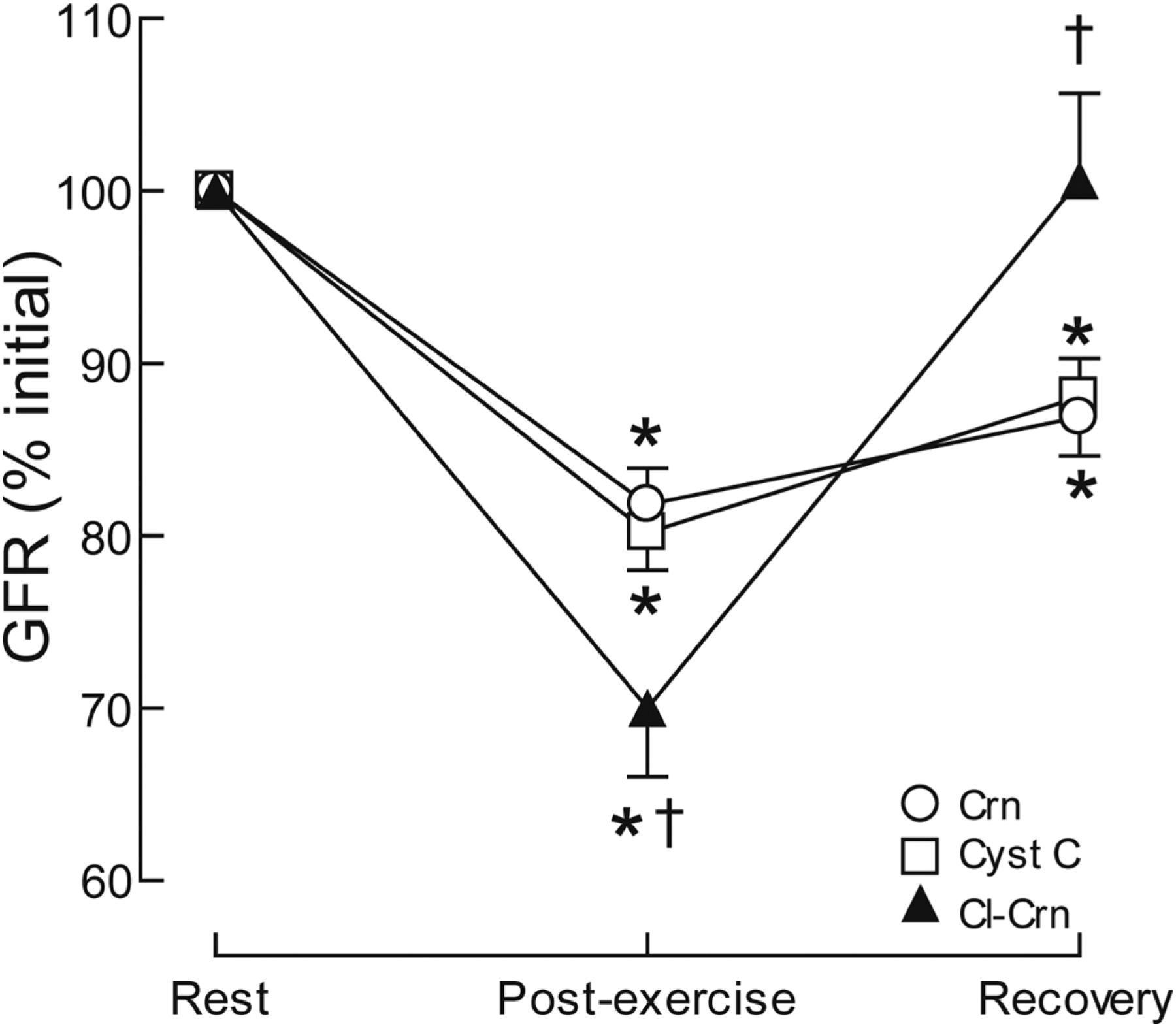
Figure 2 Changes (expressed as % rest) in glomerular filtration rate estimated by serum values of creatinine (Crn; open circles) and cystatin C (Cyst C; open squares), and Crn clearance measured from serum and urine Crn output (Cl-Crn; filled triangles) at the end of exercise period (postexercise) and after recovery. *Significant differences with initial values (p<0.05). †Significant differences with Crn and Cyst C (p<0.05).
Results
The serum values of Crn, Cyst C and albumin obtained at rest and after exercise are included in table 1. The immediate postexercise values increased by 18%, 13% and 4.8% for Crn, Cyst C and albumin levels, respectively, as compared with rest (p values<0.05). Moreover, serum values of Crn and Cyst C remained elevated after recovery (p values<0.05). The urine output was significantly reduced by exercise conditions (table 1).
At rest, the mean values of GFR obtained from Cl-Crn, Crn and Cyst C methods were 126.6±20.8, 119.6±15.8 and 118.8±15.1 ml/min, respectively (p=0.39), and were within the normal values for a healthy, young, male population (including the values expressed as GFR/1.73 m2).
The postexercise and recovery values of eGFR obtained from both Crn and Cyst C equations differed significantly compared with GFR measured from Cl-Crn (method×time, p<0.001; figure 2). After exercise, Cl-Crn, Crn and Cyst C were significantly reduced (Tukey, p values<0.001) but more so for Cl-Crn compared with Crn and Cyst C (Tukey, p values<0.05). In contrast, after recovery, Cl-Crn was returned to initial values (Tukey, p=0.99) whereas Crn and Cyst C were still reduced (Tukey, p values<0.008), and values from eGFR methods were significantly lower than those from Cl-Crn (Tukey, p values<0.004; figure 2).
The limits of agreement between the eGFR and Cl-Crn have been assessed by the Bland–Altman method (figure 3). At rest, both serum markers and evaluated Cl-Crn were within the limits of agreement. However, postexercise and recovery values differed statistically for Crn and Cyst C and Cl-Crn (p values<0.01), indicating an absence of agreement between eGFR and Cl-Crn methods.

{kind=link}
{kind=link}
{kind=link}
Bland–Altman statistical method to assess agreement between serum markers (Cyst C, Crn) and Cl-Crn methods before the exercise (rest), after stopping the exercise (postexercise) and recovery. Full line, mean difference between two methods; interrupted line =±2 SD difference against mean. There is good agreement under resting condition, but there are limits of agreement between difference and mean difference during exercise condition and recovery period. Thus serum markers cannot be rigorously applied to estimate glomerular filtration rate from serum values during exercise and short recovery period.
Discussion
The accurate determination of GFR during acute exercise is important not only to measure the renal haemodynamic changes with exercise in healthy, heart and kidney transplant recipients and diseased patients, but also to determine the precise filtered load of electrolytes, endocrines and/or pharmacological agents.
This study demonstrates the limitation of using estimated serum equations to assess GFR under exercise conditions in healthy individuals. Indeed, in resting condition, recent studies indicate that serum Cyst C is a better marker of GFR than serum Crn assay.10 ,11 The reliability of different formulae to predict Cl-Crn has been questioned by several authors.1 ,3 ,7 Crn remains the most frequent method used in clinical practice, but is affected by different variables (such as age, meat intake and muscle mass). Thus, Cyst C, provided as a potential replacement for serum Crn, has been proposed because it appears to be less affected by muscle mass. However, factors other than GFR affect serum Cyst C levels, such as sex and race.13 ,35 Fried and Grubb emphasised the need to evaluate GFR with simultaneous measurement of Crn and Cyst C in the general population to overcome pitfall interpretations.14 ,36
To date, no study has evaluated the use of eGFR using serum measurements of Crn and Cyst C to estimate GFR under exercise conditions. Previous investigations on eGFR using serum Crn equations have been obtained on athletes in resting condition26,–,28 ,37 ,38 or following a half-marathon race.39 We calculated eGFR from both serum Crn and Cyst C values, as compared with Cl-Crn GFR (serum and urine) obtained before and after exercise. Before exercise, our results showed expected values of GFR from both serum Crn (CKD-EPI) and Cyst (Grubb) equations, as compared with the Cl-Crn GFR obtained from serum Crn and urine output. However, in agreement with Hostetter et al indicating limitations in eGFR when rapid changes in GFR are expected,29 the present data emphasise that after exercise, a major difference exists between the real Crn clearance (−30%) and the eGFR from serum Crn and Cyst C (−19%) equations. Thus eGFR underestimated the decline in GFR associated with acute exercise. In 2009, Mingels et al37 evaluated GFR from equations using serum Cyst C and Crn levels at rest and after a marathon race. The authors observed that exercise induced a lesser increase in serum Cyst C (+33%) as compared with Crn (+53%). They emphasised that Cyst C seems to be a more reliable method to establish renal function after extensive marathon race. However, in that study, there was no real comparison using urine data which has a major impact on renal clearance under exercise condition. Moreover, eGFR methods also appeared unreliable after a 30 min period of recovery that followed exercise, underscoring serious limitations of these methods when used under non-resting conditions.
Our results (table 1, figures 2 and 3) emphasise two major conclusions: (1) at rest, one could apply a validated equation to estimate the GFR from serum Crn or Cyst C (such the CKD-EPI and Grubb equations), (2) during exercise, serum and urine Crn values should be used to evaluate GFR. While it may be difficult to obtain timed urine collections in studies involving exercise, these data suggest that this requirement is necessary to obtain accurate accurate measurements of GFR. An advantage of the collection of urine after exercise is that besides Cl-Crn, other important measures of renal function can be obtained, such as albumin and electrolyte excretion rate.17 ,23 Indeed, a recent epidemiology paper emphasised that physical activities of moderate intensity were found to be positively associated with estimated GFR in chronic disease patients.40 However, serum samples were only collected under resting conditions. In a previous publication, we reported modifications of measured Crn clearance and albumin excretion rate in a few cases of CKD patients.17 ,23 Thus, it would be more appropriate to evaluate the real level of transient reduction of measured GFR under exercise performance, particularly when the resting GFR is already under the normal range of a healthy population.
In summary, recent editorial and perspective statements on estimated GFR concluded that ‘serum Crn is still a very good measure of GFR’41 which ‘appears to be having salutary clinical effects’.29 However, the current study underscores that these ‘gold standard’ techniques originally proposed in resting conditions cannot be used after physical exercise events, and traditional clearance methodology (serum and urine measurements) should be used when assessing GFR during dynamically changing or non-steady state conditions.
Acknowledgments
The authors are indebted to Dr E J Zambraski for fruitful discussion and suggestions. The authors also thank Karim Banamor, Stéphanie Vieillevoye and Vanessa Albert for their efficient technical help during the entire protocol.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethical Medical Committee (Academic Hospital).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement This submission is an unpublished study.
-
▸ References to this paper are available online at http://bjsm.bmj.com