Article Text

Abstract
Objective: Although early thrombolysis reduces the risk of death in STEMI patients, mortality remains high. We evaluated factors predicting inpatient mortality for patients with STEMI in a “real-world” population.
Design: Analysis of the Myocardial Infarction National Audit Project (MINAP) database using multivariate logistic regression and area under the receiver operating curve analysis.
Setting: All acute hospitals in England and Wales.
Patients: 34 722 patients with STEMI from 1 January 2003 to 31 March 2005.
Results: Inpatient mortality was 10.6%. The highest odds ratios for inpatient survival were aspirin therapy given acutely and out-of-hospital thrombolysis, independently associated with a mortality risk reduction of over half. A 10-year increase in age doubled inpatient mortality risk, whereas cerebrovascular disease increased it by 1.7. The risk model comprised 14 predictors of mortality, C index = 0.82 (95% CI 0.82 to 0.83, p<0.001). A simple model comprising age, systolic blood pressure (SBP) and heart rate (HR) offered a C index of 0.80 (0.79 to 0.80, p<0.001).
Conclusion: The strongest predictors of in-hospital survival for STEMI were aspirin therapy given acutely and out-of-hospital thrombolysis, Previous STEMI models have focused on age, SBP and HR We have confirmed the importance of these predictors in the discrimination of death after STEMI, but also demonstrated that other potentially modifiable variables impact upon the prediction of short-term mortality.
Statistics from Altmetric.com
Over a quarter of a million people suffer an acute myocardial infarction (AMI) in the United Kingdom each year. Many die within the first two hours and at least half die within a month.1 Although primary percutaneous coronary intervention (PCI) for ST-elevation myocardial infarction (STEMI) offers advantages over and above thrombolysis for STEMI,2–4 the majority of patients who have STEMI in the United Kingdom are treated with thrombolytic agents.5 Implicit to thrombolysis therapy is the requirement for its prompt delivery as this has been demonstrated to influence outcome.6–10
Besides the timing of thrombolysis for STEMI, other factors have been suggested to predict mortality. Risk models for patients with STEMI, such as the Evaluation of the Methods and Management of Acute Coronary Syndromes (EMMACE) risk model11 and the Simple Risk Index (SRI)12 have shown that age, systolic blood pressure (SBP) and heart rate (HR) at admission predict death at 30 days. The Thrombolysis in Myocardial Infarction (TIMI) risk score for STEMI offers good discriminatory power for death within 14 days of admission but is dependent on the collection of 10 predictor variables. Other acute coronary syndrome (ACS) risk models describe additional predictor variables (over and above that of age, SBP and HR) and are applicable to the wider range of patients with ACS.13–22 Although these models are good discriminators of mortality, they are often based on temporally remote and specific subpopulations.
We aimed to determine predictors of in-hospital mortality for STEMI using the Myocardial Infarction National Audit Project database (MINAP), an extensive community-based cohort of patients from England and Wales hospitalised with an ACS. We believe this is important because it allows the identification of contemporary key variables that determine mortality in this “real-world” population, which will therefore allow the appropriate appraisal of new cardiac services such as primary PCI.
METHODS
The MINAP database
The Myocardial Infarction National Audit Project (MINAP) covers all acute hospitals in England and Wales (n = 228).23 24 Data are collected prospectively at each hospital, electronically encrypted and transferred online to a central database where there is the facility for contemporary analysis and dissemination. Each patient entry offers details of the patient journey, including the method and timing of admission, inpatient investigations, results and treatment, and (if applicable) date of death (from linkage to the Office for National Statistics, using the unique NHS number).
Statistics
We studied all patients in England and Wales who were admitted to hospital with an ACS and who were entered into the MINAP database between 1 January 2003 and 31 March 2005. We only analysed data for the first recorded (index) hospital admission for an individual patient in MINAP. We selected patients between the ages of 18 years and 100 years who presented with an admission SBP between 49 mm Hg and 250 mm Hg, and HR between 20 bpm and 200 bpm. We identified patients with STEMI if they had ECG evidence of ST elevation consistent with infarction of ⩾2 mm in contiguous chest leads and/or ST elevation of ⩾1 mm in two or more standard leads or new left bundle branch block and had a creatine kinase rise >2× upper limit of normal or troponin rise defined locally as that of an acute myocardial infarction.
Basic statistics
Continuous data were expressed as means (SD) or as median and interquartile ranges for skewed distributions. Discrete or categorical data were summarised using frequencies and percentages. An independent t test was used for comparison of normally distributed data; otherwise corresponding non-parametric tests were used. Association between inpatient mortality and potential predictor factors were quantified by odds ratios (OR) with 95% confidence intervals (CI) and p values. Using the cohort, we performed a series of univariate logistic regressions to predict in-hospital mortality. We selected those clinical variables, based on other studies and our experience, that are collected on admission to hospital. All variables with a Wald score greater than 15 or significance level (p value) <0.25 were included in the initial multivariate logistic regression analyses to predict mortality. We then eliminated factors from the multivariate logistic regression if their p values were greater than 0.05, but retained clinically relevant factors. The quality of the discriminative ability of the resultant model was judged by the area under the receiver operator curve.25 We used the statistical software package SPSS version 12.
RESULTS
Study population
Of 104 988 patients who had complete data for age, HR and SBP, there were 5995 who either did not meet the inclusion criteria or had no data for the final diagnosis. For the remaining 98 993 patients, 61.6% were male. The mean (SD) age, SBP and HR were 68.9 (13.8) years, 138.6 (29.6) mm Hg and 83.4 (24.1) bpm, respectively, and the 30-day and 1-year mortality was 13.4% and 19.2%.
STEMI population
We identified 34 722 (36.0%) patients with STEMI. There was a preponderance of males (23 764, 68.7%). A minority presented with a SBP less than 90 mm Hg (1356, 3.9%) or HR greater than 100 bpm (4711, 13.6%). Only 850 (0.8%) patients received primary PCI (and accounted for 2.4% of STEMIs), which continues to be the exception rather than the rule in most UK centres. The clinical characteristics of the STEMI cohort are shown in table 1. Nearly 80% (26 479, 76.6%) of patients with STEMI received thrombolysis, with 53% (17 499) having it administered in the accident and emergency department and 3.7% (1215) receiving out-of-hospital thrombolysis. Most decisions to use thrombolytic treatment were made either by an accident and emergency clinician (36.8%) or member of the on-call medical team (24.1%). The in-hospital mortality was 10.6% and 1615 patients (5.4%) died within 24 hours of hospital admission. The majority of patients with STEMI were discharged on β-blockers (76.3%), angiotensin-converting enzyme (ACE) inhibitors (82.3%), statins (90.7%) and aspirin (91.8%).
Univariate predictors of mortality
As expected, thrombolysis treatment offered an in-hospital mortality reduction, with thrombolysis given before hospital admission being more advantageous than in-hospital thrombolysis (OR = 0.13, 95% CI 0.01 to 0.19, p<0.001 and OR = 0.40, 95% CI 0.37 to 0.43, p<0.001, respectively) and thrombolysis given by a paramedic being more advantageous than being given by a member of the on-call medical team (OR = 0.25, 95% CI 0.19 to 0.36, p<0.001 and OR = 1.05, 95% CI 0.97 to 1.15, p<0.001, respectively). Chronic heart failure, cerebrovascular disease and a history of chronic renal failure were powerful predictors of death in the univariate analysis, whereas glucose concentration did not predict in-hospital outcome. These and other associations with in-hospital mortality are shown for each baseline characteristic in table 2. Established predictors including age, SBP and HR at admission were good univariate predictors of in-hospital mortality.
Independent predictors of mortality
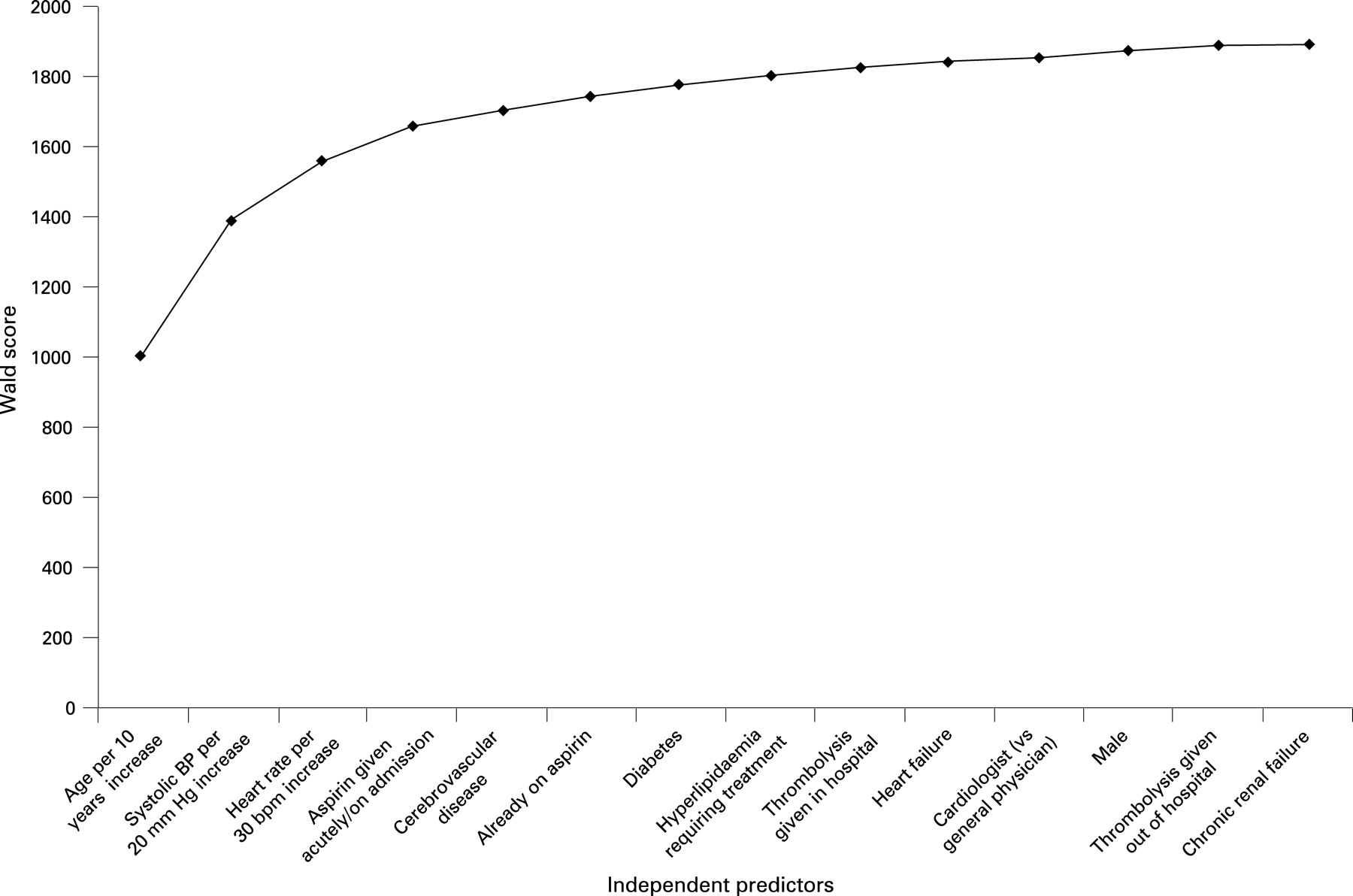
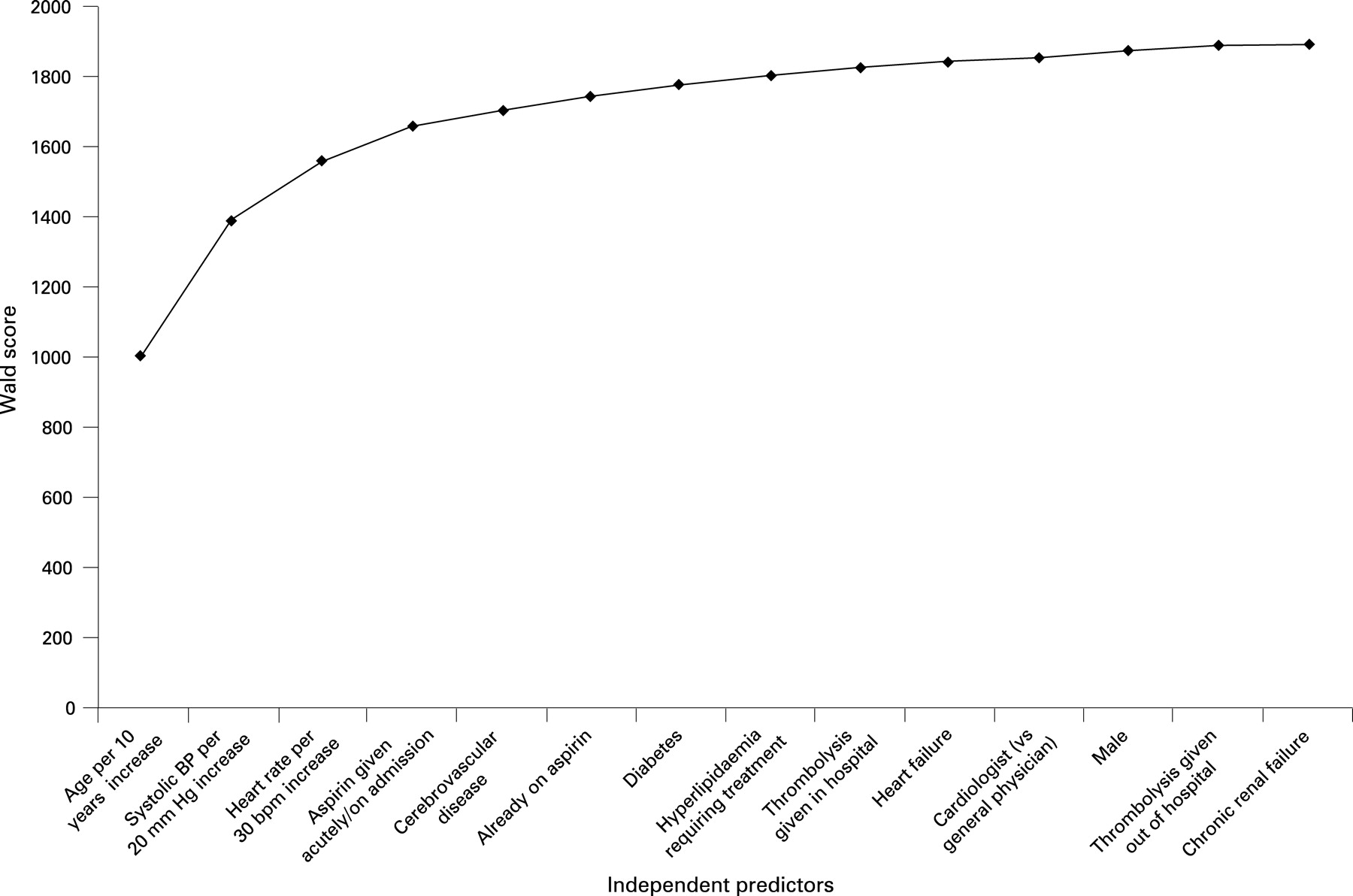
Because there was a strong correlation (p<0.0001) between who administered thrombolysis and where it was administered, we only considered where it was given in the multivariate analysis. The highest odds ratios were aspirin therapy given acutely/on admission and thrombolysis out of hospital. Both these variables were independently associated with a reduction in the risk of in-hospital death by more than half. They were closely followed by age and a history of cerebrovascular disease (table 3). A 10-year increase in age doubled the risk of in-hospital death and the presence of cerebrovascular disease increased mortality risk by 1.7. A history of heart failure was the next most important variable, followed by a history of chronic renal failure and a 30 bpm increase in heart rate. Univariate predictors that were not statistically significant independent predictors included a history of myocardial infarction, hypertension, angina, peripheral vascular disease, chronic obstructive airways disease, smoking and elevated cardiac markers. The final risk model comprised 14 predictors of death, C index = 0.82 (95% CI 0.82 to 0.83, p<0.001) (fig 1). The relative contributions of the predictor variable to the final model are shown in figure 2. A simple model, comprising age HR and SBP, offered a C index of 0.80 (95% CI 0.79 to 0.80, p<0.001).

{kind=link}
{kind=link}
DISCUSSION
This study, using data from a large national registry of ACS patients, highlights the prognostic importance of several baseline characteristics reported from previous models using other databases.15–20 The two factors most strongly associated with in-hospital survival for STEMI were thrombolysis given out of hospital and aspirin given acutely/on admission to hospital.
Previous STEMI models have focused on the importance of age, SBP and HR.11 12 We have confirmed the importance of these predictors in the discrimination of death after STEMI, but also demonstrated that other variables have an impact on the prediction of short-term outcome. However, the effect of the additional 11 variables only improved the C index from 0.80 (0.79 to 0.80) to 0.82 (0.82 to 0.83), which is similar to the performance of other STEMI risk models (EMMACE (C index 0.77)11 and the Simple Risk Index (SRI) (C index 0.78)12) that also only use age, HR and SBP to predict short-term mortality. A concern with complex risk scores is that they rely on the collection of multiple variables when it is known that secondary abstraction of difficult-to-obtain key clinical findings adds little to their predictive power.26
None the less, delays to thrombolysis are an important determinant of outcome. Administration of thrombolysis out of hospital was associated with a threefold better outcome than that of in-hospital thrombolysis and corroborate recent findings that longer intervals from prehospital treatment to arrival in hospital are associated with high re-infarction rates, which in turn are associated with elevated mortality rates.6 Although the mortality risk reduction associated with prehospital thrombolysis is likely to reflect the reduction in delay to thrombolysis it is also possible that those who received thrombolysis out of hospital were a different subpopulation from those who had treatment in hospital. Our results suggest that thrombolysis administered by paramedics offers a better outcome that that administered by the on-call team. However, this is likely to represent the timing of thrombolysis and not the standard of care given by different healthcare workers. Because thrombolysis is still the standard treatment for STEMI in most parts of the United Kingdom and because its timing is a numerical, then methods to reduce the time to thrombolysis will effect an improvement in outcome. This is in contrast to the more static predictor variables of age, heart failure, chronic renal failure and so on that cannot be immediately affected on presentation.
Interestingly, we found that STEMI univariate predictors of inpatient mortality included a history of smoking and the presence of hyperlipidaemia requiring treatment. The seemingly better prognosis of smokers after acute myocardial infarction has previously been documented.27 Even so, a history of smoking was not found to be a multivariate predictor in our final model. This corroborates previous findings where after adjustment for baseline and clinical variables (younger age and a more favourable risk profile of smokers), the improved outcome of smokers was no longer evident.28 A history of treated hyperlipdaemia was associated with a reduced inpatient mortality risk and may reflect the use of hydroxymethyl glutaryl coenzyme A (HMG CoA) reductase inhibitors as primary and secondary prophylactics agents (and that such patients may also be taking other drugs such as aspirin and β-blockers that modify outcome from STEMI).
Comparison with other models
Compared with other risk models, factors that appear to be more important in this cohort of patients were cerebrovascular disease and where thrombolysis was administered (which is likely to be a surrogate for time to thrombolysis). This model therefore incorporates those variables found to be prognostically significant in other models of selected (trial) patients, with new variables identified from a “real world” population.
Other popular risk models demonstrate good discriminative power but, because they have not been externally validated in the UK population, they may not be applicable to our population. This is because some are based upon results of randomised controlled trials that exclude high-risk patients and are not representative of our general population (indeed validation of models in the derivation cohort may overestimate their performance29–31). Although the GRACE model16 (which was derived from an unbiased population of ACS patients) has good discriminatory power for inpatient mortality across the entire spectrum of ACS, it does not evaluate wholly patients with STEMI and requires the collection of multiple predictor variables not immediately apparent on admission. This is also true for other ACS risk models. Although the TIMI risk score for STEMI20 is appropriate to our diagnostic category, it requires the collection of 10 baseline variables and does not offer the prediction of in-hospital mortality. (We used in-hospital mortality rather that 30-day mortality as a marker of outcome because the identification of high-risk patients with STEMI requiring more intensive inpatient management is important). Of note is that the TIMI risk index has recently been found to be a valid and moderately accurate tool for the stratification of risk for early death in patients with and without STEMI in a community setting remote from their derived population.32 Our full model incorporates multiple variables, though, as demonstrated, three key predictors account for the majority of the performance of the model. As such, a simplified model such as EMMACE or SRI the may be more appropriate to urgent risk evaluation of individuals. Moreover, if doctors are to risk-stratify patients at time of presentation of STEMI, then any risk prediction tool should be easy to use and be based on uncomplicated and readily available data.
Accurate determination of risk is important in the evaluation of short-term outcome after initial “emergency” treatment has been administered (for example, aspirin and thrombolysis). Although it is important in the initial evaluation of patients with STEMI that risk derivation should not delay emergency treatment. We believe that risk models with good discriminative performance should also be used for case-mix adjustment so that hospital performances may be compared. Models that take into consideration patient demographics, presentation and treatment permit accurate comparison of process and outcome data.
Limitations
Our analysis was dependent upon the extent and validity of data in the MINAP database. Data entry is subject to routine online error checking. There is a mandatory annual data validation exercise for each hospital involving the completion of data entry for 20 fields from 20 sets of randomly generated records for patients whose data had been previously entered. In total, we had data for 187 069 first admissions. Of these, 82 081 (43.9%) had missing data in at least one of the age/HR/SBP variables. When we compared the mortality we found that 30-day mortality rates were 10.2% versus 12.7% (p<0.001) for those patients included (100 686) versus those excluded (86 383) and long-term mortality rates of 17.8% versus 24.2% (p<0.001) for those patients included versus those excluded. We did not impute for missing data since others have shown that this does not affect the main result17 (however this has yet to be determined for the MINAP dataset). We found a significant difference in mortality rates between those patients included and excluded from the analysis. The exclusion of patients with missing data, therefore, could lead to biased risk estimates,33 but at worst we may have offered a conservative estimate of the predictive power of the model. Furthermore, it may be that those excluded had a higher mortality because they were the most seriously ill and it was more difficult to obtain and record accurate data for the MINAP database. Of those included versus excluded, there were more patients with diabetes (18.6% vs 18.3%, p = 0.01), fewer with cerebrovascular disease (8.3% vs 9.7%, p = 0.02) and heart failure (6.4% vs 9.4%, p<0.001) and similar proportions with chronic renal failure (3.4% vs 3.6%). Even so, we believe that the number of patients who were analysed and the data that were used were of sufficient quality to enable an accurate analysis of risk factors and render our results reliable and applicable.
CONCLUSION
This paper confirms the importance of early thrombolysis. We have demonstrated that early thrombolysis (out-of-hospital compared to in-hospital treatment) has a significant impact upon inpatient survival. Although variables such as age, SBP and HR are key to the prediction of outcome, revascularisation is not a fixed predictor variable and therefore can be modified. As such it should continue to be targeted in an attempt to reduce thrombolysis times and improve the outcome of patients with STEMI.
Acknowledgments
The extract from the MINAP database was provided by Dr J S Birkhead, clinical director of MINAP, the National Audit of Myocardial Infarction, National Institute for Clinical Outcomes Research, The Heart Hospital, London. We acknowledge all the hospitals in England and Wales for their contribution of data to MINAP.
REFERENCES
Footnotes
Competing interests: None.
Funding: MINAP is funded by the Healthcare Commission
Contributors: CG researched and wrote the manuscript. SM performed the statistics and wrote the article. CW, PB, JB and AH reviewed, wrote and critically appraised the article. All authors read and approved the final manuscript.