Article Text

Abstract
OBJECTIVES To examine the impact of time to thrombolytic treatment on multiple acute outcome variables in a single trial of thrombolysis in acute myocardial infarction.
DESIGN AND PATIENTS Mortality and reinfarction rate were measured in 2770 patients with acute myocardial infarction who received thrombolysis within 12 hours in CORE, an international, dose ranging trial of poloxamer 188. Tc-99m sestamibi infarct size and radionuclide angiographic ejection fraction substudies included 1099 and 1074 patients, respectively.
RESULTS Time to thrombolysis, subgrouped by intervals (< 2, 2–4, ⩾ 4–6, and ⩾ 6 hours), was significantly associated with infarct size (median 15.0%, 18.5%, 22.0%, 18.5% of left ventricle; p = 0.033), mean (SD) ejection fraction (51.5 (12.0)%, 48.3 (13.9)%, 48.2 (13.3)%, 48.2 (15.0)%; p = 0.006), 35 day mortality (5.7%, 7.1%, 7.9%, 12.5%; p = 0.0004), six month mortality (7.3%, 8.6%, 10.4%, 15.5%; p < 0.0001), and 35 day reinfarction rate (6.1%, 3.2%, 4.0%, 0.9%; p = 0.0001).
CONCLUSIONS In this single large trial, the beneficial effect of time to thrombolysis on infarct size and ejection fraction was restricted to treatment given within two hours of symptom onset, while the effect on mortality was evident over all time intervals. Reinfarction rate was higher in patients treated with earlier thrombolysis.
- myocardial infarction
- thrombolysis
- infarct size
Statistics from Altmetric.com
The benefits of thrombolytic treatment are greatest when it is given early in acute myocardial infarction.1 In animal models, infarct size and left ventricular function, the major prognostic determinants in clinical myocardial infarction, were adversely affected in a rapid and non-linear fashion by the duration of coronary occlusion.2 ,3 Attempts to demonstrate such an association in clinical studies have yielded conflicting results. One meta-analysis1 and two trials4 ,5 of thrombolysis in acute myocardial infarction suggest a direct linear effect of time to thrombolysis on mortality, infarct size, and ejection fraction, with a gradual diminution of benefit with increasing delay. In contrast, other clinical trials6-8 indicate a non-linear delay/benefit relation, with a pronounced decline in benefit after occlusion of one to three hours. Beyond this time threshold, other factors—such as the degree of myocardium at risk, collateral blood flow, and metabolic demand—exert a greater impact on outcome.9 ,10
Reports on the effect of time to thrombolysis in acute myocardial infarction are restricted to selected outcome measures and smaller trials.1 ,5 ,7 ,8 ,11-16 Most of these studies have analysed only short term mortality. Our aim in the present study was therefore to examine the association between time to administration of thrombolytic treatment and multiple end points—infarct size, ejection fraction, 35 day and six month mortality, and 35 day reinfarction rate—in a single trial of thrombolysis in acute myocardial infarction. Although there is evidence of benefit from thrombolysis beyond six hours to within 12 hours from symptom onset,17 time increments beyond six hours were not analysed in this study owing to the smaller benefits relative to earlier reperfusion treatment.18
Methods
The Collaborative Organisation for RheothRx Evaluation (CORE) trial was an international, multicentre, randomised, dose ranging study of poloxamer 188 (RheothRx; Burroughs Wellcome, USA) in acute myocardial infarction.14
STUDY POPULATION
In all, 2948 patients were randomised. Patients were eligible if they had symptoms consistent with acute myocardial infarction and at least 1 mm ST segment elevation in two or more contiguous ECG leads or new left bundle branch block. Exclusion criteria have been reported previously.14
Thrombolytic treatment was strongly encouraged; the 144 patients (4.9%) who did not receive thrombolysis were excluded, as were 28 (0.9%) with missing time to thrombolysis. Choice of the thrombolytic agent and other standard treatments was at the discretion of the attending physician. Patients were randomised in a blinded fashion to either thrombolysis alone, or to thrombolytic treatment plus one of five dosing regimens of poloxamer 188. The overall effect of this agent on mortality, ejection fraction, and infarct size was not significant.14
HISTORICAL AND HAEMODYNAMIC VARIABLES
Multiple clinical variables were recorded prospectively for each patient (table 1). Follow up was obtained at 35 days and six months.
Clinical characteristics of SPECT versus non-SPECT patients
CLINICAL OUTCOME EVENTS
Patients were monitored for outcome (death, reinfarction, or cardiogenic shock) while in hospital with the qualifying acute myocardial infarct, and after discharge, at 35 days and six months. During the index hospital admission, cardiogenic shock was diagnosed if the patient had, first, a persistently low systolic blood pressure (< 90 mm Hg) which was not responsive to fluid therapy alone, required intravenous inotropic support, and was felt to reflect cardiac dysfunction; and second, clinical evidence of poor perfusion (for example, decreased skin temperature, cyanosis, reduced urine output). After the index hospital admission, cardiogenic shock was recorded if the patient was readmitted and required intravenous inotropic support, and if there was a discharge diagnosis of cardiogenic shock. In unusual situations, inotropic support included management with mechanical support (for example, pump or ventilation), without initial intravenous inotropes.
Tc-99M SESTAMIBI INFARCT SIZE SUBSTUDY
The Tc-99m sestamibi infarct size SPECT (single photon emission computed tomography) substudy included 104 centres and a central laboratory at the Mayo Clinic in Minnesota, USA. If participating in the infarct size substudy, the centre was expected to enrol all eligible patients. Before infarct size assessment, cumulative mortality for the infarct size substudy group was 5.3% at day 6 and 6.3% at day 16, and the revascularisation rate was 13.8% (152 patients), with a mortality of 3.3% (five patients). Infarct size assessment was subsequently performed on 1113 patients between day 6 and day 16. Fourteen patients (1.2%) were excluded for technical reasons. In all, 1099 patients were analysed. Quality control of all imaging cameras was performed before patient studies.15 ,16 Tc-99m sestamibi acquisition was carried out as previously described16 and validated in animal19 and clinical studies,20where a 60% threshold has been shown to provide optimal separation between viable and non-viable myocardium.21 The raw planar image data were forwarded to the central core laboratory for infarct size quantitation (expressed as per cent of left ventricle). This measurement included new and old infarcts.
RADIONUCLIDE ANGIOGRAPHY OF LEFT VENTRICULAR FUNCTION
The radionuclide angiography (RNA) substudy included 114 centres and a central laboratory at The Toronto Hospital, Ontario, Canada. If participating in the RNA substudy, the centre was expected to enrol all eligible patients. Before RNA assessment, cumulative mortality was 4.9% at day 6 and 6.2% at day 16, and revascularisation rate was 15.0% (161 patients), with a mortality of 2.5% (four patients). RNA was subsequently attempted on 1172 patients between day 6 and day 16. Fifty two patients (4.2%) were excluded because of technical inadequacies, and 46 (3.7%) for administrative reasons. In all, 1074 patients were analysed. In all participating centres, the equilibrium RNA procedure was performed according to a standardised protocol.22 The unsmoothed studies were forwarded to the central laboratory for analysis, using a semiautomatic method.23 Left ventricular ejection fraction was calculated using standard techniques.23
STATISTICAL ANALYSIS
Quantitative data are expressed as mean (SD), with the exception of infarct size where, because of a severely rightward skewed distribution, the results are summarised as median (interquartile range). Kruskal–Wallis analysis of variance with time to treatment in four discrete intervals (< 2 hours, 2–4 hours, ⩾ 4–6 hours, ⩾ 6 hours) was used to assess the significance of the univariate correlation between time to treatment and infarct size or ejection fraction. Univariate and multivariate analyses were used to adjust for independent predictors of infarct size and ejection fraction. An odds ratio was performed by comparing the rates of events and mortality at different time intervals. Age, sex, thrombolytic agent, myocardial infarction location, previous myocardial infarction, diabetes mellitus, congestive heart failure, and coronary artery bypass grafting were included as cofactors in the analysis to allow adjustment for these variables. Furthermore, a product term in the models of infarct size and left ventricular ejection fraction allowed for a time × thrombolysis type (tissue plasminogen activator (t-PA)v others) interaction. These models also included adjustment for previous myocardial infarction, infarct location, and poloxamer 188 treatment.
Results
OVERALL CLINICAL CHARACTERISTICS
Table 1 summarises the characteristics of the SPECT substudy compared with those of the non-SPECT CORE group. The mean (SD) time from symptom onset to reperfusion treatment for the SPECT group was 217 (159) minutes (range 5–1770), and for the non-SPECT group, 220 (146) minutes (range 10–1560). There were significant differences in some clinical characteristics between the two groups. The RNA substudy group had similar characteristics to the SPECT group. Table 2 summarises the characteristics of the infarct size group by time interval to thrombolysis. There were multiple significant differences between the four groups. Similar findings were noted in the RNA group.
Clinical characteristics of SPECT substudy patients
INFARCT SIZE VERSUS TIME TO REPERFUSION TREATMENT
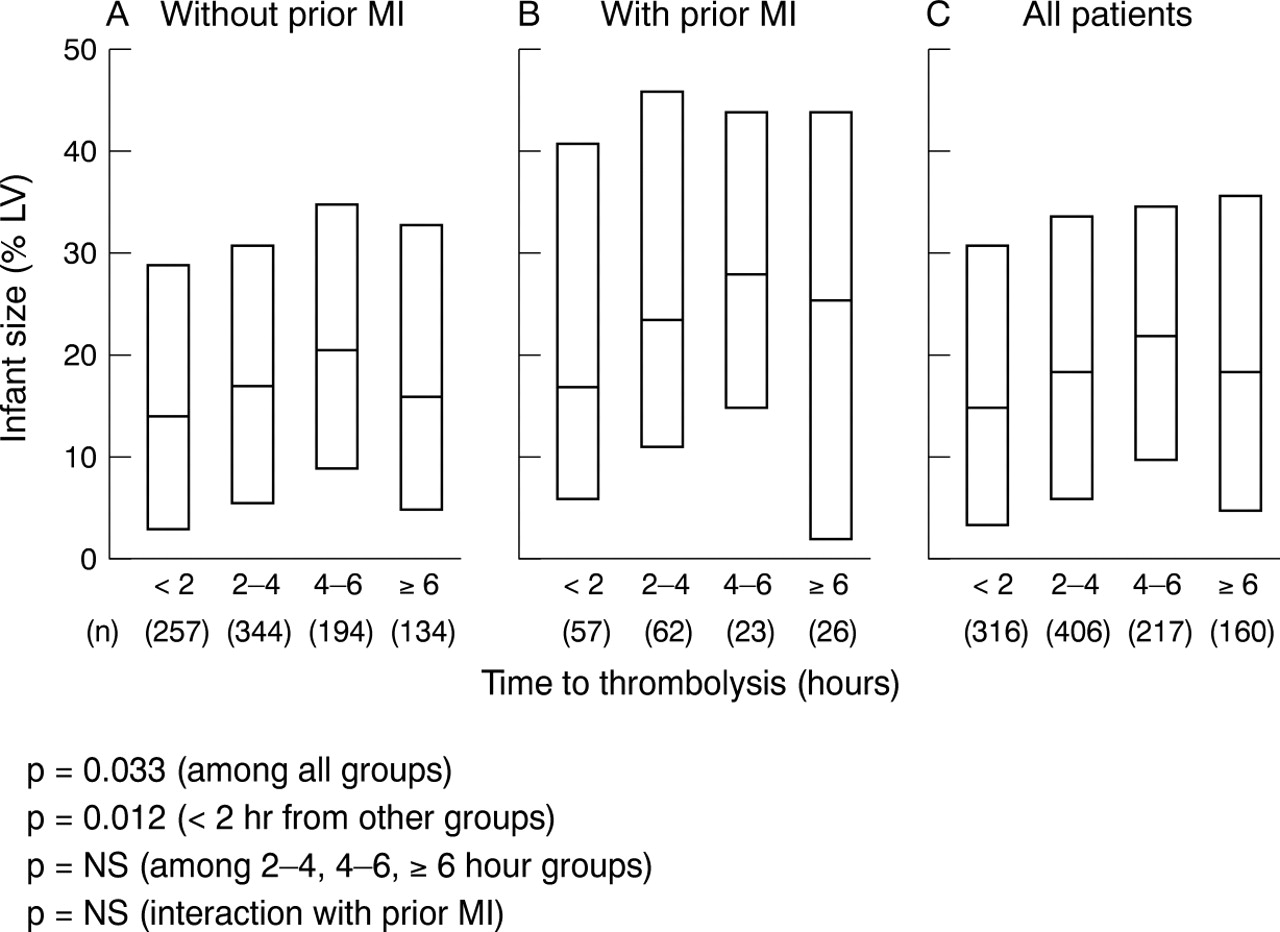
In the infarct size substudy, distribution of the 1099 patients was skewed toward early treatment, with two thirds of patients receiving thrombolysis within four hours of symptom onset. Infarct size was associated with time to reperfusion treatment (p = 0.033, fig 1). However, infarct size was highly variable for any given time to thrombolysis, with a significant degree of overlap between different time intervals. The greatest effect of time to treatment was observed in the patients treated in < 2 hours; infarct size in this subgroup (median 15%) was significantly (p = 0.012) lower than in the other subgroups (median 19%). There was no significant difference among the other time subgroups.

Box plot of infarct size versus time to thrombolytic treatment, for each time interval. (A) Patients without previous myocardial infarction. (B) Patients with previous myocardial infarction. (C) All patients. Infarct size was significantly associated with elapsed time. Infarct size in the < 2 hours subgroup was lower than in the other subgroups, among which there was no significant difference.
The effect of time to thrombolysis on infarct size was consistent for patients without and with previous myocardial infarction (fig 1A and1B). The test of the interaction between time and previous myocardial infarction was not significant (p = 0.90), neither was the interaction between time to thrombolysis and thrombolytic type (p = 0.20).
The mean difference in infarct size between those receiving early (< 2 hours) compared with more delayed treatment (⩾ 2 hours) was adjusted for confounding variables (table 3). The unadjusted mean increase in infarct size associated with later thrombolysis was 3.1% (p = 0.018), and this remained unchanged after adjustment (2.9%; p = 0.018). On average, anterior myocardial infarction was associated with a mean increase in infarct size of 16.7% (p < 0.0001). Previous myocardial infarction increased mean infarct size by 8.3% (p < 0.0001).
Adjusted effect of early thrombolysis
EJECTION FRACTION VERSUS TIME TO REPERFUSION TREATMENT
For the 1074 patients in the RNA substudy, the distribution was skewed toward early treatment, with two thirds receiving thrombolysis within four hours of symptom onset. Ejection fraction was associated with time to reperfusion treatment (p = 0.006, fig 2). Ejection fraction was also highly variable for any given time to thrombolysis. The greatest benefit of time on ejection fraction was again observed in the < 2 hour subgroup. There were no significant differences in mean ejection fraction among the other subgroups.
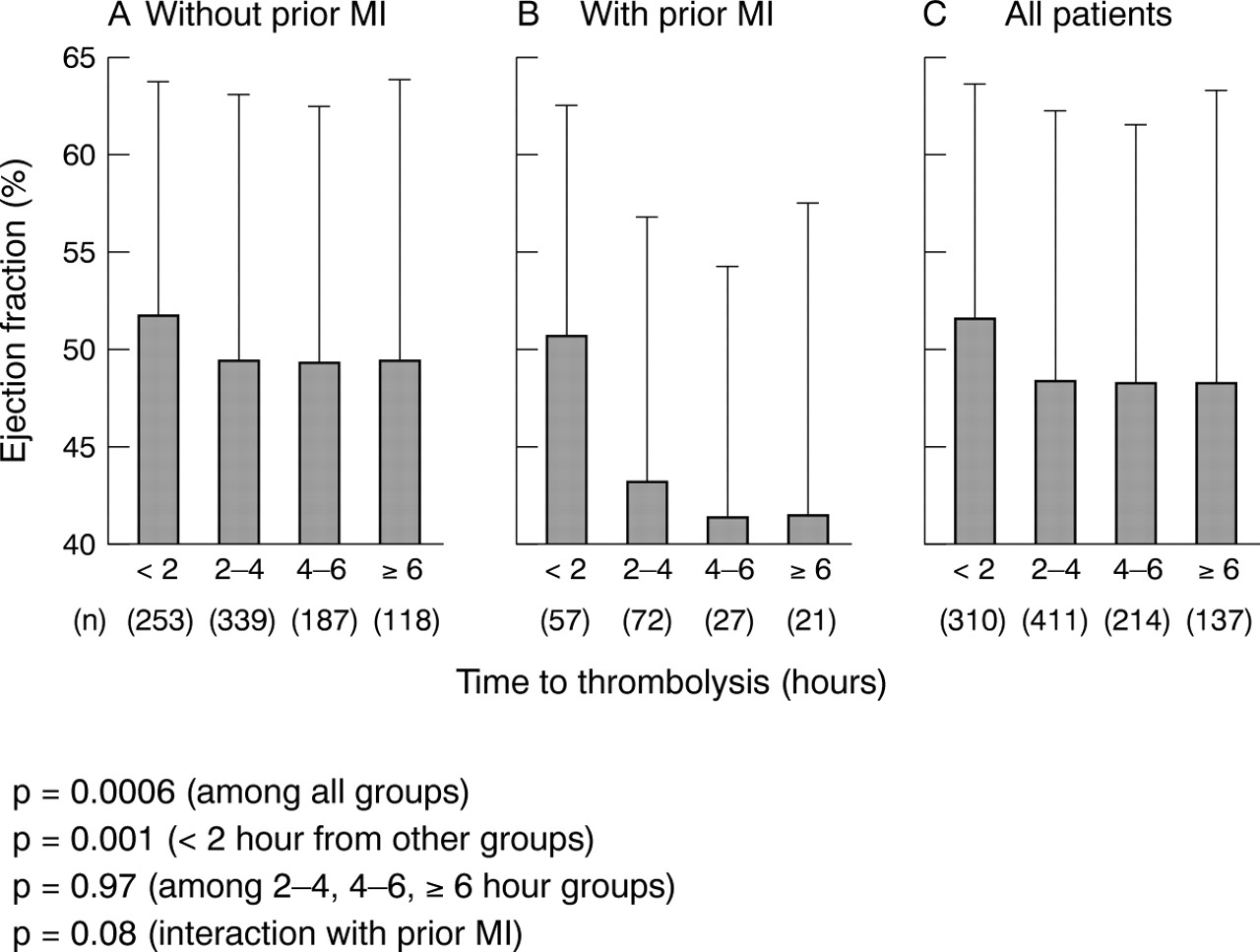
Bar graph of ejection fraction versus time to thrombolysis, for each time interval. (A) Patients without previous myocardial infarction. (B) Patients with previous myocardial infarction. (C) All patients. Ejection fraction was associated with time, p = 0.006. Ejection fraction in the < 2 hours subgroup was higher than in the other subgroups, among which there was no significant difference.
The benefit of time to thrombolysis on ejection fraction remained consistent for patients without and with previous myocardial infarction (fig 2A and 2B). The interaction of time to thrombolysis and previous myocardial infarction was of borderline significance (p = 0.076), but this effect was paradoxical in that time appeared to have less impact on the group without previous myocardial infarction. Furthermore, the interaction between time to thrombolysis and thrombolysis type was non-significant (p = 0.32).
The observed mean difference in ejection fraction between the early thrombolysis group (< 2 hours) and the more delayed (⩾ 2 hours) groups was 3.2%. Adjustment for confounding variables had little effect (table 3). Previous myocardial infarction and anterior infarct location both strongly predicted reduced mean ejection fraction (p < 0.0001 for each).
CLINICAL OUTCOMES AND TIME TO THROMBOLYSIS
There were 2770 patients in whom time to thrombolysis was known. Of these, 2734 (98.7%) were followed to day 35 and 2656 (95.9%) to six months. There were 211 deaths in the group of 2734 patients at 35 days. Figure 3 depicts the strong association between time to thrombolysis and the 35 day and six month mortality. At 35 days and at six months, regardless of previous myocardial infarction, mortality of the < 2 hours subgroup was less than half that for the ⩾ 6 hours subgroup (p < 0.0001). The 2–4 hours and ⩾ 4–6 hours subgroups also had a lower mortality (p < 0.03) than the ⩾ 6 hours subgroup (p < 0.0001 for linear trend).

Bar graph of the 35 day and six month cumulative mortality for the CORE thrombolysis population, for each time interval. (A) Patients without previous myocardial infarction. (B) Patients with previous myocardial infarction. (C) All patients. The significant association between the cumulative 35 day and six month mortality and time to thrombolysis is shown.
Adjustment for the listed variables (table 4) had little effect on the odds ratio for each interval of time to thrombolysis but did affect the p value (0.0004 unadjusted to 0.038 adjusted).
Thirty five day death rate, adjusted analysis
For the 35 day combined incidence of recurrent myocardial infarction, shock, and death, subgrouped by time to thrombolysis, there is a trend of increasing combined event rates with elapsed time of ⩾ 2 hours, regardless of previous myocardial infarction. However, the < 2 hours group paradoxically had a higher combined event rate than the 2–4 hours and ⩾ 4–6 hours groups, regardless of previous myocardial infarction. After adjustment, the odds ratio for each interval of time to thrombolysis remained similar (p = 0.19) to the unadjusted ratio.
The difference in time trends in the 35 day mortality and the 35 day combined event outcome is explained by the 35 day incidence of recurrent myocardial infarction (fig 4). There was a significant inverse trend between recurrent myocardial infarction and time to thrombolysis (p < 0.0001), regardless of previous myocardial infarction. In all patients, the highest reinfarction rate (< 2 hours subgroup = 6.1%) was six times higher than that of the ⩾ 6 hours subgroup (0.9%, p < 0.0001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bar graph illustrating the 35 day incidence of recurrent myocardial infarction, for each time interval. (A) Patients without previous myocardial infarction. (B) Patients with previous myocardial infarction. (C) All patients. There was a significant inverse trend between reinfarction rate and time to thrombolysis. The highest reinfarction rate (< 2 hours subgroup) was six times higher than that of the ⩾ 6 hours subgroup. The subgroups treated at 2–4 hours and ⩾ 4–6 hours had an intermediate level of reinfarction.
Discussion
IMPORTANCE OF EARLY REPERFUSION
This study confirms the beneficial effects of earlier reperfusion treatment in acute myocardial infarction. However, the magnitude of this time benefit on infarct size and ejection fraction was considerably less than the impact of other known determinants of outcome. A time to treatment of more than two hours was associated with an increase in infarct size of less than 40% of the increase associated with either a history of previous myocardial infarction or anterior infarct location, the most important determinant of infarct size in this model. These data support earlier animal3 ,24-26 and clinical studies,10 ,15 ,27 in which an important determinant of infarct size was myocardium at risk. The amount of myocardium at risk has been shown by SPECT sestamibi to be twofold greater for anterior than for non-anterior infarcts.28 The smaller effect of time on infarct size and ejection fraction is also consistent with the GUSTO (global utilization of streptokinase and t-PA for occluded coronary arteries) 30 day mortality data.29 Of the 12 independent predictors of mortality in that study, time provided only 1% of the prognostic information, while previous myocardial infarction provided 2.8% and anterior infarct location 6%.
These data reinforce the striking survival benefit of very early thrombolysis and the concept of the “golden hour.”7 ,8The greatest mortality benefit in this study was achieved when thrombolysis was given within two hours of symptom onset. Beyond that time, mortality reduction was attenuated. An explanation for the early survival benefit is time dependent myocardial salvage,9postulated to operate when thrombolysis occurs within one to two hours of symptom onset. The infarct size substudy, with its greatest effect of time at less than two hours, appears to support this concept.
Although results of the GUSTO trial30 ,31 show mortality rates in favour of accelerated tPA over streptokinase, in the present study the test of the interaction between time to thrombolysis and thrombolysis type was not significant, which further highlights the importance of early reperfusion treatment.
MECHANISM OF BENEFIT OF LATER TREATMENT
The mechanism of the survival benefit with later thrombolysis has been controversial.1 ,4 ,5 ,7 ,8 ,11 In this study and other trials,11 ,32-34 the mortality benefit of time beyond the two hour threshold exceeded its impact on left ventricular function and infarct size. These discrepancies suggest survival mechanisms independent of the preservation of left ventricular function and myocardial salvage, which may include prevention of cardiac rupture and electrical instability, and prevention or limitation of infarct expansion and left ventricular remodelling.18 Perfusion of the infarct related artery is also more closely related to outcome than left ventricular function.35 This open artery may provide mortality benefits by supplying collateral flow when other areas of the myocardium later become jeopardised.
Another potential explanation for the discrepancy in the effect of time on survival and ejection fraction is the time to treatment paradox. Survival of some patients with severe left ventricular dysfunction who otherwise may have died can presumably mask the gain in ejection fraction in reperfused patients and result in a discrepancy between the survival benefit and preservation of left ventricular function.36
LINEAR AND NON-LINEAR EFFECTS OF TIME
Although a monotonic but non-linear relation between the duration of coronary occlusion and final infarct size has been shown in animal models of reperfusion,2 ,3 results of previous clinical trials using mortality support both a linear1 ,5and a non-linear6-8 ,29 relation. This study shows a linear effect on mortality but a non-linear effect on infarct size. The latter is consistent with a previous single centre study.9
Concordant with the infarct size data and previous smaller studies,11-13 ,18 our ejection fraction data found a significant non-linear effect of time to thrombolysis, confirming that earlier initiation of thrombolysis preserves left ventricular function better.
On the other hand, the benefits of time on both 35 day and six month mortality suggest a linear association. While the linear versus non-linear controversy remains unresolved, this investigation shows the importance of very early thrombolysis, where mortality of the earliest treatment group was less than half that of the most delayed treatment group.
RECURRENT INFARCTION
In agreement with previous data,37 the reinfarction rate in this study was highest in the earliest treatment group, which was sixfold higher than that of the most delayed group. A possible explanation is that greater myocardial salvage renders more viable myocardium vulnerable to subsequent ischaemia and infarction.18 Obviously, improved survival with earlier thrombolysis results in more patients available for recurrent ischaemia and reinfarction.
STUDY LIMITATIONS
A potential sampling bias was introduced by the exclusion of nearly 40% of eligible patients without follow up imaging studies. A few centres enrolled patients before SPECT validation. Patients may have died before follow up was complete, or they may have refused or been too ill for the scheduled follow up. The latter supposition is supported by the higher event rate in eligible patients without follow up SPECT. However, reanalysis with only patients alive at 16 days yielded comparable event rates, suggesting early mortality as the major explanation for failure to obtain a follow up SPECT.
Given the substantial differences in baseline characteristics of patients presenting at different times, we cannot rule out the presence of other important yet unidentified baseline differences that may account for the higher mortality of the later treatment groups. As shown in table 4, adjustment for known baseline differences decreases the apparent significance of time (p = 0.0004 to p = 0.038). This modest significance might conceivably be lost with additional adjustment (as might occur with true randomisation). However, in previous larger studies,29 the significance of time was considerably greater, suggesting that the modest effect observed here may be a reflection of the limited number of deaths (n = 211).
Time to thrombolysis does not necessarily represent time to reperfusion, which is likely to be a more important predictor of outcome. However, O'Keefe and colleagues previously showed that direct percutaneous transluminal coronary angioplasty beyond two hours after symptom onset had a more variable but lesser impact on myocardial salvage than did earlier restoration of angiographic flow.38
Finally, myocardium at risk and collateral/residual flow, both important determinants of final infarct size in multiple animal and clinical studies,2 ,10 ,15 ,24-27 were not assessed in this study.
IMPLICATIONS
Although the benefits of time to thrombolysis are smaller than those of other determinants of outcome in acute myocardial infarction, for a given thrombolytic agent, time to thrombolysis is the only variable amenable to intervention. These findings emphasise the need to minimise the time delay to reperfusion treatment and to initiate thrombolysis within two hours of symptom onset.
Acknowledgments
This study was supported by a grant from Burroughs Wellcome Co, USA.