Article Text

Abstract
OBJECTIVE To quantify the change in door to needle time when delivery of thrombolytic treatment of acute myocardial infarction was changed from the coronary care unit to the emergency department.
DESIGN A comparative observational study using prospectively collected data.
SETTING Coronary care unit and emergency department of an Australian teaching hospital.
PARTICIPANTS 89 patients receiving thrombolysis in coronary care unit between June 1994 and January 1996, and 100 patients treated in the emergency department between April 1997 and May 1998.
INTERVENTIONS From April 1997, by agreement between cardiology and emergency medicine, all patients with acute myocardial infarction receiving thrombolysis were treated by emergency physicians in the emergency department.
MAIN OUTCOME MEASURE Door to needle time measured from time of arrival at the hospital to start of thrombolysis. Other outcomes included pain to needle time and mortality.
RESULTS Median door to needle times were less for patients treated in the emergency department than in the coronary care unit (37 minutes, 95% confidence interval (CI) 33 to 44 v 80 minutes, 95% CI 70 to 89, respectively; p < 0.0001). Door to needle time was under 60 minutes in 83% of emergency department patients and 26% of coronary care unit patients (57% difference, 95% CI 45% to 69%; p < 0.0001). Median pain to needle time was less for emergency department patients than for coronary care unit patients (161 minutes, 95% CI 142 to 177v 195 minutes, 95% CI 180 to 209; p = 0.004); times of less than 90 minutes occurred in 18% of emergency department patients v 1% of coronary care unit patients (17% difference, 95% CI 9% to 25%; p < 0.05). Overall mortality was similar in patients treated in the emergency department and the coronary care unit.
CONCLUSIONS With a collaborative interdepartmental approach, thrombolytic treatment of acute myocardial infarction was more rapid in the emergency department, without compromising patient safety. This should improve the outcome in patients with infarcts treated with thrombolytic agents.
- thrombolysis
- door to needle time
- treatment delay
- acute myocardial infarction
Statistics from Altmetric.com
The treatment of acute myocardial infarction has been studied intensively over the past 15 years. Proven benefits have led to the routine administration of thrombolytic agents in such patients.1 ,2 The data show that thrombolytic agents decrease overall 30 to 35 day mortality by 18–25%, with increasing benefit as the time from onset of pain to thrombolysis is reduced.1-4
One way of reducing this time is by minimising the delay in starting thrombolytic treatment once the patient has reached hospital. The Australasian Council on Healthcare Standards (ACHS) uses the proportion of patients with acute myocardial infarction who have door to needle times of under 60 minutes as a national clinical indicator.5 ,6 Other authorities have recommended that the median door to needle time should be under 30 minutes.7Moving the site of decision making and administration of thrombolysis to the emergency department has been recommended to minimise delay in starting the treatment. Previous studies have either compared different thrombolytic strategies between local hospitals or have reviewed trial registry data from hospitals using different pathways.8-12 We could locate no studies in a MEDLINE search comparing emergency department with coronary care unit door to needle time in a single institution before and after changing to emergency department initiated thrombolysis.
The departments of cardiology and emergency medicine in our hospital made a joint decision to change to emergency department initiated thrombolysis. This provided an opportunity to assess this intervention prospectively in an Australasian setting. The aim of our study was to document whether a move to emergency department based thrombolysis significantly reduced the door to needle time.
Methods
The study was conducted at a tertiary teaching hospital in which 35 000 patients are seen yearly in the emergency department, with an admission rate of approximately 45%. On average 450 to 500 patients a year have a primary diagnosis of acute myocardial infarction byInternational Classification of Diseases, ninth revision (ICD-9) discharge code.
In early 1994, we developed a fast track protocol for thrombolytic treatment of patients presenting with acute myocardial infarction. Cardiology medical staff assessed eligibility for thrombolysis after early referral from the emergency department, and treatment was given in the coronary care unit after rapid patient transfer. Prospective data collection began several months after this protocol was initiated. In April 1997 an agreement was made between the departments of cardiology and emergency medicine that all patients presenting to the emergency department with acute myocardial infarction and fulfilling criteria for thrombolytic treatment should have the treatment given in the emergency department by emergency physicians.
The study groups consisted of a preintervention group of 89 coronary care unit patients and a postintervention group of 100 emergency department patients. The coronary care unit data were collected prospectively on non-consecutive patients treated between June 1994 and January 1996. The non-consecutive nature of the data usually reflected administrative problems, but data collection was evenly spread throughout the period of study. A retrospective search was undertaken to identify patients treated in the coronary care unit group who had not been included in the prospective register. Basic demographic, time point, and outcome data were collected to allow comparison against those included in the register. It was logistically impossible to carry out a full review of all 640 patients with acute myocardial infarction admitted during this period, to identify cases where thrombolytic treatment had been missed by the register. The retrospective search used the combination of a code for “streptokinase drug alert” combined with the primary discharge code of acute myocardial infarction, and therefore was likely to miss patients given tissue plasminogen activator (alteplase). An additional search was made using death during the index admission with a primary diagnosis of acute myocardial infarction, and a subsequent review of case records was performed to review all morbid outcomes associated with thrombolytic treatment in the coronary care unit population.
The emergency department data were collected prospectively on consecutive patients receiving thrombolysis in the department from April 1997 to May 1998. Data from January 1996 to March 1997 were not available owing to technical problems with data collection during that period.
Data were collected in thrombolysis registers located in the respective departments and then transferred to computer spreadsheets. Information collected for both groups included time of pain onset, time of arrival at hospital, time when thrombolytic treatment was started, and intermediate time points that describe the process of care (fig 1). In addition, call to needle times—that is, time from entry to medical system (for example, call to ambulance service) to drug delivery)—were calculated from the St John Ambulance database if patients were in the database.

Emergency department (ED) versus coronary care unit timelines for patients receiving thrombolysis. CCU, coronary care unit.
Demographic data, site of infarct, type of thrombolytic agent, and outcome data (including deaths, inappropriate thrombolysis, and complications of treatment) were collected. These were gathered by reviewing the medical record at a later date. Delays associated with initially non-diagnostic ECGs or entry into clinical trials did not lead to exclusion from the study. Pharmacy records were reviewed to establish the overall use of thrombolytic agents for patients with myocardial infarcts during the study periods. The numbers of patients with a primary diagnosis of acute myocardial infarction for each year were calculated from the ICD-9 discharge codes.
As a registered quality improvement activity, the study was exempt from requiring ethics committee approval.
STATISTICAL ANALYSIS
Univariate analysis was performed on continuous and categorical variables. Medians were calculated for all time intervals, and the Mann–Whitney test used to determine differences in these intervals between emergency department and coronary care unit; 95% confidence intervals (CI) were calculated around differences between the two clinical units in the proportion of patients receiving thrombolysis within specific time intervals. Fisher's exact test (two tailed) was used to compare discrete contingency table variables. Analysis was undertaken using the Statistical Package for Social Sciences (SPSS; version 8.0) and significance was achieved at α < 0.05.
Results
There were 89 patients in the coronary care unit group with a median age of 63 years (range 28 to 82 years); 63 (71%) were male, 26 (29%) were female. There were 100 patients in the emergency department group with a median age of 65 years (range 29 to 91 years); 78 (78%) were male, 22 (22%) were female. To evaluate the completeness of data collection, the total number of patients in the thrombolysis registry was checked against central pharmacy data for the number of thrombolytic treatments dispensed in the corresponding period. In the emergency department group, all use of thrombolytics by pharmacy data was accounted for. In the coronary care unit study period, it was estimated that 180 doses of thrombolytic drugs were dispensed (40 alteplase, 140 streptokinase), of which 89 (50%) were included in the prospective register and 69 (38%) were found on retrospective review (total 158 (88%)). Of the missing 22 episodes, 14 were given alteplase and eight streptokinase; a few of these patients may have received thrombolysis for indications other than acute myocardial infarction.
Streptokinase was given to 61 patients in the emergency department (61%), compared with 66 (74%) in the coronary care unit group, the remainder receiving alteplase. This difference was significant (Fischer's exact p = 0.0284). The site of the myocardial infarct was similar between the two prospective groups (table 1). Entry into clinical trials occurred in 10/89 patients in the coronary care unit group versus 8/100 in the emergency department group (p > 0.05).
Site of acute myocardial infarction (AMI)
The age and sex distribution, times to thrombolysis, and outcomes for the register and non-register (retrospective) populations for the coronary care unit group are compared in table 2. The apparently lower rate of alteplase use in the non-register coronary care unit patients and the higher mean and median age in part reflect the inability to identify retrospectively those patients receiving alteplase who were not included in the register. There was no significant difference in median door to needle time between the prospective and retrospective coronary care unit patients, even though other variables were different—for example, more late presentations and an older population (streptokinase patients).
Comparison of characteristics of coronary care unit (CCU) patients collected prospectively with those in a retrospective population survey
No differences were observed between the groups in the time taken for patients to reach hospital following the onset of pain (table 3). The difference in the median time taken to decide whether to give thrombolytic drugs in the emergency department group compared with the time taken by emergency department physicians to call a cardiologist in the coronary care unit group was not significant (29v 30 minutes; p = 0.705).
Comparison of pain to door, door to decision, door to needle, and pain to needle times
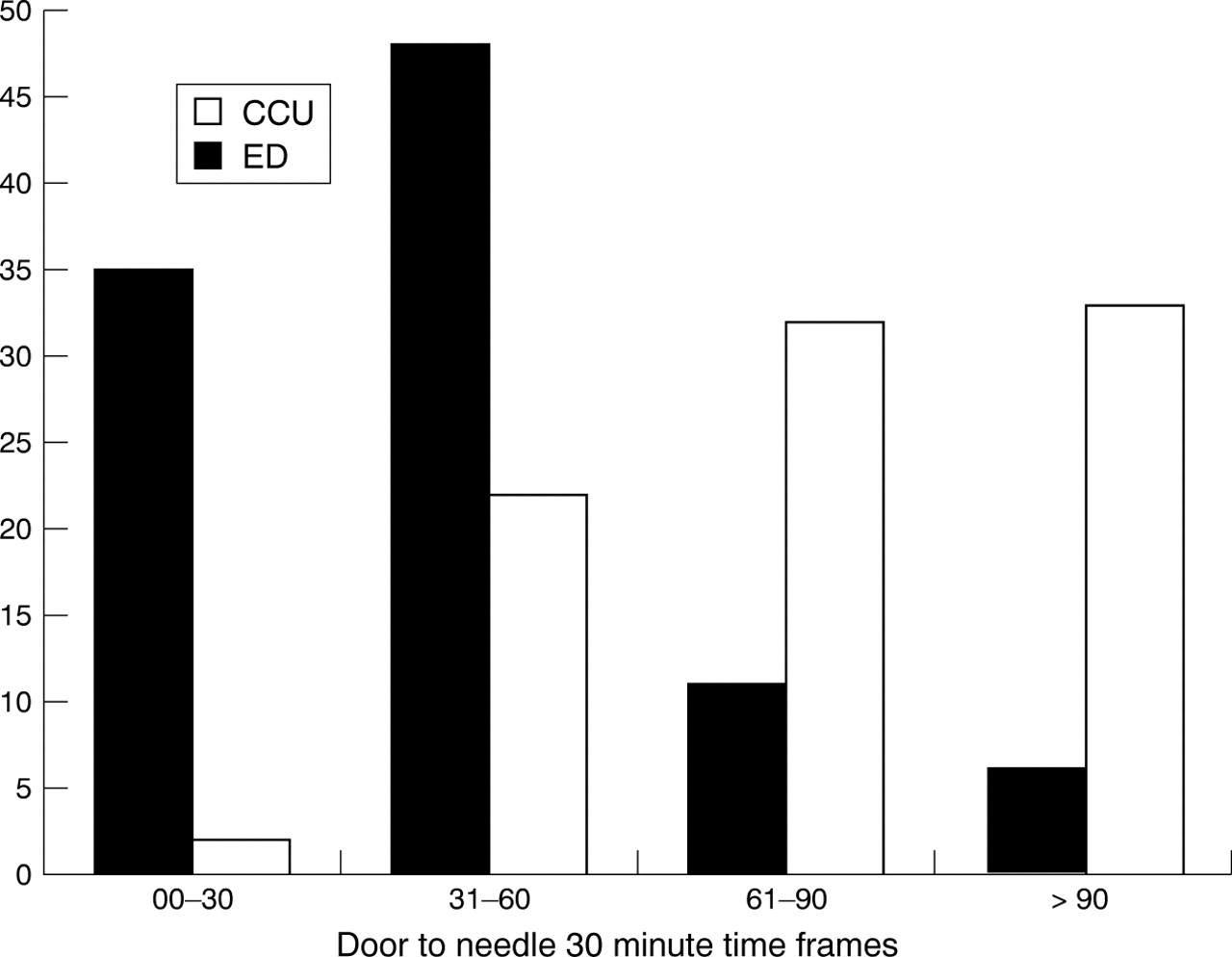
Median door to needle time for emergency department patients was 37 minutes (95% CI 33 to 44) compared with 80 minutes (95% CI 70 to 89) for coronary care unit patients (p < 0.0001). Only one of the coronary care unit patients (1%) had a door to needle time of 30 minutes or less, compared with 32 emergency department patients (32%; difference 31%, 95% CI 22% to 40%, p < 0.0001) (fig 2). For emergency department patients, 83 (83%) met the performance indicator of a door to needle time of 60 minutes or less versus 23 (26%) coronary care unit patients (difference 57%, 95% CI 45% to 69%, p < 0.0001) (fig 2)
{kind=link}
{kind=link}
Comparison of numbers of patients from the emergency department (ED) versus the coronary care unit (CCU), with door to needle times in four 30 minute frames.
Pain to thrombolysis time was significantly shorter in the emergency department patients (table 3). In the emergency department group, 18 patients (18%) received thrombolysis within 90 minutes of pain onset, versus one patient in the coronary care unit group (1%) (difference 17%, 95% CI 9% to 25%, p = 0.0001).
There was no significant difference in overall in-hospital mortality between patients treated in the emergency department and the total number treated in the coronary care unit during the study period (12/100 (12%) and 16/180 (9%), respectively; p = 0.5343, 95% CI 5.5% to 27%). However, the case fatality rate was higher in the emergency department patients when they were compared with the prospective coronary care unit group (12/100 (12%)v 3/89 (3.4%); difference 8.4%, 95% CI 2% to 16%, p = 0.021).
Intracranial haemorrhage was confirmed in one emergency department patient and suspected in another, but the clinical course was inconclusive and a necropsy examination was not done. One emergency department patient with aortic dissection secondary to Ehlers–Danlos syndrome received thrombolysis and subsequently died. Significant non-fatal complications of thrombolysis in the emergency department group included three gastrointestinal bleeds and one allergic reaction to streptokinase. In the coronary care unit group there were five gastrointestinal bleeds, one haemoptysis, and one allergic reaction to streptokinase. Inappropriate thrombolysis, defined as a discharge diagnosis other than acute myocardial infarction, occurred in one of the 89 coronary care unit patients and three of the 100 emergency department patients (p > 0.05).
Discussion
Door to needle time is a marker of system efficiency, and a reduced door to needle time should lead to a reduced pain to needle time.9-11 Better patient outcomes, with reductions in the time from symptom onset to the administration of thrombolysis, have been shown by analysing subgroups from large thrombolytic trials.1-4 The GREAT (Grampian Region early anistreplase trial) study and Cocchinelli's study are unique in that they effectively randomised two groups to differing pain to thrombolysis times.13-16 This was done by giving thrombolytic agents to one group at home or in a rural emergency department, and comparing those patients with a second group receiving thrombolytic treatment in an urban coronary care unit. These studies show that reduced pain to needle time significantly improved short and long term outcomes.
In our study, moving thrombolysis to the emergency department was associated with a major reduction in the median door to needle time (from 80 to 37 minutes), with a notable improvement in the numbers of patients treated within the ACHS guideline of 60 minutes (83%v 26%).6 This number is more impressive when it is considered that there were no exclusions in our study, even though the ACHS guidelines suggest including only patients with ST elevation on arrival at the hospital.6 Moreover the reduction in door to needle time translates into a similar reduction in pain to needle time, with a notable increase in early thrombolysis (under 90 minutes, 18% v 1%). There is evidence that very early thrombolysis provides greater benefit in patients with acute myocardial infarction.15-17
There was a median 30 minute delay before the cardiologist was called, similar to the 29 minute delay for emergency physicians to decide on thrombolysis. The coronary care unit group in this study encountered additional delay at two specific phases (fig 1). The first was the time interval between the cardiologist being called and the final decision to give thrombolysis; the second was the delay associated with transferring the patient from the emergency department to the coronary care unit.
These findings suggest that the reduction in door to needle time resulted from a system change and not from faster decision making by the emergency physicians. During the period when thrombolysis shifted from coronary care unit to emergency department there was a significant increase in emergency department doctor staffing numbers and seniority. There is no doubt that an improvement in staffing and seniority of staff in the emergency department could lead to quicker decisions to involve the coronary care unit. However, the decision time in the emergency department was still 30 minutes after the change to emergency department thrombolysis, suggesting that changes in staffing in the department were not the major reason for reduced times. While reduction in door to needle time to 37 minutes is a major improvement, it is probable that this could be reduced further with additional strategies.18 ,19
Because the coronary care unit data were non-consecutive, we retrospectively reviewed the non-registered thrombolysis population to check for potential systematic bias. In these cases the patients were slightly older and had more inferior acute infarcts and longer times to arrival. This probably reflects the fact that these patients were mainly streptokinase recipients, as these tend to be older and have more inferior infarcts. Older patients are also known to present later to hospital. Decisions about thrombolysis in these patients may be more time consuming, given associated factors such as their late presentations and the presence of significant age related comorbidity or relative contraindications. However, we found that their door to needle times were virtually the same as the prospective group and hence systematic bias is unlikely.
We have looked at safety issues for changing the site of delivery. Because of the size of the study it is not possible to prove whether the change is without consequences for safety. There was no overall difference in in-hospital mortality in patients treated in the emergency department compared with the coronary care unit. In the prospective study groups, however, there was an apparent increase in deaths in emergency department treated patients (12%,v 3.4% in the coronary care unit; p = 0.021). Several factors may have contributed to this finding.
First, the overall mortality in the coronary care unit group is calculated to be 9% (table 3; non-significant difference between emergency department and coronary care unit). This may be an underestimate as in the last 22 patients without data some may have been excluded if they had in-hospital infarcts, infarcted late during coronary care unit admission, or infarcted after angioplasty.
Second, both rates are within the range of reported mortality.1 ,2 ,20 ,21 However, the rate in the prospective coronary care unit series is similar to low risk groups from trials, while the emergency department rate is similar to current registry data.22
Third, in the earlier period thrombolysis may have been more conservative. This has been clearly shown in longitudinal studies when new treatments are instituted.23 There was more use of alteplase in the emergency department population. We also reviewed age groups in the two populations and only three of the 89 patients were older than 80 years (two deaths) in the coronary care unit group, versus 11 of 100 in the emergency department population (five deaths). Older patients are known to have a much higher mortality (with or without thrombolysis).24
Fourth, a type I error is possible. The subsequent 100 patients thrombolysed in the emergency department had an in-hospital mortality of 6%.
Fifth, a learning curve for emergency department thrombolysis may be present. Two deaths in the emergency department group were considered errors of judgement (table 4). However, the other 10 cases were considered appropriate.
Clinical details of deaths in prospectively studied emergency department and coronary care unit patients
Sixth, owing to a longer delay to thrombolysis in the coronary care unit group, several patients with early cardiogenic shock or hypotension may have succumbed or become too sick before they could receive thrombolysis. In the emergency department deaths, early signs of cardiogenic shock were seen in five patients within the first few hours.
There was one definite and one possible intracranial bleed in the emergency department group. This is well within the expected rate of intracranial bleeds from other studies.1-3 The proportion of patients misdiagnosed in the emergency department group was 3%, again well within reported rates.1 ,2 ,25 ,26
Reducing door to needle time has been a significant problem for many centres. Strategies other than moving thrombolysis from the coronary care unit to the emergency department have been examined. These have included instituting ECGs and thrombolysis in the prehospital setting,13 ,16 fast tracking patients directly to the coronary care unit from general practitioners and ambulances,27 ,28 and hospitals improving their systems approaches and increasing staff education.29 ,30 In an urban setting such as ours with short transport times, prehospital thrombolysis is unlikely to achieve significant time reductions relative to resource requirements.31 Fast tracking patients falls short in failing to recruit all appropriate patients and leads to patients with non-cardiac diagnoses using coronary care unit beds.25 Also the gains achieved tend to drop off rapidly. The experience in this hospital was that fast tracking reduced times from 80 to 65 minutes but the reduction was unsustainable. Staff education and hospital promotion of thrombolysis tend to lead to short term gains that are easily lost.30 In the present urban teaching hospital setting, moving thrombolysis delivery to the emergency department was a highly effective way of achieving significant and sustainable reductions in door to needle time.
LIMITATIONS
We recognise various potential limitations of this study. First, the study was observational and relied on historical controls, with the possibility that the two populations were very different. However, we feel this is unlikely as the data were collected prospectively and demographic data, pain to door time, and infarct location were similar between the two populations. This suggests that the populations were well matched and were treated similarly. Indeed if there was any bias it would seem to be to the benefit the coronary care unit group, as deaths and patients with later arrival times were found in the non-register population. The hospital had no major change in its catchment population during the time of the study. There was a small change in the numbers of patients coded with a primary ICD-9 discharge code for acute myocardial infarction (1994, 593; 1995, 520; 1997, 483; 1998, 468) and almost no change in the numbers of patients attending the emergency department (35 000 ± 1000); neither have there been any major changes in treatment of acute myocardial infarction offered at this hospital over the study period. Although the percentage of patients given thrombolytic agents acutely was low (about 20% of all patients with a discharge code of acute myocardial infarction), it was similar for the two groups. The only notable difference was an increase in older age groups receiving thrombolysis in the emergency department population and greater use of alteplase. Each could be expected to increase door to needle times.
When the new system was introduced the data collected for the emergency department patients were comprehensive and consecutive to ensure that the quality of the new service was adequate, particularly with regard to safety.
The possibility of ongoing trials leading to delays has been documented in other papers.32 ,33 Patients were recruited to trials during both study periods and in similar numbers, and therefore this was unlikely to bias the results. Moving thrombolysis to the emergency department did not stop recruitment for trials. A possible criticism is that we have not shown a beneficial clinical outcome, but given the numbers of patients available this was never a possibility and was not an aim of the study.
Finally we did not manage to include all patients with thrombolysis in the retrospective coronary care unit review owing to logistical problems. However, most were alteplase patients and the numbers were small. These patients were likely to have larger and more complex infarcts, and in the prospective group had longer door to needle times. It is therefore unlikely that their inclusion would decrease the observed door to needle time and would probably have increased it.
CONCLUSIONS
This prospective observational study has shown that, with a collaborative approach between the emergency department and coronary care unit, delivery of thrombolysis for acute myocardial infarction in the emergency department leads to very important time benefits. The benefit was achieved in a safe manner with diagnostic accuracy and adverse outcomes well within those already reported. We feel that this study, along with trials from other countries, shows that moving thrombolysis to the emergency department is an easy and effective way of reducing and sustaining reductions in door to needle time. This translates to reduced pain to needle times, with likely benefits in terms of mortality and morbidity. In particular, we have demonstrated this in a contemporary Australasian setting.
Acknowledgments
We are grateful to all those who have constructively reviewed and commented on this paper. Their valuable contributions have led to a better paper and we feel the extra effort involved has been worthwhile and productive.