Article Text

Abstract
Objective: To determine the predictors of time between presentation and primary angioplasty and the influence of this delay time on in-hospital mortality in clinical practice.
Design: Analysis of data from the registry of percutaneous coronary interventions in acute myocardial infarction of the Arbeitsgemeinschaft Leitender Kardiologischer Krankenhausärzte (ALKK).
Patients: Data of 4815 patients registered at 80 hospitals between 1994 and 2000 were analysed.
Results: Mean age of the patients was 61.4 (12.5) years. Cardiogenic shock was present in 14.1%. Mean time from admission to primary angioplasty (“door to angiography” time) was 83 (122) minutes. Logistic regression analysis showed the presence of a bundle branch block (odds ratio (OR) 1.95, 95% confidence interval (CI) 1.15 to 3.29), prior coronary artery bypass grafting (OR 1.67, 95% CI 1.08 to 2.59), pre-hospital delay > 3 hours (OR 1.61, 95% CI 1.37 to 1.89), and female sex (OR 1.21, 95% CI 1.01 to 1.45) to be independently associated with longer door to angiography times, whereas a higher hospital volume of performing primary angioplasty (OR 0.53, 95% CI 0.46 to 0.62) and the year of the investigation (OR 0.96, 95% CI 0.92 to 1.00) were independently associated with shorter door to angiography times. Independent predictors of in-hospital mortality were cardiogenic shock (41.6% v 4.0% without cardiogenic shock, p < 0.0001), technical success (29.2% with TIMI (thrombolysis in myocardial infarction) flow < 3 v 6.5% with TIMI flow 3, p < 0.0001), age (16.5% ⩾ 70 years v 6.6% < 70, p < 0.0001), three vessel disease (16.5% v 6.8% with < 3 vessel disease, p < 0.0001), anterior location of infarction (12% v 7.4% without anterior infarction, p < 0.0001), year of inclusion (adjusted OR 0.92 per year, p = 0.011), and volume of primary angioplasty at the hospital (11% for < 20 angioplasty procedures/year v 8.3% for ⩾ 20/year, p = 0.027) but not the door to angiography time (adjusted OR 1.14 per tertile, p = 0.397).
Conclusions: In current clinical practice in Germany median door to angiography time is quite short (83 (122) minutes). Some patients and hospital factors are independently associated with a longer door to angiography time. Within the observed short in-hospital delays door to angiography time did not influence in-hospital mortality. However, efforts to keep them as short as possible should be continued.
- ALKK, Arbeitsgemeinschaft Leitender Kardiologischer Krankenhausärzte
- AMI, acute myocardial infarction
- CI, confidence interval
- NRMI-2, second national registry of myocardial infarction
- OR, odds ratio
- PCI, percutaneous coronary intervention
- STEMI, ST elevation myocardial infarction
- TIMI, thrombolysis in myocardial infarction
- acute myocardial infarction
- door to angiography time
- primary angioplasty
- time to treatment
Statistics from Altmetric.com
- ALKK, Arbeitsgemeinschaft Leitender Kardiologischer Krankenhausärzte
- AMI, acute myocardial infarction
- CI, confidence interval
- NRMI-2, second national registry of myocardial infarction
- OR, odds ratio
- PCI, percutaneous coronary intervention
- STEMI, ST elevation myocardial infarction
- TIMI, thrombolysis in myocardial infarction
In patients with acute ST elevation myocardial infarction (STEMI) reperfusion with primary angioplasty is superior to intravenous thrombolysis regarding in-hospital mortality, repeat infarctions, strokes, and cerebral bleeding.1,2 This difference becomes more pronounced with increasing time from symptom onset to start of reperfusion.3–5
For thrombolysis a clear relation between mortality and time delay between symptom onset and the initiation of thrombolysis has been shown.6–8 In contrast, data concerning the influence of time to treatment with primary angioplasty are conflicting. Most studies have suggested that treatment with primary angioplasty may not be as time dependent as treatment with thrombolysis.3,5,9–12 This difference between primary angioplasty and thrombolysis may result from differences in the time dependent effect on achieving TIMI (thrombolysis in myocardial infarction) grade 3 flow.13 In the case of primary angioplasty there seems to be no major effect of time to treatment on the rate of TIMI grade 3 flow.11,12 However, in the case of thrombolysis, longer times to treatment are associated with lower patency rates. This is more pronounced for streptokinase14 and for urokinase15 than for tissue plasminogen activator, but tissue plasminogen activator also becomes less effective with longer times to treatment.15
An analysis of the NRMI-2 (second national registry of myocardial infarction) data showed, however, that if the treating physician or hospital delays the start of primary angioplasty while the patient is already in the hospital, which is the case with long times from hospital admission until the beginning of primary angioplasty (“door to angiography” time), then longer delays are associated with increasing mortality.10 In contrast a recent analysis of the Zwolle database did not confirm these findings.16
To investigate the predictors of door to angiography times and their influence on primary angioplasty on in-hospital mortality in clinical practice, we analysed data from the Arbeitsgemeinschaft Leitender Kardiologischer Krankenhausärzte (ALKK) registry of percutaneous coronary interventions (PCI) in acute myocardial infarction (AMI).
METHODS
The ALKK registry of PCI in AMI
The PCI registry of the ALKK contains all PCI procedures from 80 centres in Germany since October 1992. Details of the organisation of the registry have been published previously.17 In brief, all interventions were prospectively registered by telephone or fax to the coordinating centre in Kassel, Germany. All complications occurring in the catheter room and during the hospital stay were prospectively documented.
From July 1994 until the end of 2000 a subregistry was opened of all PCI procedures in AMI within 24 hours after symptom onset in more detail than in the general registry.18 Only the procedures from this subregistry were analysed for this report. All data were collected prospectively and analysed centrally.
Definitions
STEMI was diagnosed in the presence of the two following criteria: persistent angina pectoris for ⩾ 20 minutes and ST segment elevation of ⩾ 1 mm in at least two standard leads or ⩾ 2 mm in at least two contiguous precordial leads or the presence of a left bundle branch block. It was later confirmed by the increase of cardiac enzymes of > 3 times the normal upper range. Pre-hospital delay was defined as the time from the onset of symptoms until hospital admission. In-hospital delay (door to angiography time) was defined as the time from admission to the hospital until the start of primary angioplasty (angiographic needle entry). Angioplasty was performed according to the standard protocol of each centre. The physician performing the intervention evaluated the success of primary angioplasty according to the TIMI flow grade.13
Patient selection
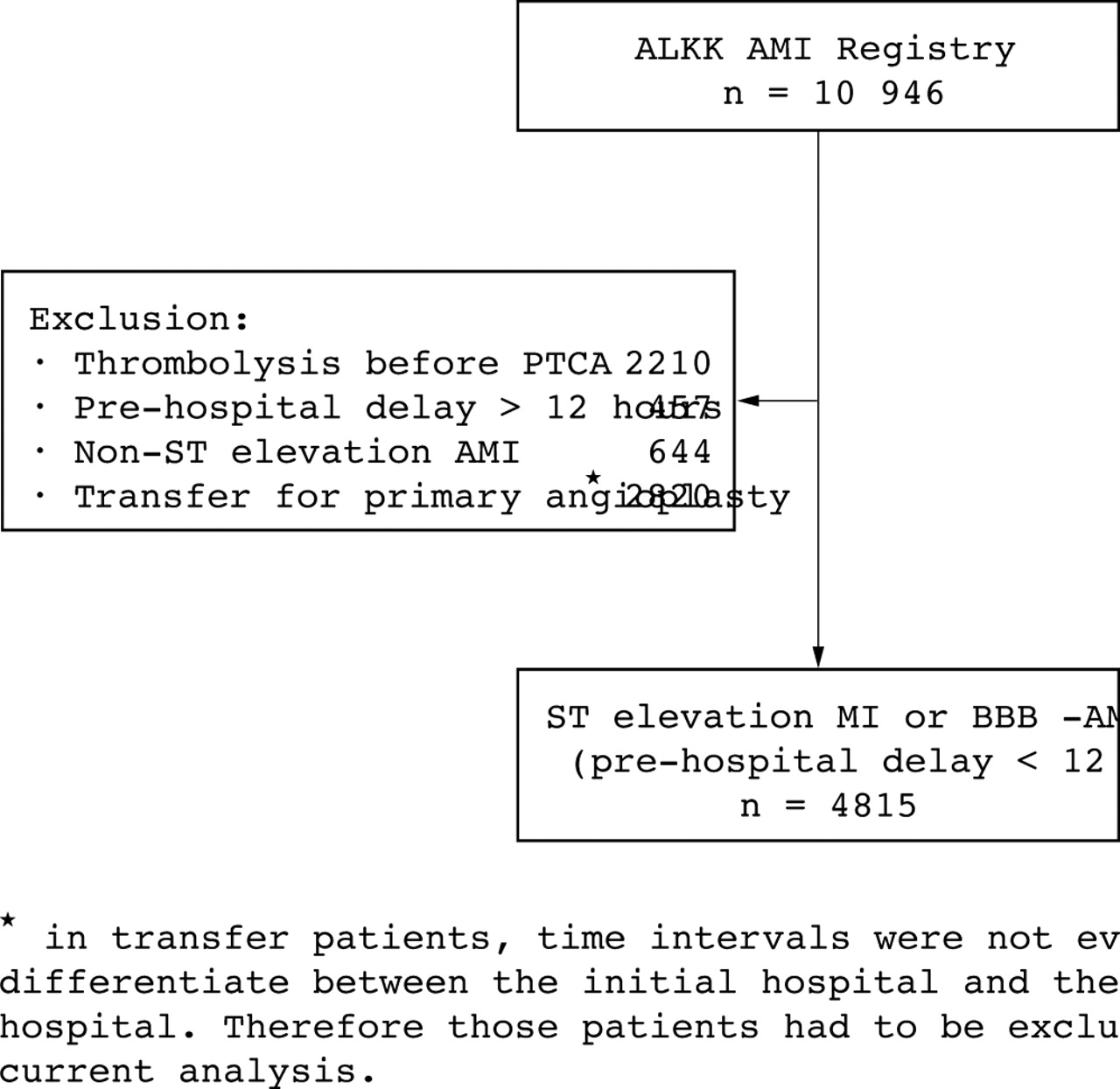
All patients undergoing PCI for STEMI within 12 hours after symptom onset were considered for this analysis. Patients were excluded from this analysis if pre-hospital delay was longer than 12 hours, if patients were treated with thrombolysis before PCI, if patients had a non-STEMI, or if patients were transferred from other hospitals for primary angioplasty (fig 1). Transferred patients were not included because recording of time intervals started with the patient’s admission at the PCI centre and not at the primary hospital.

Selection of patients from the Arbeitsgemeinschaft Leitender Kardiologischer Krankenhausärzte (ALKK) registry of percutaneous coronary interventions in acute myocardial infarction (AMI). BBB, bundle branch block; PTCA, percutaneous transluminal coronary angioplasty.
Statistical analysis
Absolute numbers, percentages, and mean (SD) were computed to describe the patient population. Categorical values were compared by χ2 analysis. Continuous variables were compared by analysis of variance. Door to angiography times were divided into tertiles to investigate angiographic success and in-hospital mortality according to the door to angiography time. Multiple logistic regression analysis was used to adjust for factors influencing door to angiography times and in-hospital mortality. The following variables were examined in the model of door to angiography times: age, sex, location of infarction, cardiogenic shock, previous coronary bypass surgery, presence of a bundle brunch block, pre-hospital delay, volume of primary angioplasty at each hospital, and the year of inclusion. The following variables were examined in the model of in-hospital mortality: age, sex, location of infarction, cardiogenic shock, previous coronary bypass surgery, presence of a bundle brunch block, volume of primary angioplasty at each hospital, year of inclusion, technical success (TIMI 3 flow after primary angioplasty), and tertiles of the door to angiography time. Pre-hospital delay was not included in this model because it was not associated with mortality in univariate analysis. Further logistic regression analyses regarding mortality were done separately for patients with and without cardiogenic shock and after exclusion of technical success from the model. We also compared the mortality rates of patients with a door to angiography time < 120 minutes with those ⩾ 120 minutes. All p values are results of two tailed tests. All statistical calculations were made with the CSS STATISTICA software package from StatSoft, Inc (Tulsa, Oklahoma, USA).
RESULTS
Patients
Between July 1994 and the end of 2000 a total of 10 946 patients from 80 hospitals were entered into the ALKK PCI in AMI registry. Of these patients, 4815 with STEMI were admitted within 12 hours after onset of symptoms primarily to a hospital with PCI facilities and did not receive thrombolysis before angioplasty (fig 1).
Door to angiography times
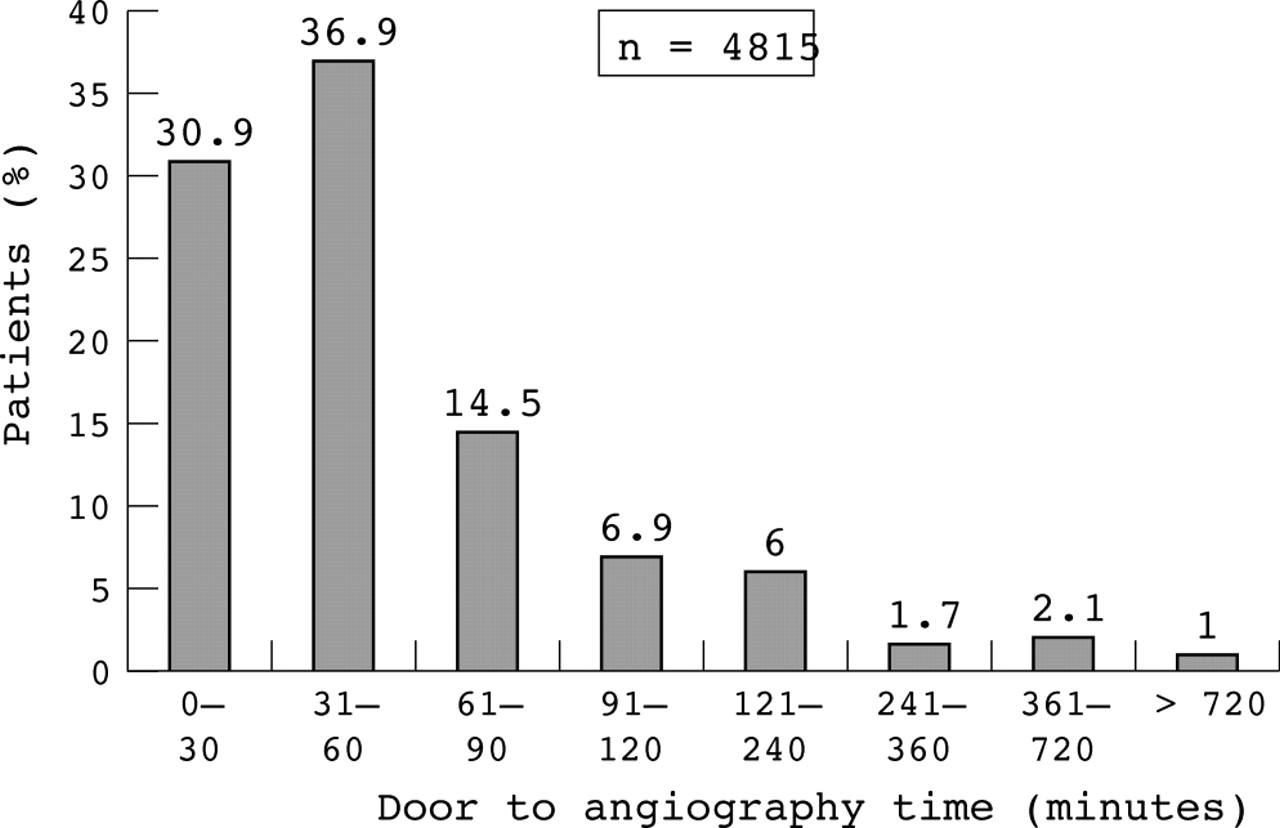
Figure 2 shows the distribution of the door to angiography times. Mean (SD) door to angiography time was 83 (122) minutes. In most patients PCI was started within 60 minutes after admission to the hospital and only a few patients had a door to angiography time exceeding 120 minutes.

Distribution of door to angiography times.
Mean (SD) age of the patients was 61.4 (12.5) years and 25.6% of patients were women (table 1). Cardiogenic shock was present in 14.1%. With increasing in-hospital delay, age increased slightly (p = 0.002) as did the proportion of women (p = 0.025). With longer door to angiography time pre-hospital delays also increased, from 166 (152) minutes (first tertile) to 204 (173) minutes (last tertile, p < 0.0001).
Baseline characteristics and outcome by door to angiography time
Logistic regression analysis showed the presence of a bundle branch block (odds ratio (OR) 1.95, 95% confidence interval (CI) 1.15 to 3.29), prior coronary artery bypass grafting (OR 1.67, 95% CI 1.08 to 2.59), a pre-hospital delay > 3 hours (OR 1.61, 95% CI 1.37 to 1.89), and female sex (OR 1.21, 95% CI 1.01 to 1.45) to be independently associated with longer door to angiography times, whereas a higher hospital volume of performing primary angioplasty (OR 0.53, 95% CI 0.46 to 0.62) and a more recent year of investigation (OR 0.96, 95% CI 0.92 to 1.00) were independently associated with shorter door to angiography times (table 2).
Predictors of door to angiography time >90 minutes
Angiographic success and in-hospital mortality
TIMI grade 3 flow was achieved in 87.5% of all patients. Among patients with door to angiography times < 30 minutes, 89.3% had TIMI grade 3 flow, among patients with door to angiography times between 31–60 minutes 89.0% had TIMI grade 3 flow, and among patients with door to angiography times > 60 minutes 84.1% achieved TIMI grade 3 flow (p = 0.0005). In-hospital mortality was 9.2% with door to angiography times < 30 minutes, 8.3% with door to angiography times between 30–60 minutes, and 10.5% in patients with door to angiography times > 60 minutes (p = 0.552; table 1).
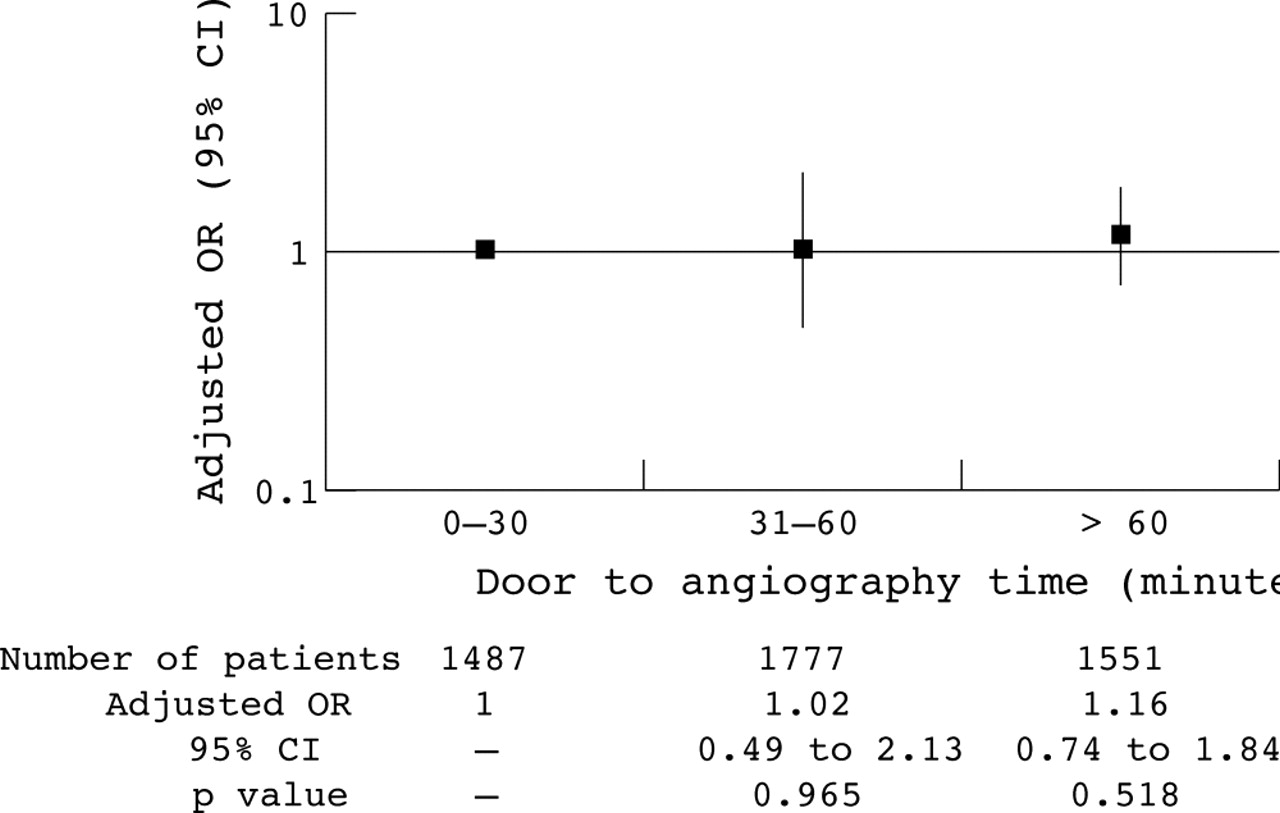
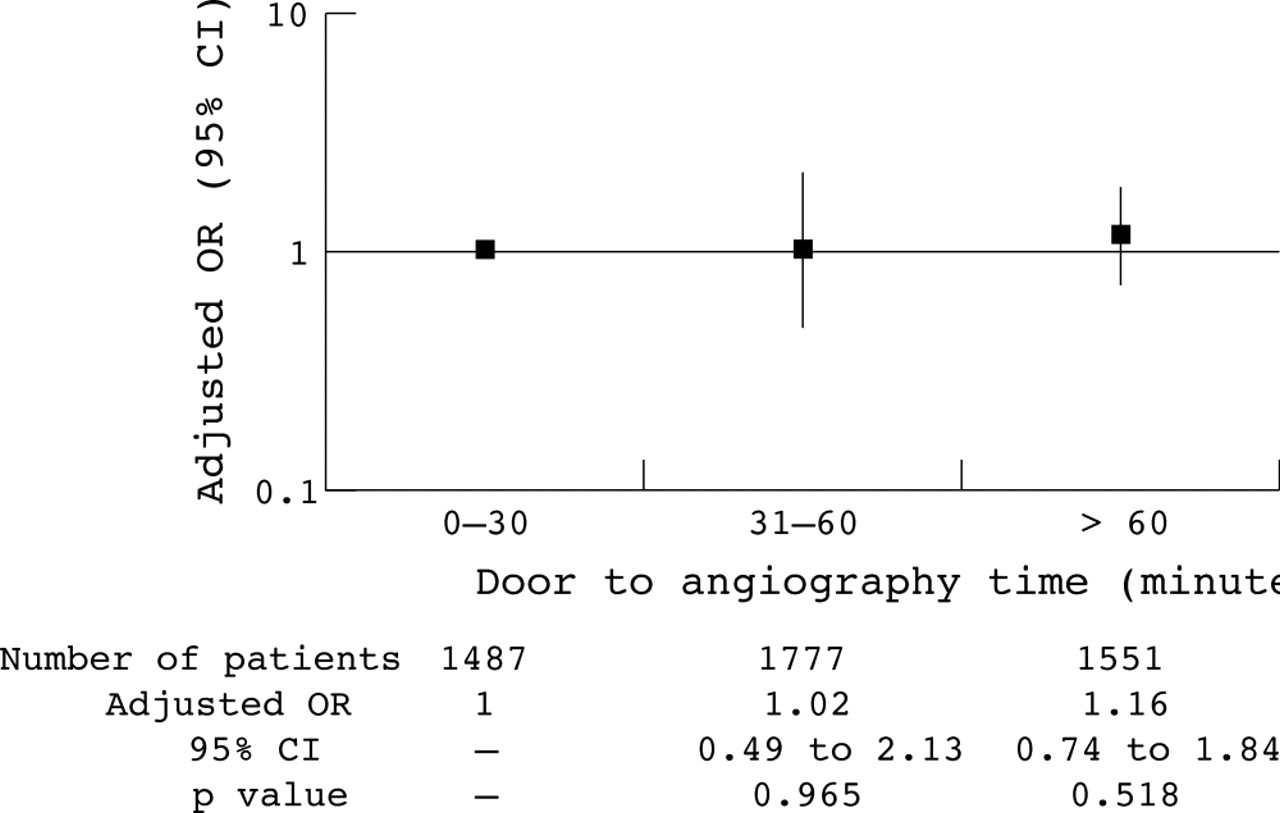
Independent predictors of in-hospital mortality were cardiogenic shock (p < 0.0001), technical success (p < 0.0001), age (p < 0.0001), three vessel disease (p < 0.0001), location of infarction (p < 0.0001), year of inclusion (p = 0.011), and volume of primary angioplasty in each hospital (p = 0.027) but not the door to angiography times (p = 0.397) (table 3). These data did not change substantially if the technical success rate was excluded from the regression model. In-hospital mortality was not significantly lower among patients who started treatment within 30 minutes after admission than among patients treated within 31–60 minutes (OR 1.02, 95% CI 0.49 to 2.13) or later than 60 minutes (OR 1.16, 95% CI 0.74 to 1.84) (fig 3). These data did not change if patients presenting with and without cardiogenic shock were analysed separately.
Predictors of in-hospital mortality
{kind=link}
{kind=link}
{kind=link}
Relation between door to angiography time intervals and mortality. CI, confidence interval; OR, odds ratio.
In-hospital mortality was 12.2% in patients with door to angiography times ⩾ 120 minutes compared with 8.8% in patients with door to angiography times < 120 minutes (p = 0.118, after adjustment for confounding parameters: OR 1.34, 95% CI 0.97 to 1.85, p = 0.098).
DISCUSSION
The data of the ALKK PCI in AMI registry obtained in 80 hospitals in Germany showed a mean door to angiography time of 83 (122) minutes, with only a few patients having a delay exceeding 120 minutes. The presence of a bundle branch block, prior coronary artery bypass grafting, a pre-hospital delay > 3 hours, and female sex were independently associated with longer door to angiography times, whereas a higher hospital volume of performing primary angioplasty (OR 0.53, 95% CI 0.46 to 0.62) and a more recent year of inclusion (OR 0.96, 95% CI 0.92 to 1.00) were independently associated with a shorter door to angiography time. Under these circumstances of short in-hospital delays, we found no influence of the door to angiography time on in-hospital mortality.
Door to angiography times in the ALKK PCI in AMI registry
The observed 50 minute median (quartiles of 31–75 minutes) door to angiography time in our analysis of the ALKK PCI in AMI registry is much shorter than the 116 minute median (quartiles of 95–163 minutes) of the NRMI-2, in which only 8% of patients had a door to balloon time of 60 minutes or less.10 Although obtained at 80 hospitals in Germany these data are very close to the data from the single centre registry in Zwolle (mean 55 (36) minutes door to balloon time).16 Door to angiography time is not door to balloon time, but this difference is usually 10–15 minutes in clinical practice and therefore does not explain the observed large differences in time between the ALKK und the NRMI-2 studies. Door to angiography time may be the more objective way to look at time intervals because it is similar to an intention to treat way to handle primary angioplasty. This becomes obvious in the small group of patients in whom reperfusion cannot be achieved because the obstructed vessel cannot be crossed by a guidewire. No balloon can be used in such circumstances and these patients have a high mortality.18 How such patients were handled in the Zwolle registry is not mentioned16 and there is only one short sentence about this in the NRMI-2 publication.10
Predictors of long door to angiography times
An analysis of the NRMI-2 data by Angeja and colleagues19 described a lot of patient related and hospital related factors being independently associated with longer door to balloon times. These factors are concordant with our findings, especially the finding that door to angiography time increased with increasing pre-hospital delays. This finding may perhaps best be summarised with the notion that if the patient comes late, the doctor does not hurry either. The longer door to balloon times for angioplasty during the night and at low volume hospitals underscore the need for quality control at each hospital.20 The shortened door to angiography times during the last years of the ALKK registry may already be the consequence of the quality control reports of this registry and the increased experience of the centres.
Outcome of long door to angiography times and the paradox of no time dependency of primary angioplasty
The analysis of Cannon and colleagues10 of the NRMI-2 database is the only adequately powered evaluation showing a clear interaction between door to balloon time and in-hospital mortality: increasing door to balloon time was independently associated with increasing in-hospital mortality. Berger and colleagues21 and Juliard and associates22 reported similar results from much smaller patient groups. However, neither the Zwolle data16 nor our data confirmed these results. Both studies found no association between in-hospital delay and mortality. Are these findings really in contrast to the NRMI-2 data? The main difference between the Zwolle and the ALKK data on the one hand and the NRMI-2 data on the other is the in-hospital delay, which was almost twice as long in the NRMI-2 database as in the two other registries. In the NRMI-2 mortality increased significantly only if the door to balloon time increased over 120 minutes, a delay rarely observed at Zwolle or in the ALKK database. Therefore, the conclusion from the Zwolle and the ALKK data is that, if door to angiography time is < 120 minutes in the vast majority of patients, then in-hospital mortality is not significantly influenced by small time differences within this interval. This conclusion is congruent with the data from NRMI-2.
As a result of this, the door to angiography time analysis strongly supports the hypothesis that primary angioplasty is time dependent, if the analysed time delays are long enough. When we compared patients with door to angiography times < 120 minutes with the small proportion of patients with door to angiography times ⩾ 120 minutes, in-hospital mortality was 8.8% versus 12.2% (p = 0.118; after adjustment for confounding parameters, p = 0.098). This hypothesis is also supported by the finding that an increasing time delay to the initiation of primary angioplasty compared with the start of thrombolysis is associated with decreasing superiority of primary angioplasty over thrombolysis.3,23
Is this hypothesis contradicted by the finding in the same study of Cannon and colleagues10 or other data5,24 that there was no association between mortality and increasing symptom onset to balloon time in primary angioplasty? No, because the symptom onset to balloon time is mainly influenced by pre-hospital delay and only in a small part by door to angiography time. Increasing pre-hospital delays are associated with increasing in-hospital mortality only among patients treated with thrombolysis,6–8 not in patients receiving no reperfusion, as shown in the placebo arms of the randomised thrombolysis studies.6 The interaction between in-hospital mortality and pre-hospital delay in thrombolysis is mainly caused by the decreasing effectiveness of thrombolysis to achieve TIMI grade 3 flow with increasing pre-hospital delays,14,15 which is not true for primary angioplasty.11,12 This is also supported by a recent paper of Schömig and colleagues,25 who found a treatment dependent influence of time to treatment interval on myocardial salvage in patients with AMI treated with thrombolysis but not in patients treated with primary angioplasty.
Conclusions
In current clinical practice at a variety of hospitals in Germany median door to angiography time is 50 minutes (quartiles of 31–75 minutes). Several patient and hospital related factors are independently associated with a longer door to angiography time. Although we did not find an influence of door to angiography time on in-hospital mortality within these overall short in-hospital delays, we should continue to keep them as short as possible.
Limitations of the study
Several limitations should be considered. This was an observational study with no randomisation to different door to angiography times. We documented door to angiography time but not door to balloon time, so direct comparison of the in-hospital delays with other registries may be difficult. However, needle to balloon time is usually only 10–15 minutes in clinical practice. Since the number of patients with a door to angiography time > 90 minutes was very low, we could not statistically analyse the long time intervals in detail. Therefore, our analysis reflects the consequences only of small differences in door to angiography times as observed in the ALKK data.