Article Text

Statistics from Altmetric.com
A 64 year old man fell from a ladder directly onto his right foot. Physical examination disclosed a wound on the lateral aspect of the ankle and the midfoot. The talus was completely dislocated and loosely connected to some soft tissue. There were no other apparent injuries except a non-displaced fracture of the fifth metatarsal head. After radiography of the injured area (fig 1A–C), the patient underwent surgery that involved a thorough irrigation of the wound, debridement of avascular skin and soft tissue, and reduction of the talus, followed by fixation by Steinmann pins and primary closure. The leg was placed in a short leg cast (fig 2). His postoperative course was unremarkable, and he was discharged from the hospital with the recommendation to avoid any weight bearing on his right foot. After six weeks, the cast and the pins were removed and weight bearing was gradually resumed. At the one year follow up he continued to complain of ankle and foot pain. On examination the ankle was swollen and painful, and there was limitation of motion at the ankle and the subtalar joints. Radiography showed signs of avascular necrosis of the talus (fig 3). The patient preferred conservative treatment, involving the use of an ankle brace and analgesic medications.
Complete open dislocation of the talus from all its adjacent joints with or without a fracture is a very rare type of injury, with only a few such cases having been described in the literature.1–4 It is usually a consequence of a severe trauma to the foot incurred by a car or motorcycle accident or a fall from height. In some cases the talus is completely disconnected from the foot (“missing talus”).1 Treatment usually involves irrigation, debridement, open reduction, some method of internal fixation, and primary or secondary closure of the wound. Tibiocalcaneal arthrodesis can be performed in cases of a “missing talus”.1 Long term results are variable: some reports describe good results and functional outcome,2–4 while others describe high rates of infection, avascular necrosis of the talus,4 wound healing problems, and prolonged postoperative pain.1 Palomo-Traver et al report that late avascular necrosis or ankle joint arthrosis may be treated by talectomy with or without some form of arthrodesis,2 but Ritsema recommends that talectomy should be avoided.4
Avascular necrosis and infection are the most common complications and they can be anticipated among many of the patients, even if the primary treatment was appropriate. Development of arthrosis in the surrounding joints can cause long term pain and disability, and probably can be treated successfully by conventional methods such as ankle joint arthrodesis or triple arthrodesis.
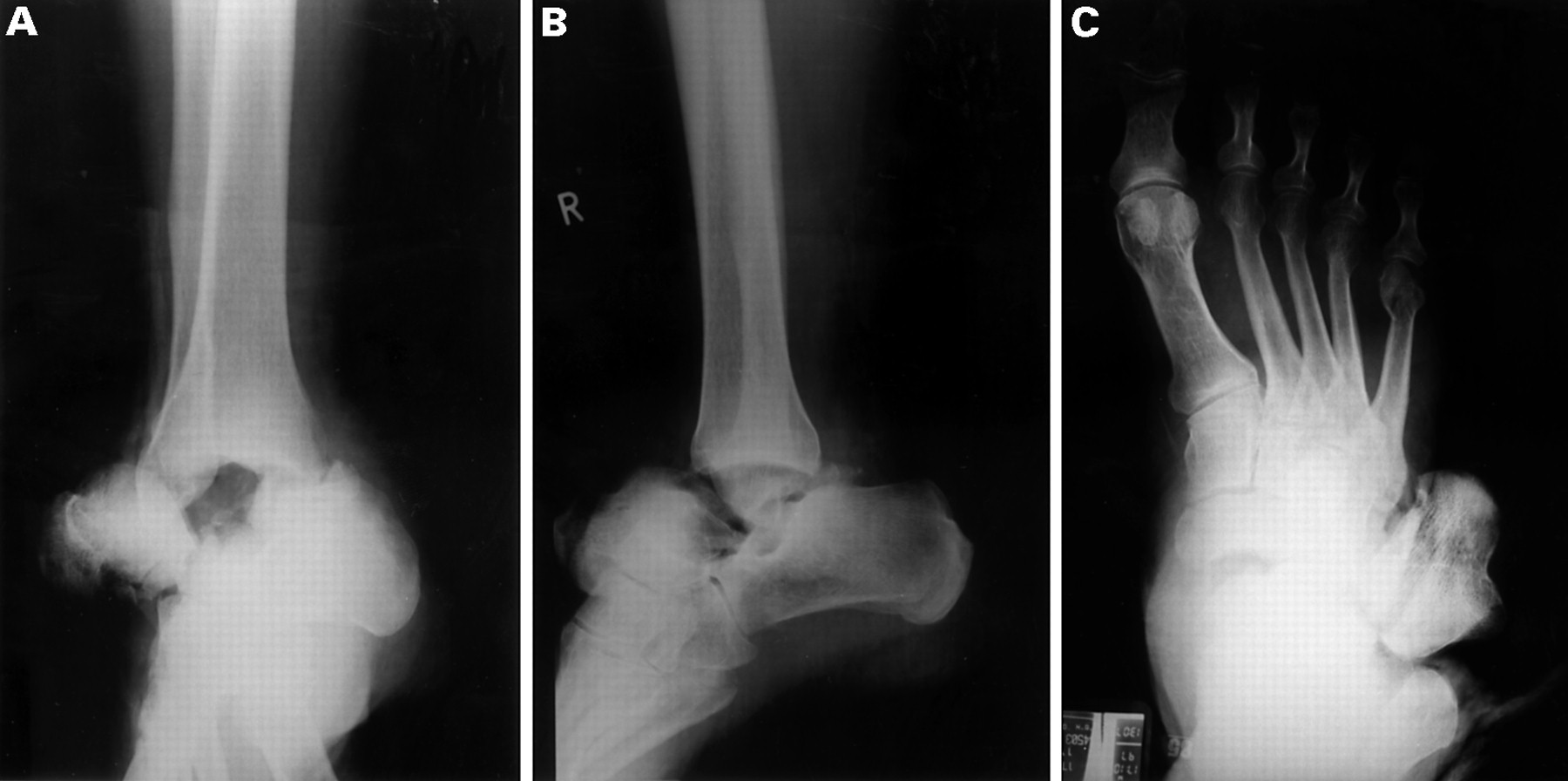
(A)–(C) Anteroposterior and lateral radiographs of the ankle and the foot on admission, demonstrating complete lateral dislocation of the talus and an associated fracture of the fifth metatarsal head.

Postoperative anteroposterior and lateral radiographs of the ankle demonstrating the reduction and internal fixation of the talus.

{kind=link}
{kind=link}
{kind=link}
One year postoperative radiographs demonstrating avascular necrosis of the talar body.