Article Text

Abstract
Objective: A study was undertaken to answer the question: “For those ambulatory patients who attend the emergency department, does routinely measuring their blood pressure and providing written information about hypertension and advising them to see their general practitioner if indicated, compared with no measurement or advice, lead to subsequent interventions (drug therapy, life style advice) to control blood pressure?”
Method: A randomised controlled trial was performed in 400 patients attending the emergency department of Southampton General Hospital, a large UK teaching hospital serving a mainly urban population. Patients were randomised to the intervention and control groups.
Outcome measure: New drug treatment for hypertension at follow-up at 3 and 6 months.
Results: No new antihypertensive drug treatment was started for any of the participants (n = 377) in the trial.
Conclusion: Although screening was successfully completed, no differences were seen between the intervention and control groups. The high level of blood pressure screening within primary care became evident as the trial progressed. This, combined with the fact that the trial was limited to patients registered with a general practitioner, possible expectation bias in control subjects and poor compliance with follow-up instructions, may explain the result.
Statistics from Altmetric.com
Hypertension is a major modifiable contributory factor in cardiovascular diseases such as stroke and coronary heart disease.1 Population-based studies have confirmed that hypertension leads to a 2–3-fold increase in the risk of various cardiovascular consequences.2 For individuals aged 40–70 years, each increment of 20 mm Hg in systolic blood pressure or 10 mm Hg in diastolic blood pressure doubles the risk of cardiovascular disease events independent of other factors.3 Yet uncomplicated hypertension can only be detected by measurement. Thus, screening for hypertension is widely accepted as beneficial and is part of governmental targets for “The Health of the Nation”, seeking a 40% reduction in death rates from stroke, coronary heart disease and related disease in people under 75 years by 2010.4
The emergency department (ED) could potentially represent a suitable setting for the screening of disease and hypertension in particular for the following reasons:
Certain groups may be infrequent users of primary care and their visit to the ED represents an opportunity for screening. According to Fleming et al,5 one-third of attendees at one central London teaching hospital viewed the ED as their main source of primary care.
Blood pressure readings are routine, can be automated and could easily be undertaken in the ED setting.
Screening could be undertaken while the patient is waiting or just after their care is completed.
Possible disadvantages to such activity include:
Diversion of resources to undertake activity that is already commissioned elsewhere. Indeed, Lee6 states that EDs do not have a duty or the resources to universally screen for asymptomatic chronic conditions, and he reflects the concern of many emergency physicians.
These patients will still need to be followed up. Who would do this and would the patient comply?
Would the benefits be worth the effort?
Studies from North America suggest that screening for hypertension in the ED is worthwhile.7–9 In this population there are significant numbers of patients with unrecognised hypertension that are subsequently treated once identified in the ED.7 8 Approximately 20% of North American ED patients are hypertensive and only one-third of these are receiving treatment.9 In the UK, Fleming et al5 studied an inner city population and found that 29% of patients were hypertensive. There have been concerns that hypertension identified in the ED may be raised transiently because of pain and anxiety. However, a recent review concluded that hypertension identified in the ED persists in a significant proportion of patients after they leave the ED,10 and this is supported by Fleming et al5 who found that, of those initially found to be hypertensive, 75% of those who returned for follow-up remained so. Thus, screening for hypertension in the ED may capture a significant group who evade screening (size unknown) and who, if hypertensive in the ED, may remain so.
Our research question is: For those ambulatory patients who attend the ED (patient group), does routinely measuring their blood pressure and providing written information about hypertension and advising them to see their general practitioner if indicated (intervention), compared with nothing, lead to subsequent interventions (life style advice, new drugs) to control blood pressure? The primary outcome measure was new drug treatment for hypertension at 3 and 6 months follow-up.
This study presented the opportunity to undertake a pragmatic study (set within a busy department and referring patients on to their general practitioners for follow-up), exploring the role of screening within the ED, which is not seen as a traditional role for EDs in the UK but is advocated by other countries.11 At the time the study was commissioned in 2004, all previous literature relating to hypertension screening in the ED was North American and the frequency data of screening for hypertension locally within primary care was unavailable.
METHODS
Study design
A randomised controlled trial was performed in the ED of Southampton General Hospital between October 2005 and August 2006. The hospital serves a mainly urban population of 0.5 million and is a teaching hospital. The inclusion criteria were as follows:
Age >35 years (the frequency of hypertension is very low below this age).
Ambulatory patients going to be discharged from the ED.
Patients who had not had their blood pressure measured for other reasons (as we did not want to interfere with the normal departmental practice for these patients).
Patients had to be registered with a general practitioner in the Southampton area because the follow-up and possible treatment of hypertension would be provided by the general practitioner. However, this would mean that those who were not registered would be excluded. One study5 suggested that one-third of patients (17/51) who were hypertensive at ED presentation and who attended follow-up were in this category.
Patients must not be under the influence of alcohol or drugs.
Patients must be contactable by telephone.
Patients with poor comprehension of English or who were pregnant were excluded from the study.
Recruitment of patients
A research nurse (KC) who worked on the ambulatory side of the department (typically weekdays during office hours) was dedicated to recruiting patients. Patients who might be eligible were provided with an information sheet detailing what hypertension is, how it is treated and a written and verbal explanation of the trial. Consent to participate in the trial was sought. After they had completed their ED treatment, those who consented were asked to sit quietly for 5 min during which time they completed a questionnaire which asked about age, sex, risk factors for cardiovascular disease, whether the patient was known to be hypertensive, whether they were having treatment (advice/life style/drugs), when they last had their blood pressure measured and confirmation that they agreed to a telephone follow-up 3 and 6 months later. Those who were approached who did not want to participate in the trial but did want to have their blood pressure measured were offered measurement and advice and their frequency was recorded. Randomisation was by the use of a random numbers table and the allocation concealed in an opaque envelope with a trial number recorded on it. Consenting patients were then allocated to either the intervention or control group.
Those in the intervention group had their blood pressure measured in both arms while sitting using an automated and appropriately calibrated machine and cuff (Marquette DASH 3000 patient monitor). The time interval between the two blood pressure measurements was >2 min. The evidence suggests that, within the ED, two blood pressure measurements taken >2 min apart are adequate for screening purposes.10
The patients were told of the highest of the two readings which were used to classify them into the following six categories according to the British Hypertensive Society guidelines:12
>220/120: immediate treatment
180–219/110/119: general practice follow-up in 1 week
160–179/100–109: general practice follow-up in 2 weeks
140–159/90–99: general practice follow-up in 4 weeks
130–139/85–89: general practice follow-up in 1 year
<130/85: general practice follow-up in 5 years
A letter was sent to the general practitioner that explained the basis of the study, the patient’s blood pressure reading and the follow-up advice given. An advisory booklet entitled “Blood pressure” published by the British Heart Foundation13 was given to each patient. They were asked to record subsequent blood pressure measurements, advice given and any new antihypertensive medication that had been started using a dedicated proforma attached to the booklet which also recorded when the follow-up telephone calls (at 3 and 6 months) would occur.
The control group did not have their blood pressure measured nor were they provided with written advice, but they were contacted by telephone at 3 and 6 months. A letter was sent to their general practitioner explaining that they had participated in the study but had not had their blood pressure measured.
Those who agreed to participate but then wished to move from the control to the experimental group or vice versa were analysed in the group to which they were originally allocated.
Outcomes
Both groups were contacted at 3 and 6 months by telephone and a questionnaire was administered by the investigator who was blinded as to the group to which the patient had been allocated. The following questions were asked:
Were you asked to have your blood pressure remeasured?
If so, what was it?
What advice were you given?
Are you on any new medication?
What is it?
Is the medication for control of your blood pressure?
Sample size calculation
If the primary outcome is new drug treatment for hypertension and it is assumed that 20% of those patients attending the ED are hypertensive and, of these, one-third have drug treatment (7%),9 and if it is agreed that it would be clinically worthwhile to double this rate (15%), then 187 patients would be required for each arm of the trial.
Analysis of data
χ2 tests were used to compare the two groups.
RESULTS
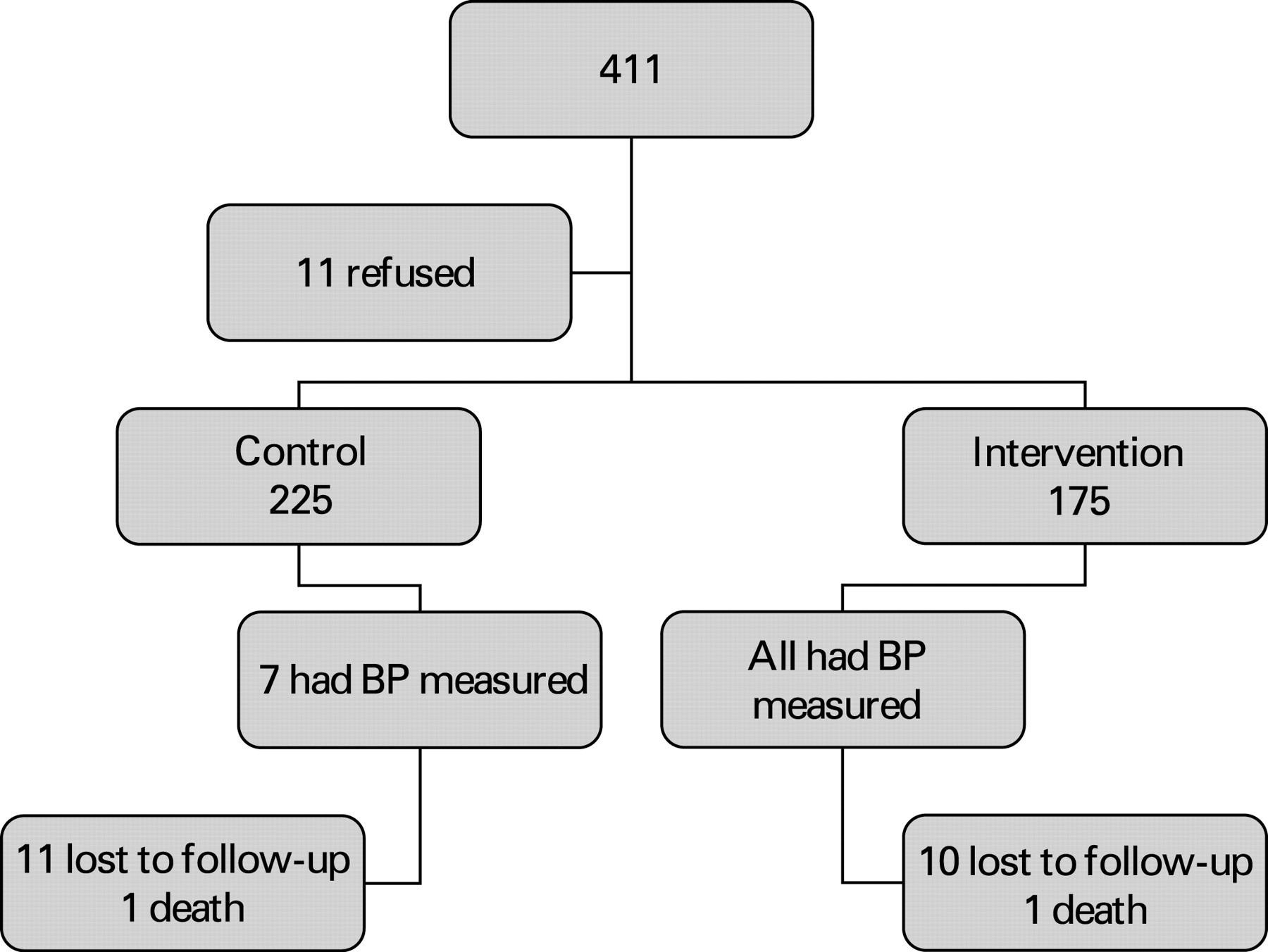
Figure 1 shows the flow of patients through the trial. Eleven patients who were approached refused to participate in the study and the remaining 400 were randomised to the control and intervention groups. The baseline characteristics of the two groups are shown in table 1. By follow-up at 3 months, 10 patients in the intervention group could not be contacted and 1 patient had died, leaving 164 patients in this group. In the control group 11 could not be contacted and 1 patient had died, leaving 213 patients in this group.

{kind=link}
Table 2 shows stratification of the control and intervention groups according to whether or not they were known to be hypertensive and by blood pressure reading at the time of recruitment. Seven patients in the control group wished to have their blood pressure measured and, when they did so, they remained in the control group. Patients who had their blood pressure measured again and recorded at 3 and 6 months are shown in table 2.
At the 3 month follow-up, 26/213 in the control group had a follow-up blood pressure measurement and four new patients with hypertension were identified, none of whom were given new drugs or advice. In the intervention group 34 patients had their blood pressure measured again. Only 15 of the original 47 who had blood pressure >140/80 complied with the advice given in the ED (ie, some patients with blood pressure <140/80 had their blood pressure rechecked). Indeed, only 6/23 of those with blood pressure >140/80 not previously known to be hypertensive were followed up. No patients had new additional antihypertensive drug treatment and only three patients had life style advice.
At the 6 month follow-up (including all those contacted at 3 months), 10/175 in the intervention group had their blood pressure measured compared with 5/213 in the control group. No new drug treatments were added and only two patients received life style advice.
DISCUSSION
It is surprising that there was no difference between the groups. However, the high level of surveillance (90% had had their blood pressure measured in the previous 5 years) and levels of treatment (25% were taking cardiac drugs), not known at the inception of the study despite inquiry, limited the population that might benefit from ED screening. Excluding patients not registered with a general practitioner may also have excluded a population that had not been screened by primary care and would have benefited from ED screening. However, it was essential that the recruited patients who needed follow-up were registered, and it was considered unreasonable to expect general practitioners to commit to the care of patients not previously in their care. The control group had to be aware of the trial in order to give consent and were free to do as they wished when they left. It is likely that, by being recruited to the study, they were sensitised to the issue of hypertension and this led to an expectation bias that they should get their blood pressure measured, which 26/213 did. All of these factors will have reduced any differences between the groups.
CONCLUSION
Although 1 in 10 patients in the intervention group had a blood pressure reading of >140/80, the high level of existing screening and treatment together with the poor compliance of patients to keep to follow-up plans meant that there was no difference between the groups in terms of drug treatment for hypertension. Screening for hypertension in the ED for this population was ineffective.
Acknowledgments
The authors thank Boehringer Ingleheim for making funding available to the College of Emergency Medicine who independently made this award and the British Heart Foundation for provision of the hypertension booklets.
REFERENCES
Footnotes
KC recruited the patients, measured their blood pressure and carried out the telephone follow-up. SG helped with the design, ethical approval, analysis and writing up of the trial. MC initiated the project, secured funding and helped with the design, analysis and write up.
Funding: Boehringer Ingleheim made funding available to the College of Emergency Medicine who independently made this award.
Competing interests: None.
Ethics approval: Ethical approval was sought and given in August 2005.
Linked Articles
- Primary survey