Article Text

Abstract
Background Many previous studies have shown that patients admitted to hospital at weekends have worse outcomes than those on other days. It has been proposed that parity of clinical services throughout the week could mitigate the ‘weekend effect’. This study aimed to determine whether or not a weekend effect is observed within an all-hours consultant-led major trauma service.
Methods We undertook an observational cohort study using data submitted by all 22 major trauma centres (MTCs) in England to the Trauma Audit & Research Network. The inclusion criteria were all major trauma patients admitted for at least 3 days, admitted to a high-dependency area, or deceased following arrival at hospital. Patients with Injury Severity Score (ISS) >15 were also analysed separately. The outcome measures were length of stay, in-hospital mortality and Glasgow Outcome Score (GOS). Secondary transfer of patients between hospitals was also included as a process outcome.
Results There were 49 070 patients, 22 248 (45.3%) of which had an ISS >15. Within multivariable logistic regression models, odds of secondary transfer into an MTC were higher at night (adjusted OR 2.05, 95% CI 1.93 to 2.19) but not during the day at weekends (1.09, 0.99 to 1.19). Neither admission at night nor at the weekend was associated with increased length of stay, worse GOS or higher odds of in-hospital death. These findings remained stable when confining analyses to the most severely injured patients (ISS >15), excluding transferred patients, and using a single mid-week (Wednesday) baseline.
Conclusions After adjustment for known confounders the weekend effect is not detectable within a regionalised major trauma service.
- major trauma management
- Trauma
- Trauma, epidemiology
Statistics from Altmetric.com
Key messages
What is already known on this subject?
Increased mortality for patients admitted at weekends has been demonstrated across many disease populations and healthcare systems. The reasons for this ‘weekend effect’ are unclear but could include differences in patient case mix, coding practice, or the availability of hospital resources at weekends. A weekend effect has previously been shown for major trauma patients in the USA, although the effect was smallest in the highest-level trauma centres.
What might this study adds?
This study found no evidence of increased mortality for patients admitted at night or during the weekend. It is important to identify populations that do not exhibit outcome differences at weekends in order to understand the nature of the weekend effect, and whether it can be modified by restructuring healthcare services.
Introduction
Increased mortality for patients admitted at the weekend was first shown in Canadian hospitals in 2001.1 The ‘weekend effect’ has since been explored by over 100 studies and described in both elective and emergency populations.2 ,3 Worse outcomes have been shown for patients admitted at the weekend in the setting of acute stroke,4 myocardial infarction,5 pulmonary embolism,6 lower extremity ischaemia,7 emergency general surgery,8 paediatric neurosurgery,9 cosmetic surgery10 and elective joint replacement.11 Increased weekend mortality has even been recognised in the palliative care setting.12
The ‘weekend effect’ has been observed in many different patient groups and healthcare systems.13 However, the reasons for this phenomenon are unclear and a number of explanations have been proposed. One possibility is that it simply reflects inadequate risk adjustment by large observational studies as patient case mix can vary at the weekend.14 ,15 However, the weekend effect persists in emergency populations4–9 and it is unclear why these patients should vary substantially by day of the week. There have also been attempts to eliminate the effect by adjusting for patient characteristics, which have mitigated the weekend effect to varying degrees.2 ,3 A second possibility is that the weekend effect is an artefact of systematic miscoding in administrative datasets. For example, it has been proposed that the weekend effect can be eliminated by studies that only analyse high-quality data, for example, from clinical registries.16 ,17 Finally, an alternative explanation is that the delivery of healthcare services varies at the weekend to the detriment of patients. This has prompted a vigorous debate in the UK about how best to provide equivalent services to NHS patients seven days per week.18
Since April 2012, major trauma services across England have been organised into inclusive trauma networks. Within these networks, severely injured patients are triaged directly to regional hospitals that have been designated as major trauma centres (MTCs). English MTCs were designated by the Department of Health following a national assessment of clinical capabilities and population needs. They are broadly comparable to Level 1 and 2 trauma centres in the USA.19 ,20 Major trauma patients treated at MTCs are usually met on arrival by a trauma team led by a consultant-grade doctor regardless of the time or day of presentation. All further resources necessary for the management of patients with multiple injuries (including CT scanning, subspecialty expertise and an emergency operating theatre) should also be available at all hours.20 The trauma networks were funded with an additional investment of £37 million to support a ‘payment by results’ model of hospital remuneration.19 This rewards MTCs for meeting a number of quality standards, including the initial assessment of major trauma patients being led by a consultant-grade doctor. In the post-reconfiguration period, major trauma in England represents the first truly all-hours specialty service in the NHS. Worse outcomes for major trauma patients admitted at weekends might suggest that the weekend effect is not readily amenable to mitigation by reorganising NHS services.
This study used a comprehensive national trauma registry to explore whether weekend admission is associated with worse outcomes for severely injured patients treated in MTCs.
Methods
Data source
The Trauma Audit & Research Network (TARN) collects data from all hospitals that manage severely injured patients in England. MTCs are paid for meeting specific performance criteria under the Major Trauma Best Practice Tariff (BPT), which includes a submission to TARN within 25 days of patient discharge or death.21 Most MTCs employ a dedicated data coordinator for the purposes of managing TARN submissions. This process ensures that TARN captures the overwhelming majority of eligible patients admitted to the MTCs. Data completeness is estimated using data on trauma admissions (ICD10 diagnosis S00-T75) from Hospital Episode Statistics (HES). During the study period, data completeness was estimated at 105.1%, which means that more cases were reported to TARN than were found using appropriate diagnostic codes in HES. As TARN is a clinical registry, all variables identified as necessary for optimal risk adjustment are collected prospectively.
The inclusion criteria for TARN are all patients with a severe injury that were admitted for at least 3 days, required high-dependency care or died following arrival at hospital. Severe injuries are defined by the TARN procedure manual but exclude isolated hip fractures in patients aged ≥65 years.
Participants
All cases within TARN were included, including paediatric presentations. The major trauma lead clinician at each MTC was contacted to determine the date on which their hospital was fully functional within the terms of the major trauma service reconfiguration. Cases were only included from each hospital after they were fully operational as an MTC. The London trauma network was established in 2010 and many of the MTCs throughout the rest of England went live in April 2012. The complete list of MTC launch dates used in this analysis has been described elsewhere.22
Earlier cases were not included as reporting to TARN improved substantially following introduction of the Major Trauma BPT.21 Although the nature of services provided before reconfiguration are unknown (and likely variable), major trauma services were consistently resourced in the postimplementation period.
Variables and outcome measures
Hypotension was defined as a systolic BP (SBP) ≤90 mm Hg and tachycardia as a heart rate ≥100 bpm. ‘Day’ was defined as 08:00–17:00 hours and ‘night’ as 17:00 until 08:00 hours the following day. The weekend was defined as Saturday and Sunday.
The Injury Severity Score (ISS) is calculated from Abbreviated Injury Scale (AIS) scores, which are values reproducibly assigned by trained coders within the TARN co-ordination centre. The AIS codes are based on the severity of injuries sustained in each body region (as detailed by imaging, operative and autopsy reports). The Charlson Comorbidity Index (CCI) provides a weighted score from 22 comorbid diagnoses and is the mostly commonly used comorbidity measure in observational studies.
The outcome measures were in-hospital mortality, length of stay and Glasgow Outcome Score (GOS). Secondary transfer of patients into MTCs was also included as a process indicator as it could highlight weekend differences in effectiveness of prehospital triage or the ability of non-MTCs to definitively manage severely injured patients. Length of stay was only calculated for patients discharged alive from hospital to avoid downward bias of this measure. The GOS is a five-point disability score through ‘good recovery’ (return to normal life), ‘moderate disability’ (some impairment but living independently), ‘severe disability’ (dependent on daily care), ‘persistent vegetative state’ and ‘death’.
Statistical analysis
Unpaired t-tests were performed for normally distributed continuous data and Mann-Whitney U-tests for non-normally distributed data. Right-skewed length-of-stay data were subject to the Bonnet-Price test for difference between two medians.23 χ2 tests with Yates' correction for continuity were used for categorical variables. Associations between time of presentation and outcomes were explored using multivariable logistic (secondary hospital transfer, in-hospital mortality, GOS) regression and log-linked gamma family generalised linear models (length of stay (LOS)). The covariates were age, sex, ISS, GCS and CCI. As there were only small numbers of patients in some GOS categories (eg, ‘persistent vegetative state’), this was included in the logistic regression models as a categorical variable, that is, ‘good recovery’ versus all other recorded GOS outcomes. ISS was transformed into a functional form to correct for non-linearity in the relationship between continuous variables and outcome.24
The principal analyses directly compared weekday versus weekend day and weeknight versus weekend night. Subgroup analyses were planned a priori for patients with ISS >15, which is conventionally used as the critical threshold for ‘major trauma’.25 As secondary transfer patterns could vary within and outside normal working hours, we planned a sensitivity analysis that excluded patients transferred into MTCs.
Standardised risk-adjusted excess survival rates (Ws) were calculated for groups of patients based on their admission time category. Ws is a standardised W statistic that is calculated as ((survivors—expected survivors)/total patients)×100.26 Expected survival is determined using survival probability as predicted by the risk adjustment model used by TARN for performance benchmarking of individual hospitals. This model has been validated prospectively and shown to have excellent predictive value for mortality at 30 days.27 SAS (Cary, North Carolina) was used for all statistical analyses and p<0.05 selected as the threshold for statistical significance.
The study protocol was developed in full before any statistical analyses were undertaken. The only post hoc decisions were to use generalised linear models instead of multiple linear models to analyse LOS data (because of right skew), to analyse GOS as a binary outcome (because of inconclusive multinomial regression), and to report sensitivity analyses using (i) a Wednesday baseline to support comparison with other recent studies and (ii) a mixed-effects model adjusting for clustering within centres.
Results
There were 49 070 cases submitted to TARN, 22 248 (45.3%) of whom had an ISS >15. These included 20 711 patients presented during the working day (weekday 14 711 (71.0%) and weekend day 6000 (29.0%)) and 28 359 at night (weeknight 15 799 (55.7%) and weekend night 12 560 (44.3%)). The most severely injured body regions were limbs (28.4%), head (28.2%), chest (15.4%), spine (10.9%), multiple (10.7%), abdomen (3.7%) and other (2.6%). Table 1 shows the differences in case mix between the time periods.
Characteristics of TARN patients by time of presentation
Secondary transfer
Table 2 shows that a greater proportion of patients were transferred from other hospitals at night, both during the week (weekday 15.0% vs weeknight 27.1%, p<0.001) and at weekends (weekend day 21.6% vs weekend night 32.2%, p<0.001). Secondary transfer rates were modestly increased at weekends (weekday 15.0% vs weekend day 16.2%, p=0.029). Table 3 shows that a similar pattern was observed for severely injured patients arriving at night (day 20.5% vs night 32.2%, p<0.001) but that secondary transfer was not associated with weekend admission in this subgroup (weekday 20.0% vs weekend day 21.6%, p=0.110).
Outcomes for TARN patients by time of presentation
Outcomes for patients with ISS >15 by time of presentation
In the adjusted analysis, patients had higher odds of transfer into an MTC if they were injured at night (adjusted OR (aOR) 2.05, 95% CI 1.93 to 2.19) but not during the day at weekends (weekend day aOR 1.09, 0.99 to 1.19) compared with admission during the day in the week (table 4). The same finding was observed within the ISS ≥15 subgroup (weekend day aOR 1.09, 95% CI 0.96 to 1.23; weekend night 1.83, 1.67 to 2.00; weeknight 1.92, 1.76 to 2.09).
Adjusted outcomes for patients by time of presentation*
Length of stay
Table 2 shows that length of stay was the same for patients admitted during the day at weekends than during the week (weekend day median 9 (IQR 5–18) vs 95–18 days, p=1.00). However, patients admitted during the night at weekends had a shorter length of stay than those in the week (weeknights 85–17 vs 95–17 weekend nights, p<0.001). Table 4 shows that the only significant differences within generalised linear models were that patients admitted at night had a shorter length stay relative to those admitted during the day. However, these differences are unlikely to be clinically significant. The full model is available as online supplementary table S1.
Supplementary tables
Mortality
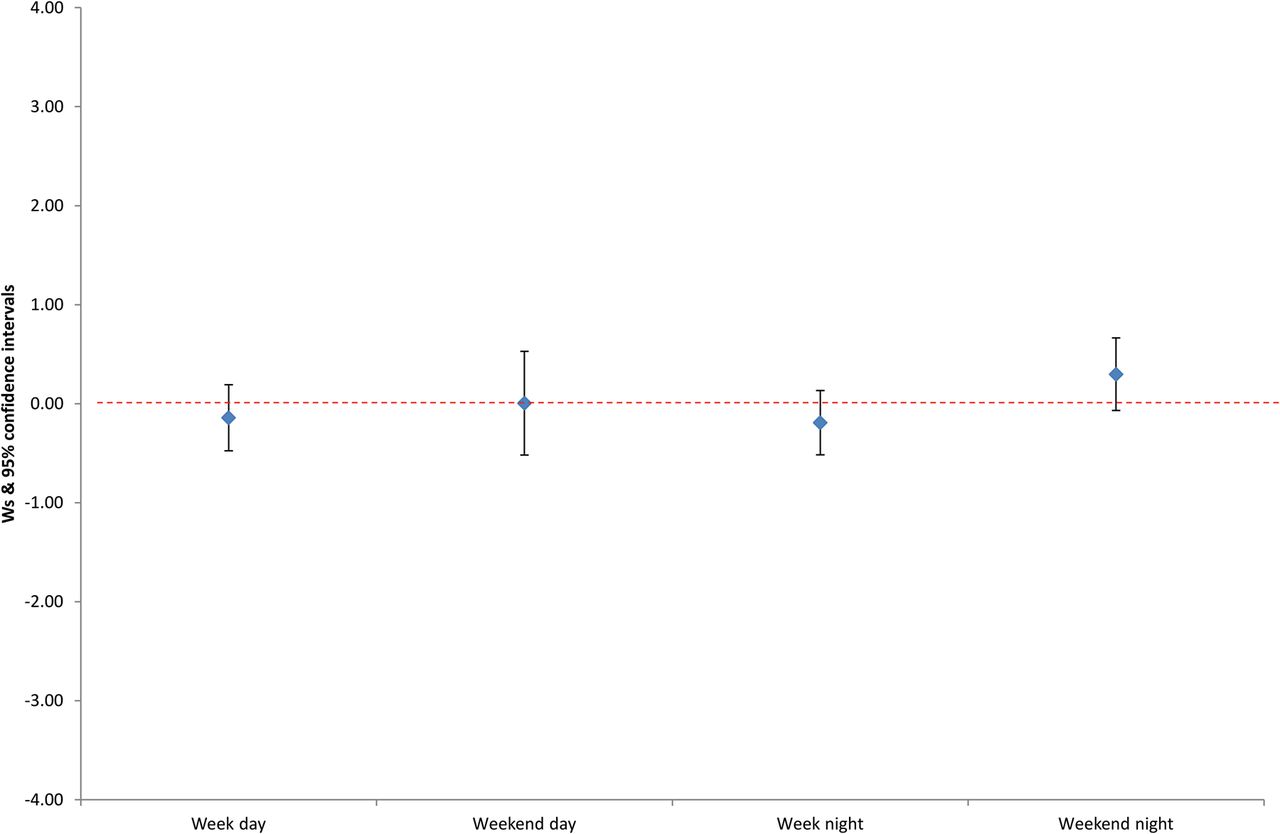
There were not any significant mortality differences between groups within the whole TARN cohort, either in unadjusted (tables 2 and 3) or adjusted analyses (see table 4 and online supplementary table S2). Figure 1 shows that there were not any significant differences in standardised risk-adjusted excess survival rates (Ws) between the admission categories. A number of exploratory analyses were undertaken to test the effect of specific methodological decisions taken during this study. There was no detectable weekend effect in mortality when the logistic regression model was substituted for a mixed-effects model with random intercept to adjust for clustering (see online supplementary table S3) or when a midweek (ie, Wednesday) reference was selected (see online supplementary table S4).
{kind=link}
Standardised risk-adjusted excess survival rates (Ws) for major trauma patients by admission category.
The logistic regression mortality models showed excellent (area under receiver operating characteristic curve or c statistic ≥0.90) predictive value for mortality. The coefficients and diagnostics for each of these models are provided in online supplementary tables S2–4.
Glasgow outcome score
Tables 2⇑–4 and online supplementary table S5 show that there were not any differences in the proportion of patients with a GOS of ‘good recovery’ in any of the analyses.
Sensitivity analysis
There were no significant differences in adjusted length of stay, mortality or GOS between the groups when transferred patients were excluded. There were also not any residual associations between outcome and time of presentation in the ISS >15 subgroup (table 4).
Discussion
The ‘weekend effect’ has been so consistently reported across different patient populations and healthcare systems2–12 that it has been described as ‘ubiquitous’.13 The finding of increased mortality for patients admitted at weekends has prompted discussion about expanding 7-day NHS services and whether doctors' working patterns could be changed to improve weekend outcomes. As NHS major trauma services provide a relatively consistent service regardless of time or day of admission, it is important to understand whether they are also associated with increased weekend mortality.
Beginning in April 2012, major trauma services across England were reconfigured into a series of regional trauma networks. These networks are based on MTCs, which are financially remunerated for meeting defined quality standards, including the availability of a consultant trauma team leader, CT scanning and an emergency operating theatre.20 Although there might still be variability in the provision of allied subspecialty services, the reconfigured major trauma system represents the first truly all-hours service in the NHS. Other regionalised services (eg, for acute stroke and ST-elevation myocardial infarction) also provide augmented services out of hours, although they do not specify that patients must be assessed on arrival by a consultant.
Our study did not find evidence of a weekend effect for injured patients treated within English MTCs. This is contrary to US evidence that patients admitted at night are 1.18 times more likely to die than those presenting within working hours.28 However, it is consistent with studies from other large regional hospitals that did not find increased mortality for trauma patients at weekends.29 ,30 Importantly, the US study reported that the weekend effect was weakest in level 1 (ie, the highest level) trauma centres.28 Previous studies have suggested that the weekend effect can be explained by reduced staffing levels,31 use of temporary clinical staff32 and reduced access to some investigations and procedures.33 The weekend effect is known to be attenuated in settings with strong all-hours services, such as the emergency34 and critical care35 areas of large regional hospitals. It is possible that MTCs are sufficiently well resourced to provide a consistent trauma service and so achieve equivalent outcomes at all hours. An alternative explanation is that the weekend effect is really a coding artefact16 ,17 that was eliminated by our use of high-quality clinical registry data. Finally, it is possible that the weekend effect identified by previous studies is explained by differences in case mix. In our cohort, the differences in ISS between weekends and weekdays were small and unlikely to be clinically significant. However, this observation should be interpreted in the context of studies that have reported weekend effects in other emergency populations.4–9
There was evidence that secondary transfers into MTCs are increased for patients injured at night. This could be explained by smaller hospitals having sufficient resources to manage such cases during the day but not at night. For example, the availability of senior staff, imaging resources and specialty expertise might have reduced the need to transfer patients during daylight hours. Although case mix could be vulnerable to differences in prehospital triage, there is little evidence to suggest that major trauma triage processes vary by time of day. The decision to convey patients to an MTC is guided by a formal decision tree with additional advice provided to ambulance crews by a major trauma dispatch desk that is accessible at all times.36 However, there were significantly fewer air ambulance transfers at night (5.4% vs 13.8% during the day), which probably results from additional restrictions imposed on aircraft flying after sundown.37 It is possible that a proportion of patients that might have been transferred directly to an MTC by air ambulance during the day were conveyed by vehicle to a non-MTC hospital at night. This is particularly plausible in the case of stable patients in rural areas who are sometimes transferred by air ambulance for logistical reasons rather than a clinical need for rapid treatment.38
Strengths and limitations
The principal strength of this study was its use of a national registry that captures almost all severely injured patients treated at English MTCs. There are a number of limitations that inevitably arise from our use of an observational dataset. It has previously been suggested that in-hospital mortality is a biased outcome measure because it does not capture patients who are discharged early but subsequently die.2 However, this is unlikely to have exerted a substantial effect in the major trauma setting because acutely unwell patients (those at greatest risk of death) should not normally be discharged from hospital. Although we adjusted for known confounders (including age, injury severity and comorbidities), the possibility of residual confounding remains. It is also possible that a weekend effect might be detected in a larger cohort of patients, although a considerable number were included in this study.
It is important to note that a proportion of major trauma cases recorded within TARN did not receive the full benefit of a specialised 24/7 service. This is because some patients are undertriaged and therefore not assessed on arrival by a consultant-grade doctor. Although MTCs are remunerated for providing consultant-grade trauma team leaders, a small number of institutions do not yet guarantee the onsite availability of such a senior clinician at all times. However, MTCs are all distinguished by the 24/7 availability of radiology and operating facilities and it is likely that the majority of patients within TARN were exposed to the full benefits of an all-hours major trauma service in English MTCs.
Finally, this study showed that the weekend effect is undetectable in an all-hours consultant-led major trauma service. However, it cannot show that there was a previous weekend effect that has been eliminated by the major trauma reconfiguration. We did not present data from before the reconfiguration, as case reporting to TARN was incomplete and it was not possible to quantify the services provided by hospitals during this period. It is also possible that this study, which used data from a comprehensive clinical registry, adjusted for confounding factors more successfully than previous studies based on administrative datasets. However, the statistical models used in some earlier studies did achieve similar levels of discrimination to our own but nevertheless reported weekend effects.2 ,3
Conclusion
This study did not find any evidence that weekend major trauma admission is associated with increased mortality in English MTCs. Further work should aim to understand which datasets and hospital services exhibit a weekend effect as a means of understanding whether or not some patients truly experience worse outcomes when admitted at weekends.
Acknowledgments
The authors are grateful to individual MTCs for submitting their data to TARN.
References
Footnotes
Twitter Follow David Metcalfe at @TraumaDataDoc and Antoinette Edwards at @AntoinetteE60
Contributors DM designed the study and drafted the paper. OB extracted the data and performed the statistical analysis. DP, AS, FL, MW, AE and MC contributed to the study design, interpretation of the results and critical appraisal of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Pursuant to the terms of our data sharing agreement with the Trauma Audit & Research Network (TARN), no additional data are available from the corresponding author. Further data may be available on application directly to TARN.
Linked Articles
- Commentary