Article Text

Abstract
Introduction Sexual assault is disturbingly common, yet little is known about those occurring at mass gatherings, defined as a group of people congregated for a common purpose. Our objectives were to examine patterns of variation in sexual assault associated with mass gatherings and to determine factors associated with assaults occurring at mass gatherings.
Methods We performed a case series analysis from January to December, 2013. We included all patients >16 years presenting within 30 days of their sexual assault to the Ottawa Hospital Sexual Assault and Partner Abuse Care Program (SAPACP). Cases were stratified by whether or not they occurred at mass gatherings. We abstracted from the SAPACP records: patient and sexual assault characteristics, alcohol or drug consumption and medical and forensic care accepted. We performed descriptive analyses and multiple logistical regression to identify factors associated with mass gathering assaults.
Results We found 204 cases of sexual assault, of which 53 (26%) occurred at mass gatherings. Relative frequencies of mass gathering sexual assaults peaked during New Year's Eve, Canada Day, university frosh week and Halloween. We found the following factors were statistically significantly associated with sexual assault at mass gatherings: younger age (OR=0.95, 95% CI 0.91 to 0.99); voluntary consumption of drugs and alcohol (3.88, 95% CI 1.34 to 11.23); assault occurring on a holiday (2.37, 95% CI 1.00 to 5.64) and the assailant unknown to the victim (2.43, 95% CI 1.15 to 5).
Interpretation This study is the first to describe patterns of variation in sexual assault incidents associated with occurrence of mass gatherings as well as factors associated with such assaults. We will disseminate these results to key stakeholders in order to develop prevention-minded policies for future mass gatherings.
- violence, interpersonal
- mass gathering medicine
- forensic/legal medicine
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known on this subject?
Sexual assault occurs most often to women between the ages of 18 and 30 years, usually occurs in the victim's home and the assailant is known to the victim between 60% and 85% of the time.
Little is known about the incidence and circumstances of sexual assault associated with mass gatherings.
What might this study add?
In this review of sexual assault cases reported to the only referral centre in Ottawa in 2013, 26% occurred at mass gatherings.
Assaults at mass gatherings occurred more often at holidays and university frosh week.
Victims of sexual assault at mass gatherings were younger, more likely to have consumed alcohol/drugs, to suspect they had been drugged and only knew their assailant 30% of the time.
The distinct nature of sexual assaults at mass gatherings requires a unique approach to prevention, education and policy.
Introduction
Sexual assault is an important public health concern affecting approximately 50% of women in their lifetime.1–3 In general, sexual assault occurs most often to women between the ages of 18 and 30 years, usually occurs in the victim's home and the assailant is known to the victim between 60% and 85% of the time.1–6 Little is known about the incidence of sexual assault associated with mass gatherings. Previous research into this area focused mainly on college and university students in the USA, and particularly those in sororities and fraternities, with alcohol consumption at gatherings identified as risk factors.7–9 No studies have been conducted examining assault patterns or risk factors influencing populations outside of college and university students. Mass gatherings are defined as an organised event occurring within a defined space attended by a large number of people.10 The objectives of this study were to first describe patterns of variation of sexual assaults at mass gatherings in Ottawa and second to determine risk factors associated with these assaults occurring after mass gatherings.
Methods
Design and setting
This is a case series analysis of sexual assaults stratified by whether or not they occurred following a mass gathering. We conducted a health records review from 1 January 2013 to 31 December 2013. This time frame encompassed all mass gatherings occurring in Ottawa without duplication and thus would include all sexually assaulted patients who sought care. Ottawa, population approximately one million, hosts over 50 official mass gatherings a year (eg, public holidays and music festivals).11 The definition of a mass gathering used in our study was any event where a group of people congregated for a common purpose. We purposely did not limit the size of these gatherings in our definition for three reasons: we wanted to include the greatest number of events over the course of a calendar year; there has been no prior definition of mass gathering in the context of sexual assault that would signify an increased risk of sexual assault to a gathering attendee and the medical record usually did not explicitly state the size of the gathering and we were not directly contacting patients to estimate the attendance at the event at which they were sexually assaulted. We sourced the dates for these events using the specific event websites as well as through the City of Ottawa. Public holidays were designated as those recognised in the province of Ontario.
The Ottawa Hospital Sexual Assault and Partner Abuse Care Program (TOH SAPACP) is the sole referral centre for all sexually assaulted patients in Ottawa, providing comprehensive medical and forensic care to any adult victim of sexual assault occurring in the previous 30 days. Referrals originate from victims themselves or any of regional hospitals, police forces, post-secondary learning institutions, mental health providers, community agencies and medical clinics in Ottawa. The SAPACP sees over 200 cases of sexual assault annually.12
Study population
We included all patients aged ≥16 years seen by the SAPACP for a new sexual assault representing a consecutive sample. These were identified from confidential medical records maintained by the SAPACP. All follow-up patient visits or patients presenting >30 days after assault were excluded.
Data collection
Patients were stratified into mass gatherings or control groups based on the narrative information within their medical record identifying them as attending such an event. All patients who did not have a mass gathering explicitly identified or described in their medical record were assigned to the control group. We abstracted the following variables: patient characteristics, mass gathering attendance, date of assault, disclosure of alcohol and/or drug consumption, timing of presentation to the SAPACP, nature of the sexual assault, medical and forensic care accepted.
Outcome measures
The primary outcome measure was the presence of a mass gathering sexual assault documented in the record. The secondary outcomes were factors potentially associated with sexual assault at mass gatherings compared with the control group, including patient age and sex, voluntary alcohol and/or drug consumption, suspected drug-facilitated assault, whether or not the date of the assault was associated with a holiday, loss of consciousness and whether or not the assailant was known to the victim.
Analysis
We calculated descriptive statistics, in particular, mean values and SDs or medians and ranges as appropriate. We assessed bivariable associations between risk factors and mass gathering assaults using the χ2 or Fisher’s exact test for categorical variables or Student’s t or Wilcoxon two-sample tests for continuous or ordinal variables. We conducted multiple logistical regression to further evaluate factors that were associated with sexual assaults occurring at mass gatherings. To avoid overfitting resulting from an inadequate number of events per predictor variable, we entered a maximum of five a priori factors into the logistical regression analysis: patient age, voluntary alcohol and/or drug consumption, date of assault associated with a holiday, loss of consciousness and assailant known to the victim. In these analyses, all patients whose record did not explicitly include documentation of a risk factor (eg, alcohol and/or drug consumption, being known to victim) were classified as not having that risk factor present. We evaluated the sensitivity of our results to this assumption by repeating the logistical regression analysis using only cases with complete data. To avoid increasing the risk of spurious findings, no model reduction or stepwise variable selection was used. Goodness of fit of the model was assessed with the Hosmer–Lemeshow test. To verify the quality of data abstraction, two separate investigators (KS and JG) independently reviewed a randomly selected sample of 10% of the records. We resolved discrepancies by consensus agreement. We calculated a kappa value for these reviews to determine inter-rater reliability. All analyses were conducted using SAS V.9.3 for Windows.
Results
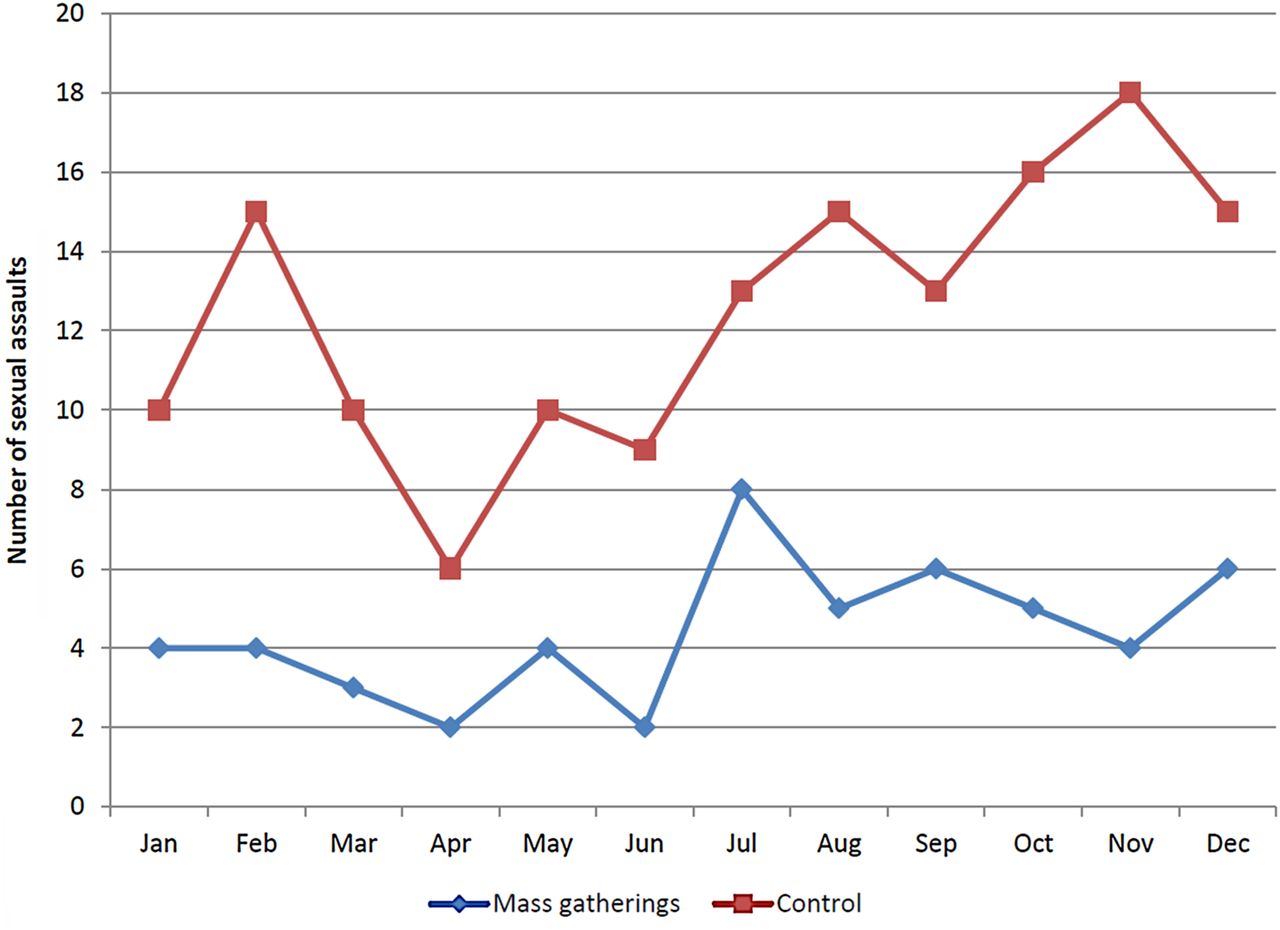
We found 204 new cases of sexual assault in 2013. Of these, 53 (26%) were associated with mass gatherings. The number of sexual assault patients presenting to TOH SAPACP by month are illustrated in figure 1. We noted the proportion of sexual assaults associated with mass gatherings peaked in January, July, September and October, coinciding with New Year's Eve, Canada Day, university frosh week (celebrating the start of the university academic year) and Halloween mass gatherings. This proportion varied over time, reaching a peak in July (38.1%). These proportions are shown in online supplementary appendix 1. The baseline characteristics of the patients are shown in table 1. Patients in the mass gatherings group were younger, more likely to have consumed alcohol and/or drugs, experienced a loss of consciousness during their assault and to have suspected being drugged as compared with the control group.
Baseline characteristics of 204 sexually assaulted patients presenting to the Ottawa Hospital SAPACP (entries are frequency and percentage, unless otherwise indicated)

{kind=link}
Number of sexual assaults presenting to the Ottawa Hospital Sexual Assault and Partner Abuse Care Program (SAPACP) by month in 2013 (n=204; 28% of sexual assaults associated with a mass gathering occurred on a public holiday compared with 19% in the control group).
Table 2 shows the characteristics of the assault. No significant differences were seen between the mass gatherings and control groups in the time from the assault to being seen by the SAPACP, how they arrived in the emergency department, the number of assailants or the bodily injuries observed. The assailant was known to the victim less than one-third of the time in the mass gatherings group versus over half of the time in the control group.
Assault characteristics of 204 sexually assaulted patients presenting to the Ottawa Hospital SAPACP
Table 3 illustrates the medical care accepted by the sexually assaulted patients. No significant differences were noted between the groups.
Medical care accepted by 204 sexually assaulted patients presenting to the Ottawa Hospital SAPACP
The forensic care accepted is shown in table 4. Patients from the mass gatherings group were less likely to release their sexual assault evidence kit (SAEK), commonly known as a ‘rape kit’ to police than those in the control group.
Forensic care accepted by 204 sexually assaulted patients presenting to the Ottawa Hospital SAPACP
When we performed the multiple logistical regression analysis, we found that age (OR=0.95, 95% CI 0.91 to 0.99), voluntary consumption of drugs and/or alcohol (4.4, 95% CI 1.65 to 11.7), assault occurring on a holiday (2.3, 95% CI 1.00 to 5.4) and the assailant unknown to the victim (OR=2.14, 95% CI 1.04 to 4.42) were statistically significantly associated with sexual assault at mass gatherings. Loss of consciousness was not statistically significant in the presence of the other risk factors (OR=1.53, 95% CI 0.75 to 3.2). The Hosmer–Lemeshow goodness-of-fit test showed that the model fit was adequate (p=0.53). The sensitivity analysis of only cases with complete data (n=182) did not change the conclusions.
We calculated a κ value of 0.93 for all variables abstracted in a random sample of 10% of patients included.
Interpretation
Major findings
This is the first study to examine factors associated with sexual assault at mass gatherings. An increased proportion of sexually assaulted patients associated with mass gatherings was seen around Canada Day, university frosh week, Halloween and New Year's Eve. Traditionally, gatherings at these dates tend to have high degrees of alcohol consumption by their participants.13 ,14 Sexually assaulted patients seen after these mass gatherings were more likely to have consumed alcohol or drugs in our study. It has previously been shown that increased alcohol consumption is the most common means of drug-facilitated sexual assault (DFSA), through surreptitiously adding a drug to an alcoholic drink.15 The combined effect of the alcohol and additional drug is usually intended to render a person unconscious. We also noted that patients in the mass gatherings group were significantly younger than in the control group. This may represent the tendency of mass gatherings to attract a younger population and/or a younger population not being as well-versed in safe drug and alcohol consumption strategies.
The assailant was only known to the victim one-third of the time in the mass gatherings group. This concerning finding is markedly different from the control group (60%) and previous studies which have identified that the assailant was known to the victim between 60% and 85% of the time.4–6 Sexual assaults associated with mass gatherings were most often occurring at a friend's home (26.9%) and outdoors (23.1%), likely reflecting the location of the mass gathering itself. SAEKs were completed slightly more often in the mass gatherings group, although this was not statistically significant. Mass gatherings patients were less likely to release this evidence to police however. We had no indication as to the reason for this decision in the health record, patients in the mass gatherings group may have been reluctant to initiate a police investigation based on the evidence collected in the SAEK when they had little or no memory of the assault itself.
Context
Much of the previous literature focusing on college and university students in the USA has established drinking alcohol as a risk factor for sexual assault.7–9 One Canadian study has estimated the rate of suspected DFSA at approximately 25% of patients seen.15 Previous studies examining the nature of sexual assaults have found that the assailant was known in 60%–85% of the assaults and a large proportion of assaults occurred in the victim's home.4–6 Our results would indicate that sexual assault in the context of a mass gathering is a different entity and thus educational, prevention and policy strategy need to differ.
Implications
The results of this study will be disseminated among key local, provincial and national stakeholders in order to develop a unique educational and prevention-minded policy for future mass gatherings. These events represent a significant number of the sexual assaults seen and are an obvious target for prevention strategies at all levels, from the licensing and organisation to the volunteer and security training to public awareness for attendees. Safe partying strategies aimed primarily at the age group of 19–25 years, including the buddy system and alcohol education programmes, are being spearheaded by TOH SAPACP and our community partners. One example of this is Project Sound Check, an extensive training programme for all volunteers for all of the music festivals held in Ottawa has been implemented. A reduction in the number of assaults post-mass gatherings is the overall goal and will be studied in the future. We realise that the number of reported assaults may initially increase as more people are aware of this phenomenon and are willing and able to report them.
Limitations
Limitations of this study include being a single centre (although our centre is the single referral site for all sexual assaults in the city) and not capturing the proportion of sexual assaults that do not seek medical care. We may have misclassified a small proportion of assaults associated with mass gatherings as this was not always explicitly charted in the medical records. Finally, we did have a proportion (11%), though low, of records with missing data which were either not documented in the health record or missing due to the lack of recall on the part of patient who experienced a loss of consciousness during the assault, but sensitivity analyses revealed that results were robust against the presence of missing data.
Conclusions
This Canadian study is the first to establish an association between a peak in sexual assaults and the occurrence of mass gatherings and to identify factors associated with mass gathering assaults. The nature of these assaults is different than assaults previously documented in the literature and thus requires a unique approach to prevention, education and policy. We plan to increase awareness around these events and engage in prevention strategies in order to reduce the number of sexual assaults occurring.
Acknowledgments
The authors wish to thank MyLinh Tran for her assistance with the statistical analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Twitter Follow Kari Sampsel at @KariSampsel
Contributors KS: Study design, funding, data analysis, interpretation of data and manuscript preparation. JG: Data analysis and review of manuscript. TL: Assistance with study design and review of manuscript. MT: Study guidance, data analysis, interpretation of data and review of manuscript. LC: Study guidance, data analysis, interpretation of data and review of manuscript.
Funding The Women's College Hospital Women's XChange provided the grant funding for this work.
Competing interests None declared.
Ethics approval The Ottawa Hospital Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.