Article Text

Abstract
Field referral of emergency ambulance patients by paramedics on a widespread basis is a relatively new aspect of paramedicine. Its implementation involves a significant revision to paramedics’ clinical responsibilities and level of interaction with medical specialists. Using grounded theory methodology, this qualitative study uses interviews with paramedics from Ontario, Canada, to explore the framing of risk associated with these referrals in the context of caring for patients with two high-stakes medical conditions: acute stroke and S–T elevation myocardial infarction. The results outline how paramedics have incorporated risk framing into their practice.
- paramedics
- practitioners
- prehospital care, clinical management
Statistics from Altmetric.com
Key messages
What is already known on this subject?
While there is a significant amount of information available on the technical aspects of field referral, there is very little research available on the non-technical aspects, such as how risk is framed.
What might this study add?
Using the context of high-stakes field referrals, this study reports that paramedics have developed a unique aspect of their practice with respect to how they frame risks for field-referral patients in order to facilitate transport.
Insights into the nature of paramedicine such as these can improve the likelihood of success of programmes that alter paramedics’ scope of practice, such as field referral.
When discussing the nature of professional responsibilities, it is well accepted that being a professional involves more than just technical or objective knowledge, such as recognising the clinical presentation of high-risk conditions. Professionals have a responsibility to use both objective and subjective knowledge.1 ,2 Several researchers have emphasised the importance of the subjective, non-technical aspects of paramedicine3–7 and investigated how paramedics manage the interplay between objective knowledge and its subjective application. A need for research in this area has been recognised internationally8–10 and can make an important contribution to more fully understanding the nature of paramedicine.
This interplay is particularly important during the communication of acute health risks. Although perhaps obvious, it is worth confirming that risk as a concept is the probability of a negative outcome.11 The mandate of conceptualising risk has been located within the province of the professions since the early 1900s,12 and since then health professionals have worked to improve their understanding of how risk is framed because understanding risk is often essential for clinical decision making. In this study, risk framing refers to how paramedics present risk-related information to patients.
Study context
Emergency ambulance patients who are suspected of suffering from an acute stroke or S–T elevation myocardial infarction (STEMI) represent a unique group of patients because there are two possible transport options: (1) transport the patient from the scene directly to a local hospital ED that is located close to the patient or (2) transport the patient from the scene as a field referral, directly to a physician who specialises in these conditions who is located in a more distant regional treatment centre. Which transport option is selected in these cases is complicated because there are operational considerations involved including the fact that these patients are often clinically unstable; patients must be informed about their transportation options and consent to transport to either destination, and referrals often require time-pressured consultation between medical specialists and paramedics (prior to their departure from the scene).
In these circumstances, there are two main categories of health risks that paramedics must consider when they frame risks for a given patient. These are (1) risks associated with the results of patient assessments, for example, possible acute stroke or STEMI and (2) risks associated with long (to a regional centre) versus short (to a local ED) transport time.
How risk is framed can be a major determinant of patient selection of treatment (and transport) options.13 Stated more optimistically, risk framing can be very helpful in terms of facilitating patient access to time-sensitive regional interventions. However, for patients with acute stroke and STEMI, this can be a difficult undertaking when we consider that it is challenging even within the controlled environment of a hospital to identify and treat these patients within strict time limits.14 Yet, paramedical referral seeks to extend these goals into the operationally diverse and uncontrolled prehospital setting, making these referrals both high-stakes and ambitious.
In this qualitative study then, I explore the framing of risk by paramedics for patients with acute stroke and STEMI who may be receiving field-based referrals directly to medical specialists.
Method
There is little formal research into the non-technical aspects of how paramedics implement field referrals used in emergency medical services (EMS) and so this situation required the use of an exploratory approach. Additionally, as a practical matter field referral must be activated by paramedics on an individualised basis, and so it was important to obtain an understanding of the practitioners’ point of view. This necessitated an approach that would emphasise the context of referral, provide in-depth data and draw on highly personalised perspectives.15 Grounded theory methodology (GTM) was therefore an appropriate choice as it is ideally suited for exploring social contexts and processes and for emphasising the participants’ perspective.16 GTM uses systematic, inductive and cyclical data collection and analysis to discover hidden social processes that are subsequently organised and abstracted into concepts.16
Participants
All the participants in this study were paramedical employees of a large suburban land ambulance service in Ontario, Canada. Their employer agreed to allow participation on a voluntary, confidential and anonymous (to anyone other than the researcher) basis, with the researcher contacting participants directly. All participants signed voluntary informed consent agreements. Selection was purposeful as all participants were required to meet criteria that fit with the topic to be studied. Thus, the sampling criteria for participating paramedics were:
hold current paramedical credentials as required by provincial regulations
be employed as a paramedic in a certified land ambulance service actively using EMS STEMI and acute stroke referral programmes
have received in-service training on the use of EMS acute stroke and STEMI referral protocols
have personal experience using EMS acute stroke and STEMI referral.
Charmaz17 describes this sampling in GTM as purposive because it establishes a relevant starting point for data collection. I interviewed a total of 15 paramedics, comprising 11 men and 4 women. All had successfully completed a 2 year preservice college programme.
Data collection and analysis
I obtained data during in-depth, private interviews with paramedics using a series of open-ended questions concerning field referrals. To minimise researcher influence on the participants, I (1) introduced myself as a researcher, not affiliated with the paramedics’ employer, exploring the non-technical aspects of field referrals and emphasised that the interviews were intended to gather practitioner views and (2) maintained an approach of encouraging participants to respond on a relatively unstructured basis and focus the conversation on those aspects of referrals that they believed were important and relevant. These interviews varied in length from 1 to 2 h. Interviews were audiotaped and the recordings were subsequently transcribed to facilitate analysis. There were three rounds of interviews, and each round included five different paramedics. During the initial round, open coding (meaning there were no predetermined categories for grouping data) was used followed by line-by-line data analysis to identify recurring categories of narrative. This ensured that the categories were based on the respondents’ data. For example, many initial comments concerned how paramedics present transport risks for patients’ who indicated uncertainty with respect to accepting the longer transport time required for referrals from their residence to a regional centre. As an example, one paramedic said “when patients are hesitant, I emphasize the logic of going (to the regional centre)”, so an initial, rather broad category of “how options are presented to uncertain patients” was established. During this step, I wrote numerous memos in what Charmaz17 describes as a self-conversation to identify possible categories and to determine direction to take subsequent sampling. This step ‘prompts analysis … to explicate and fill out categories’ (p. 72). The next step was to revise interview questions in accordance with these memos to support theoretical sampling during the second round. Here I focused on seeking data relevant to theoretical concepts such as risk framing and establishing trust that had emerged during round 1. These questions were then used to sample during a second round of interviews using the same interview approach. A major strength of theoretical sampling is that researchers can develop and densify16 categories that have emerged, so that data are clarified as much as possible. Again, line-by-line analysis of interview transcripts was used to ensure that the patterns in data were consistent with the development of concepts. Consistent with GTM, constant comparison16 of data was used to progressively develop the concepts and an understanding of the social processes in play. For example, this step enabled the refinement of the earlier category or code into that of ‘narrowing of uncertainty’ when presenting risks involved during referrals. Further, when paramedics emphasised the importance of communicating potential risks to patients quickly during their risk framing of uncertainty, the property of speed was identified and so the category was clarified into ‘rapid narrowing of uncertainty’.
As the theoretical concepts became clearer, I decided to return to the field for a confirmatory step. Thus, the key aspects of the theory were organised into open-ended interview questions and the third group of paramedics were asked to indicate if they believed these concepts accurately described their approach to framing of health risks, and to add any information they believed was relevant. Strauss and Corbin16 and Charmaz17 describe this step as part of theoretical sampling, where researchers return to the field to evaluate their transfer of data into concepts. The interview questions used for each round are listed in online supplementary appendix A.
Cessation of sampling occurred once theoretical saturation14 was reached, meaning that no new information relevant to the theory was forthcoming.
This human subject research was approved by a hospital-based research ethics board, and the confidentiality of paramedical identities is preserved by using artificial initials for attributing narratives.
Results
Paramedics described being aware that in recommending referral to patients they are introducing an element of risk to their patients’ lives and they are doing so during a high-stakes situation (a list of these risks identified by paramedics is provided in the online supplementary appendix B). They are aware, for example, that there can be significant transportation risks associated with the referral. Patients in acute distress (such as those with borderline unstable vital signs) may have definitive care delayed due to the longer transport time needed if a local hospital is bypassed to travel to a regional referral/treatment centre. Additionally, once a referral has been activated, it is extremely difficult to undo: second chances are rare. Operationally, for example, this would involve a reversal of transport distance, essentially meaning that the transport time in this circumstance is actually double for the portion of ‘retraced travel’. As explained by ‘AK’ when considering whether to recommend a field referral, “The patient's presentation and history is what it comes down to and do we know [for example] is there is a road closure [en route], that will that add another 30 minutes [to the transport time]? My ability to reverse my position [if a patient suddenly deteriorates] is then impacted”. This complexity of this situation is compounded by the fact that a referral does not equal treatment, meaning that a given patient may be referred but not receive an intervention and so they may have been exposed to risk with no benefit. So at the time of referral, no one knows for certain whether the patient will be adversely affected by transport risks.
Given this situation, several themes emerged from the data in terms of how paramedics frame risks for patients during referrals.
The first theme was emphasising the importance of establishing trust with the patient. This actually commences upon arrival at the scene. As explained by ‘GH’, “First and foremost everything we are doing is always in their [patients] best interests and so once we arrive the patients sort of know this and that awareness sort of transmits. If I am confident and professional in my delivery they are quite accepting”. And ‘AK’ describes his approach: “If the patient sees that I remain calm and have confidence and am speaking clearly then I gain their confidence. So rarely will I show any anxiety. That works really well. Calmness is contagious”.
A second theme was demonstrating transparency when conducting patient assessments. For example, when paramedics described performing a 12-lead ECG, they did not conceal the tracing from the patient. Rather, the opposite is emphasised and they deliberately showed the tracing to most patients together with an explanation of what the tracing indicates. LM explains “I like to explain when we are reading an ECG. I don't just show it to my partner, I tell the patient right away and tell them what we are going to do. I am honest”.
A third theme was being authentic in their communications. This authenticity requires making a judgement concerning frankness as explained by ‘LM’, “I look at the strip and say you may be having a blockage in your heart”. Additionally, paramedics described knowing that their patients are being confronted with new information that involves medical technology and this can be alienating. Paramedics described wanting to ensure that their communication has been understood. As ‘GH’ explained “I don't want them to be agreeing with us yet really having no idea what is doing on. I want them to understand everything we have done”.
Although a referral is often readily accepted by the patient, this is not always the case. Sometimes patients are unsure whether to agree, particularly if transportation involves bypassing a closer community hospital, and paramedics use several strategies in these cases. One of these is being blunt as explained by ‘RL’: “It looks like you may be having a heart attack”. Another is by using logic as explained by ‘NP’: “I reiterate that we are trying to get them to a hospital where there are specialists. The local hospital doesn't have the equipment that the specialist has. Getting you to the specialist is better than getting to the local hospital and then having to get you to that same specialist anyway during a second trip”. Sometimes paramedics recruit family members to provide support for the referral: “If they [family] have a grasp of the situation then I say this is what we want to do and they help”, ‘TB’.
A fourth theme was rapidly narrowing the uncertainties associated with field referrals. Paramedics described being very aware of the need for speed related to decision making as emphasised by ‘JP’, “time is always in my head”, and ‘GH’, “there is a lot of quick decision making”. Additionally, paramedics discussed providing as much certainty as possible as explained by ‘BA’, “The things I know for certain, I let them [patients] know so they are prepared for what will happen e.g. You will be met by a cardiac team”.
A final theme was making sure that the communication of the risk is coupled with a plan of action. This means that the referral process is incorporated within a message of action, intended to mitigate inherent risk. As explained by ‘LM’, “I say we are taking you to the best place for you and I am staying with you and committed to getting you there. We are doing everything we can – those simple phrases really help”. Consequently, patients are not left to wonder what will happen to them now that they know they are at risk, rather they are provided with a means to act in their own best interests by cooperating with the paramedics.
When these themes were organised and presented to the paramedics interviewed during the final round, they all confirmed that the themes represented their key considerations during referrals.
Discussion
The framing of risk can be a major influence in patients’ understanding of clinical options and subsequent decision making.18 ,19 For professionals, this part of their practice is often nuanced and calls for situational-specific judgements. This is because while professionals have considerable discretion in choosing which and how risks are communicated to patients, they also have to consider which risk narrative is most productive in a specific patient's context. For instance, risk disclosure brings with it an element of responsibility to avoid so-called risk-mongering,12 which would do more harm than good.
Paramedics reported being aware of the risks that are in play to one extent or another in a given call. This awareness appears to motivate several specific social processes that are evident in paramedical descriptions of the framing of risk and include establishing trust, with emphasis on being transparent, and authentic. However, the next process is a less obvious, two-part process of ‘rapid narrowing’.
The ‘rapid’ refers to that fact that the acuity of the patient's condition necessitates rapid decision making. As time passes at the scene, the likelihood of an effective referral diminishes and in some cases, this involves working within a time frame of mere minutes. Yet, within the operational limits imposed by time, paramedics must provide sufficient clarity to support informed consent. This means discussing suspected diagnosis, and related risks versus benefits, while being careful not to add to the stress of an already apprehensive patient.
To support this process, paramedics reported disclosing the uncertainty associated with a field-referral situation in a particular way. They ‘narrow’ the uncertainty.20 But they do not do this in the more traditional and common use of population-based statistical probabilities. Rather, they use a conceptual, qualitative approach that relies on narrative. This type of risk discussion is recognised as professional in nature and is one way to fit risk to an individual patient's needs.12 There is legitimacy to the selection of this approach during referrals, because variables such as drive time and patient acuity are unlikely to ever be the same for any two patients. The content of these paramedical narrowing narratives comprised emphasising the potential benefits of expert care in a regional centre by medical specialists, and the access to this expertise via direct transport.
This rapid narrowing also includes a particular way of interpreting patient assessment findings. Paramedics described interpreting their findings in an auspicious manner,21 meaning that they emphasise the positive aspects of a referral. For patients who are being presented with potentially overwhelming technical information, this approach can be both informative and reassuring.
When coupled with a final process of providing a clear plan of action, this approach establishes social momentum for moving the trajectory5 of the case forward. There is also a symmetry to this framing, as its final step reinforces its first step, namely the trust between patient and paramedic.
Professional practice must be understood in the context of the particular line of work under consideration. Paramedicine is a unique occupation and not surprisingly there is a unique character to its practice, which reflects the fiduciary application1 of paramedical knowledge in uncontrolled and time-sensitive prehospital settings. When paramedics are dealing with patients requiring field referrals, they need to make objective clinical patient assessments and then use subjective knowledge to fit these clinical findings to the needs of each patient. The themes identified in figure 1 comprise this subjective knowledge, in the form of social processes.

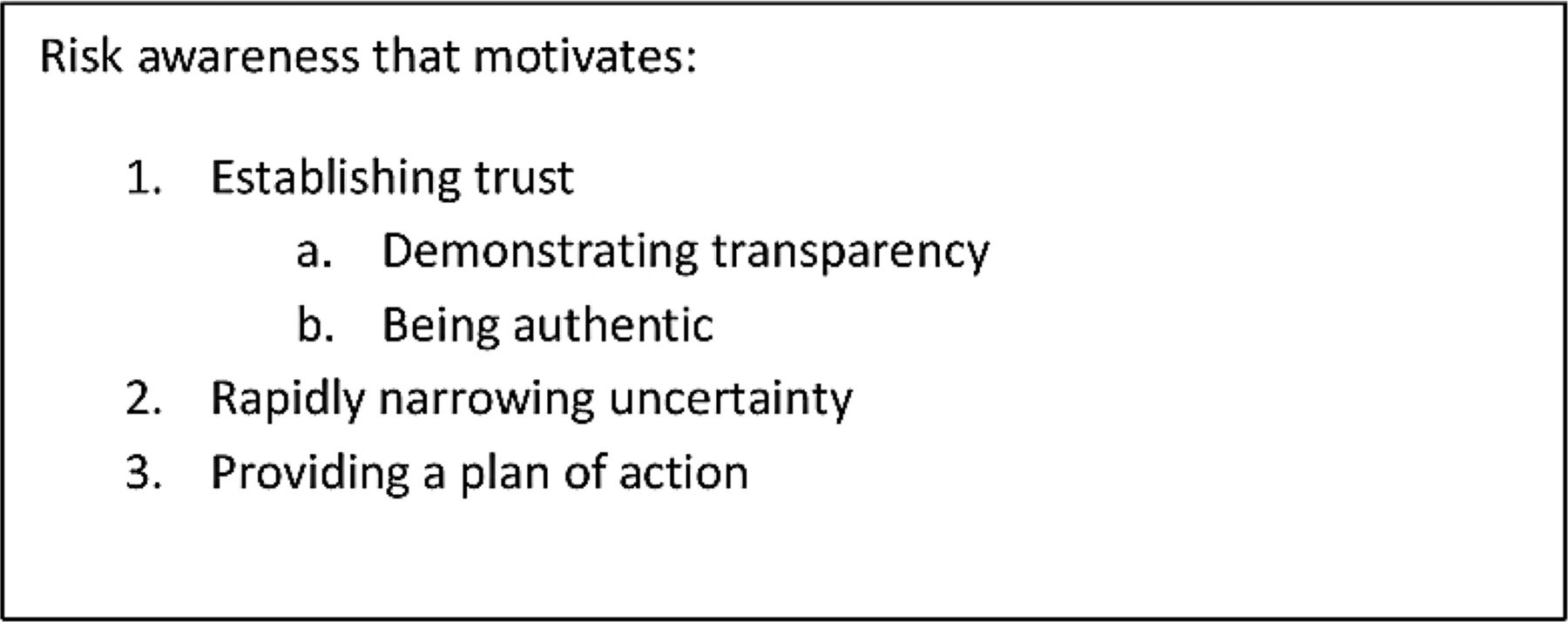{kind=link}
Paramedical risk framing during field referral of acute stroke and S–T elevation myocardial infarction patients.
Note that although there are various ways of determining the quality of GTM15–17 studies, one aspect they have in common is an emphasis on procedures that connect data to the theoretical concepts developed in the study. In this case, trustworthiness relies principally on the use of verbatim interview transcripts, line-by-line coding of data, constant comparison of data to emergent concepts and end-stage verification with participates.
Limitations
Consistent with inquiry into an area that has not been well researched, this study should be considered exploratory rather than definitive. Readers are reminded that the study's data are narratives provided by paramedics, not field observations. Also, although the form of GTM used here emphases line-by-line coding, which establishes strong connections between data and theory, it is also true that social science research inevitably includes the researcher's interpretation of data.15 ,17 Finally, GTM is intended to generate, not test, theoretical understandings of social phenomenon. Further observational research into this area would provide important related insights into the nature of paramedicine.
Conclusion
Paramedics have a professional responsibility to frame the risks associated with the high-stakes referral of patients experiencing acute stroke and STEMIs. This study's findings reveal a type of paramedical risk framing that is qualitative in nature and consists of establishing trust, rapidly narrowing uncertainty and providing a plan of action. Awareness of this aspect of practice may assist with programme-related training, evaluation and management.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online Appendix A
- Data supplement 3 - Online Appendix B
- Data supplement 4 - Online figures
Footnotes
Competing interests None declared.
Ethics approval Sunnybrook Health Sciences Centre Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.