Article Text

Abstract
Objective ED visits have been rising year on year worldwide. It has been suggested that some of these visits could be avoided if low-acuity patients had better primary care access. This study explored patients' efforts to avoid ED presentation and alternative care sought prior to presentation.
Methods Consecutive adult patients presenting to three urban EDs in Edmonton, Canada, completed a questionnaire collecting demographics, actions attempted to avoid presentation and reasons for presentation. Survey data were cross-referenced to a minimal patient dataset containing ED and demographic information.
Results A total of 1402 patients (66.5%) completed the survey. Although 89.3% of the patients felt that the ED was their best care option, the majority of patients (60.1%) sought alternative care or advice prior to presentation. Men, individuals who presented with injury only, and individuals with less than a high school education were all less likely to seek alternative care. Alternative care actions included visiting a physician (54.1%) or an alternative healthcare professional (eg, chiropractor, physiotherapist, etc; 21.2%), calling physician offices (47%) or the regional health information line (13%). Of those who called their physicians, the majority received advice to present to the ED (67.5%).
Conclusions Most low-acuity patients attempt to avoid ED presentation by seeking alternative care. This analysis identifies groups of individuals in the study region who are less likely to seek alternative care first and may benefit from targeted interventions/education. Other regions may wish to complete a similar profile to determine which patients are less likely to seek alternative care first.
- emergency department
- access to care
Statistics from Altmetric.com
Key messages
What is already known on this subject?
Low-acuity visits contribute to high ED input and entry block.
Some of these presentations may be avoidable if patients had better access to primary care.
To date, however, increasing primary care access alone has had minimal impact on reducing low-acuity presentations to the ED.
What this study adds?
The majority of the 1402 low-acuity patients presenting during weekday office hours to three study EDs attempted alternative care prior to ED presentation.
They perceive the ED as their best care option regardless of presentation severity.
Men, individuals who presented with injury only, and individuals with a high school education or less were all less likely to seek alternative care before coming to the ED.
These factors may guide future targeted education and intervention efforts but may still need to be externally validated.
Introduction
Patient presentations for emergency care are increasing internationally.1 The high demand for services often exceeds ED staffs' abilities to provide evidence-based and timely care, resulting in delays to time-sensitive treatments, patient dissatisfaction and overwhelming anxiety for staff.2 ,3 Low-acuity presentations contribute to high ED input and ‘entry block’,4 leaving open the question of why these patients do not use a less resource-intensive place of care. In the UK, an estimated 10%–30% of ED patients could be treated appropriately in the primary care setting.5 ,6
In Canada, non-urgent patients have access to care through family physicians, walk-in clinics, urgent care centres or local EDs. Their care choices have no financial ramifications. Availability of care alternatives is province-dependent. In Edmonton, Canada, a 2004 study on low-acuity patients' care choices identified that 61% of low-acuity patients reported attempting alternative healthcare prior to ED presentation.7 Since 2004, this region's health system has undergone substantial reform. A single provincial healthcare delivery system—Alberta Health Services (AHS)—has replaced multiple regional health authorities. This has resulted in many healthcare delivery changes, including a provincial medical help line (Health Link), implementation of strategies to reduce ED delays and the display of real-time ED wait time estimates on the AHS website. Significant efforts to increase provincial residents' access and attachment to a primary care provider (eg, general practitioner, family physician) have accompanied these changes. Despite these measures, claims by policymakers of ‘inappropriate’ (ie, low-acuity) and/or convenience ED attendance as a major input issue persist.
Given the significant efforts in this region to reduce non-urgent presentations through the aforementioned strategies, an up-to-date analysis of what care patients had attempted, if any, prior to presentation is needed. Exploring patient actions and rationales for ED presentation is important for developing a ‘whole system approach’ to sustainable interventions to reduce non-urgent visits and potentially relieve some of the pressure of high ED volumes and entry block experienced by EDs.
This study of non-urgent ED presentations identifies the characteristics of patients who sought alternative care prior to ED presentation and their knowledge and use of alternative sources of healthcare such as the provincial helpline and the wait time website.
Methods
Study design
A cross-sectional survey of ED patients was undertaken over a 10-week period (May–July 2013) at the Royal Alexandra Hospital (RAH), Northeast Community Health Centre (NECHC) and the University of Alberta Hospital (UAH) in Edmonton, Canada. Both the RAH and the UAH are major referral centres for trauma. The NECHC is a community ED; together, these three centres assessed and managed over 330 000 patient visits during the study year (AHS, 2013 data). The three hospitals represent diverse patient populations, are staffed by full-time emergency physicians and have various levels of trainees.
Study participants
Patients aged ≥17 years presenting consecutively to the ED with a Canadian Triage and Acuity Scale (CTAS)8 score of ≥3 (less acute) were eligible for inclusion in the study as these have been identified by Canadian policymakers as potentially ‘inappropriate attenders’. CTAS is a valid and reliable five-level triage tool used in EDs across Canada to determine the timing of patient assessment based on severity. The scale does not account for the comorbidities and/or complexity of patients at presentation. Children were excluded from the study as one of the included hospitals (UAH) has a separate paediatric ED, which is not administratively linked with the adult ED and the reasons for presentation are different for children. Patients were excluded from the study if they were cognitively impaired, deemed too unwell (eg, nausea, pain or intoxication) to participate, had been previously enrolled, were direct consultations, presented to the ED for imaging tests or a preset appointment or were under police escort. If the patient's ability to consent was unclear, the attending physician or nurse provided final adjudication regarding the patient's ability. Patients who were unable to read or communicate in English were also excluded, unless a friend or family member was able to complete the survey on their behalf.
Survey methods
A non-stratified, cluster-based random sampling method was used. Each week during the study period this was randomly assigned, via a computerised random number generator, each week during the study period, to one of three ED registration periods: 07:00–13:00, 09:00–15:00 or 13:00–19:00. Randomisation was balanced so that each of the three ED registration periods occurred at least once at each site. Patients presenting later than 19:00, overnight and on weekends were not included, as many alternative sources of care, such as primary care physician (PCP) practices, are not available during these hours. Within each registration period, randomisation assigned patients a number based on their presentation time. This number identified the order in which patients were approached. The electronic Emergency Department Information System provided minimal patient information such as name, age, CTAS triage score and time of arrival.
A 47-item questionnaire was developed based on a previously validated survey,7 with some additional questions capturing risky health practices. Patients completed the questionnaire, which was available in both paper and computerised tablet form, through either self-administration or interview based on the patient's preference. The questionnaire was completed within 15–20 min and included questions on the reasons for ED presentation as well as care sought prior to presentation.
Sample size
The sample size calculation method has been described elsewhere.7 Briefly, based on estimates obtained from previous research at the UAH and RAH, the proportion of ED patients reporting no family physician in 2004 was 21%. In order to obtain a precision of approximately 3% surrounding the point estimate, a sample size of approximately 500 from each site was required for an expected total recruitment of approximately 1500 patients. To obtain a more precise estimate (∼1%) would have required more than 1000 patients per site, which was beyond the resources available for this study.
Statistical analysis
Data were entered into a custom-built Microsoft Excel spreadsheet (Microsoft, Redmond, Washington, USA). Thematic content analysis was completed using patients' qualitative responses to understand the reasons why patients felt the ED was (or was not) their best care option. Previous experience and review of the literature informed the identification of themes. Two independent research staff themed a subset of responses. Inconsistencies in theming were resolved through discussion.
Quantitative analyses were conducted using the Statistical Package for the Social Sciences (SPSS, V.13.0, Chicago, Illinois, USA). Dichotomous variables were reported as proportions; continuous variables were reported as means and SDs or medians and IQRs, as appropriate. Patients who sought alternative care before ED presentation were compared with those who did not using bivariate analyses of association (t-test or Mann-Whitney U test for continuous variables and χ2 test or Fisher's exact test for categorical variables, as appropriate). Seeking alternative care was defined as at least one of: visiting a physician, visiting another healthcare professional, calling a physician's office, calling the AHS Health Link line or seeking other treatment or advice sought prior to presentation. A logistic regression model was used to determine factors that were associated with seeking alternative care prior to ED presentation using backward Wald techniques (model entry set at p=0.2 and model removal set at p=0.15). This model entry allows for all variables to be entered and then each one eliminated in an iterative process to arrive at the most parsimonious model. The sample size was sufficient to avoid inflation of the standard error concerns.9
Ethics
The study protocol and materials were approved by the Health Research Ethics Board (Reference ID: Pro00039886) at the University of Alberta, Edmonton, Alberta, Canada. Patients provided verbal consent to discuss the study with a research staff member and completion of the survey represented implied consent.
Results
Sampling
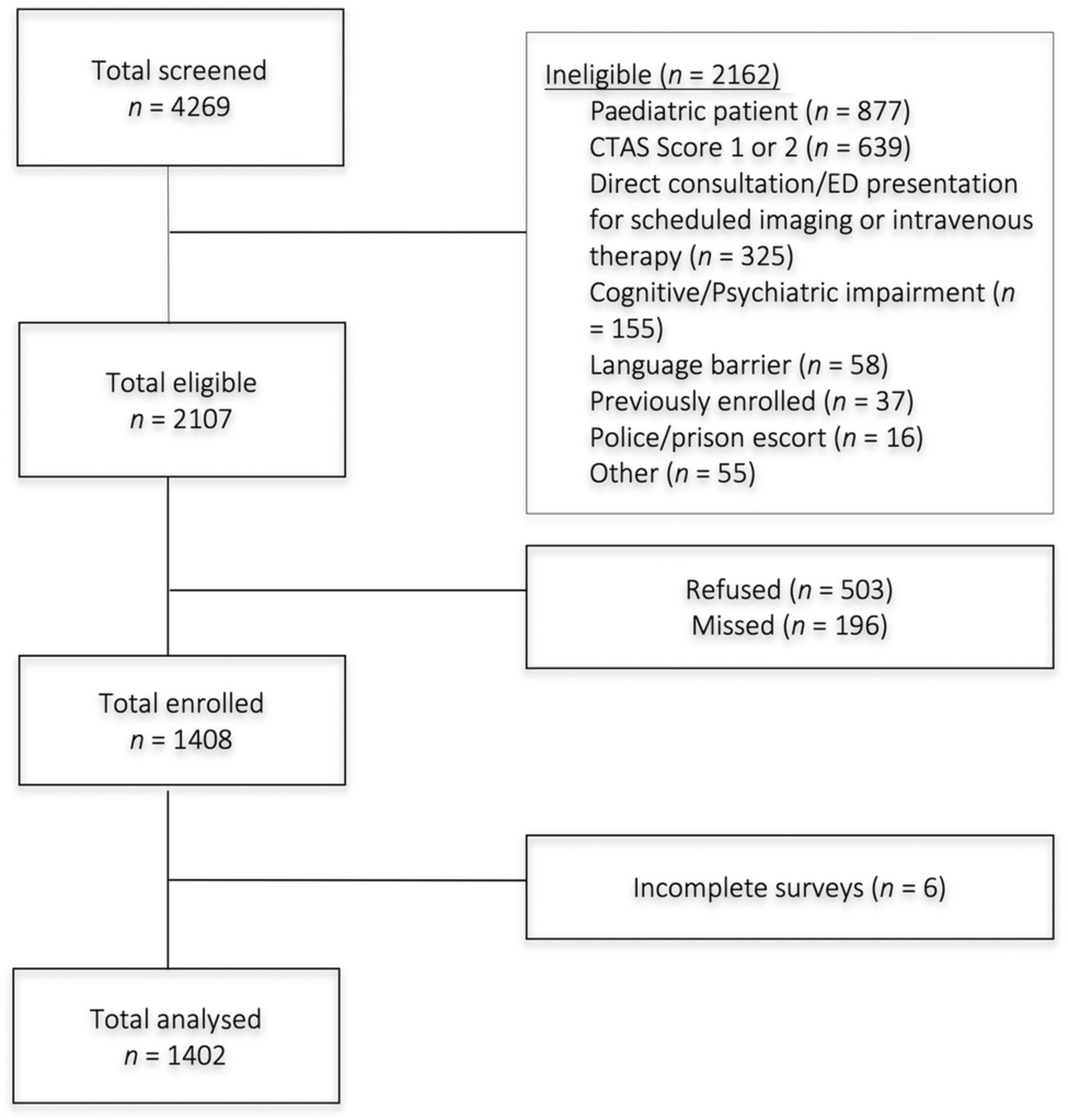
A total of 4269 patients were screened, of which 2107 were eligible. Of the 2107 eligible patients, 503 patients declined to participate and 196 were missed (ie, research assistants were unable to locate the patient at the time of their selection for participation). Overall, 1408 patients were enrolled and 1402 completed questionnaires were analysed (figure 1). Six participants were excluded from the analysis due to a failure to respond to the five survey questions that distinguished participants who attempted to seek alternative care from those who did not.
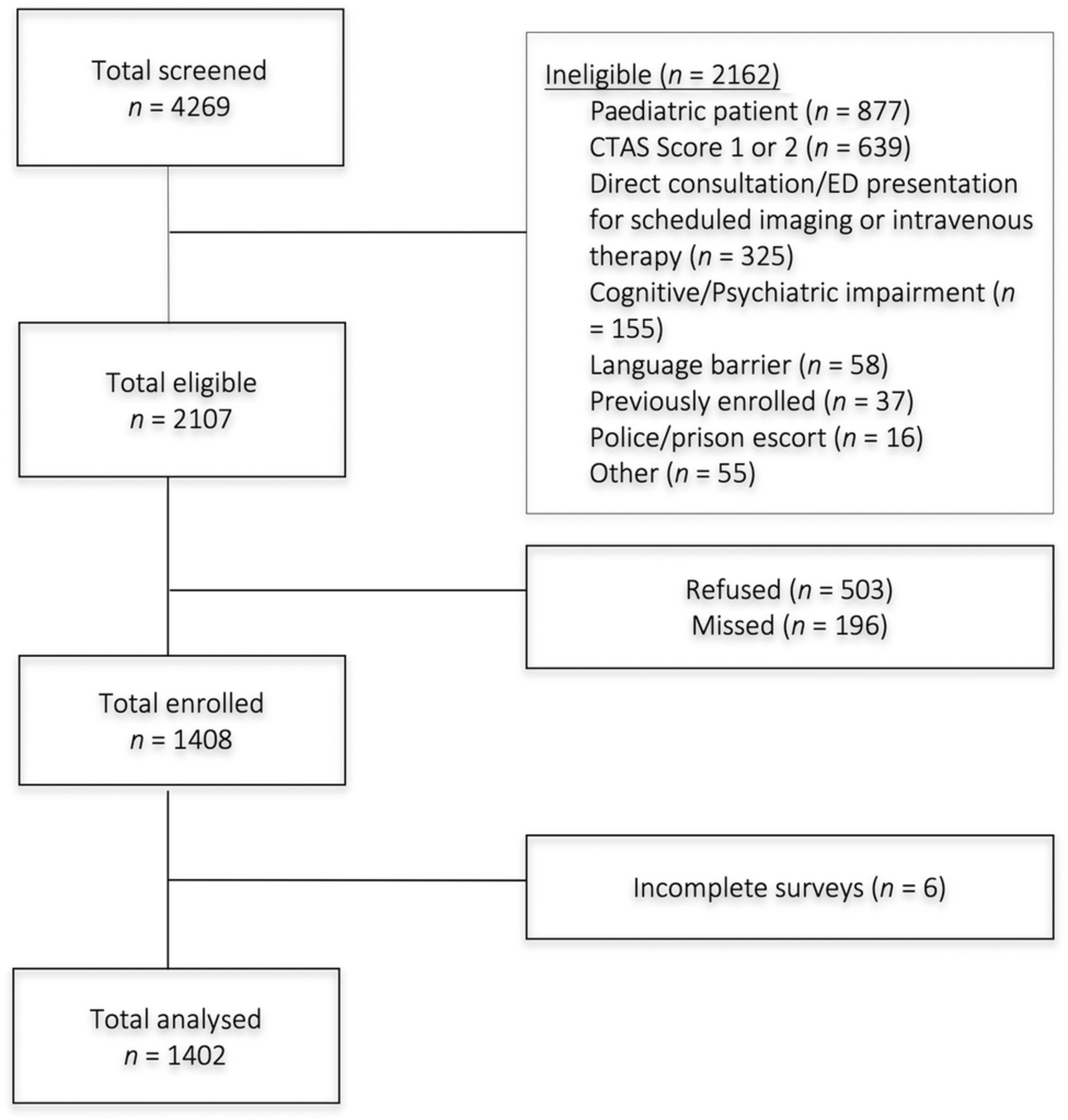
Patient recruitment flow diagram. CTAS, Canadian Triage and Acuity Scale
Participant characteristics
Characteristics of study participants are summarised in table 1. Briefly, the mean age was 45.2 years (SD: 19.8), the majority were women and most patients identified themselves as being Caucasian. The majority of patients reported that their presenting problem was due to illness or injury; 4.0% presented due to both. The majority of patients were triaged with a CTAS score of 3.
Demographic characteristics of patients who did and did not attempt to access alternative care prior to the emergency department visit
Reasons for presentation: thematic content
Overall, 89.3% of the patients (n=1234/1382) felt the ED was their best care option. Themes included: safety, effectiveness, patient-centred, access and efficiency (figure 2 and table 2). For patients who felt the ED was their best option, rationales included: safety concerns (n=309), effectiveness of ED care (n=284), patient-centredness of ED (n=277) and access to healthcare professionals at the ED (n=204). For patients who felt the ED was not their best option (n=148/1382 (10.7%)), rationales included perceptions that access to health professionals outside the ED was preferable (n=39), patient-centredness (particularly timeliness) was lacking in the ED (n=26) and their health concern was not significant enough to require ED care (n=18).
Qualitative themes for patients' self-reported feelings about being at the Emergency department

{kind=link}
{kind=link}
Qualitative data flow diagram.
Sought alternative care before the ED visit
The majority of patients (n=842 (60.1%)) reported that they attempted to access at least one source of alternative care before presentation. Their baseline characteristics were similar to the total patient sample (see table 1). The univariate analyses found no statistically significant differences in sexual orientation, employment status, living situation, residence, smoking status, alcohol consumption, drug use, having had a influenza shot, CTAS score or mode of arrival to ED between participants who sought alternative care before presenting to the ED and those who did not (p value >0.05).
Factors associated with seeking alternative care before the ED visit
Regardless of statistical significance at the univariate level, some variables were considered clinically important and were retained in the multivariable analysis, including employment status, living situation, residence, smoking status and having had a influenza shot in the past year. The multivariable logistic regression identified that men, patients presenting because of injury only, and having a high school education or less were all less likely to attempt alternative care before ED presentation (table 3).
Factors associated with seeking alternative care prior to Emergency department visit; bivariate (unadjusted OR) and multivariable regression (adjusted OR)
Alternatives selected
Of the 842 patients who attempted alternative care (table 4), 452 (54.1%) visited a physician and 176 (21.2%) visited another healthcare professional. Less than half (n=394/833 (47.3%)) of these patients reported calling a physician's office prior to ED presentation. Of those who called, the majority received advice to present to the ED (67.5%). Patients also received advice to visit a family physician (5.7%) or another healthcare professional (3.0%). A small percentage of patients (1.4%) received reassurance only.
Type of actions taken to get alternative care prior to the Emergency department visit
Among patients who sought an alternative, 68.4% (n=566/828) were aware of the AHS Health Link line; although a minority of patients used this resource (13.5%). A minority of patients who sought alternative care were aware of the AHS wait time website (n=204/826 (24.7%)). Of the 8% of patients who checked the website prior to presentation, approximately half (50.8%) reported that the wait time information influenced where they presented.
Discussion
In this multicentre study, many patients (60.1%) made efforts to avoid ED presentation. Our study refutes the myth that low-acuity presentations are ‘convenience visits’ as many patients have attempted alternative care. Despite widespread efforts focusing on mitigating ED volume (eg, Health Link, wait time website, primary care attachment, etc), low-acuity presentations often result from patients experiencing difficulties accessing or receiving adequate help at another source.
Patients attempting alternative care most frequently visited a physician, specifically their family physician. This may indicate a care preference for family physicians; further improving their accessibility may support patients in seeking alternative care. This notion is supported by many patients who reported access-related rationales for their ED presentation. Alternatively, attempting to seek care from their family physician and subsequently presenting to the ED may highlight a limited awareness among patients of this region's urgent care centres, their hours and their services. For example, several study participants reported presenting to the ED for fracture imaging, setting and casting, which is offered by urgent care centres. Including urgent care centre information on family physician ‘out of office’ voicemails and public education on which conditions/symptoms can be effectively managed by urgent care centres may assist those attempting alternative care to be more successful in accessing the care they need outside the ED.
This study identified several factors associated with whether or not alternative care prior to ED presentation was sought. Men, individuals who presented with injury only, and individuals with a high school education or less were all less likely to seek alternatives before presentation. The external validity of these factors is yet to be determined; however, they could assist in targeting public education on care alternatives.
This study also identified the limited use of two widely promoted information points among patients who presented to the ED: the regional health line and the ED wait time website. While these findings could be confounded by limited awareness and selection bias, further research on these services is required to identify potential facilitators and barriers to use and to examine the effectiveness of subsequent revisions of these services.
Other literature
The proportion of patients who sought alternative care is higher in this study than elsewhere,10 although previous work has not focused solely on regular primary care clinic hours when patients have the highest number and variety of non-ED care options. This study supports previous research suggesting patients perceive the ED as their best care option because they perceive an urgency of health need, timeliness and access to ‘one-stop shop’ care, referral to the ED and accessibility to care.11–13 Our findings support those reported by Masso et al11 which suggest that patients' perception of urgent care needs differs from clinicians. Recently, Beache and Guell13 highlighted the role of social customs in presentation decisions by low-acuity patients. Consequently, strategies for reducing low-acuity ED visits may need to address factors other than primary care access, such as public education addressing local social customs and ensuring adequate health system capacity.14 ,15 In addition, with evidence suggesting ineffectiveness, primary practices should be discouraged from performing annual physical examinations.16 Moreover, they should be encouraged to (1) expand hours; (2) reserve a proportion (all) of physician visits for same-day bookings and (3) provide alternative practitioners to see some low-acuity patients.
Evidence for strategies to reduce non-urgent ED visits by increasing primary care access is inconclusive.17–20 The large proportion of patients in this study who unsuccessfully attempted contact with a PCP before coming to the ED indicates that strategies to reduce barriers to PCP access in Alberta, Canada, have had minimal impact and may be compounded by an undersupply of family physicians.21 Similar strategies are being attempted globally (eg, expanded hours, urgent care clinics, patient attachment, co-location of walk-in clinics with EDs,19 ,20 etc). Given the results of this study and the wide array of patient rationales for ED presentation, these strategies may need to be enhanced to address the complexities of patient decisions to visit the ED. Patient rationales for presentation need to be understood before proposing multifaceted interventions. Further research is required to determine the clinical characteristics of non-urgent presentations and the clinical and economic impact of non-urgent patients on the ED, thereby informing tailored and evidence-based strategies to reduce non-urgent visits and potentially reduce the impact of low-acuity presentations on entry block, ED staff stress and improve ED resource use.
Limitations
This study contained several limitations. First, CTAS was used as a proxy measure of the need for ED care. Triage scores are an imperfect measure of ‘inappropriate attendance’ as they do not account for patient comorbidities or complexity and not all patients having CTAS score of 3–5 could be appropriately cared for in primary care clinics; however, administrators often use these scores to define visit appropriateness. Additionally, a higher proportion of moderate acuity (CTAS 3) compared with low-acuity patients (CTAS 4 or 5) were included in the study. This is representative of ED presentations to study sites for the study year; among patients having CTAS score of 3–5, patients having a CTAS score of 3 were the largest group (66.1%) (AHS data). Second, this study excluded children, who make up a large proportion of ‘inappropriate’ ED attendances in some regions.22 Third, this study was unable to collect data on patients' presenting complaint or discharge diagnoses. This information would be useful in characterising frequent presentations to the ED that could be appropriately treated in primary care. Identifying these conditions may assist in future efforts to educate patients on what requires emergency care. Fourth, baseline differences in patient characteristics suggest that variation in ED use exists within these sites (a unique ‘signature’ for each ED), limiting the generalisability of the results. Research in other contexts may provide additional granularity. Fifth, the qualitative analysis was limited to a few questions integrated throughout the questionnaire. As is common among survey work, this format may have resulted in a priming of participants to their care-seeking decisions and social desirability bias may have influenced the results. Finally, the study's refusal rate and participants' responses may have been negatively influenced by lengthy delays prior to being seen and a protracted length of stay.
Conclusion
Patients using EDs in this region appear to make considerable efforts to avoid the ED by seeking care elsewhere, despite the high proportion of patients without regular physicians and the barriers to accessing alternative care. This study identified factors associated with not attempting to seek alternative care which may guide targeted interventions and education; however, the external validity of this socio-demographic and clinical profile is yet to be determined. Most non-urgent patients perceive the ED as a highly appropriate place for care and it remains an important safety net within many healthcare systems in developed countries. Finally, these results should stimulate further epidemiological and clinical research into barriers faced by patients in accessing care outside the ED.
Acknowledgments
The authors would like the thank Danielle DeVuyst, Francis Tenorio, Elfriede Cross, Dr Don Voaklander and Dr Maria Ospina for their assistance with this study.
References
Footnotes
Presentations: Presented in part at the Western Emergency Department Operations Conference in Alberta, Canada, 2014; Canadian Emergency Physician Association Conference in Ontario, Canada, 2014 and the International Conference on Emergency Medicine, in Hong Kong, 2014.
Contributors The project was conceived by BHR, RC and GC. All named co-authors participated sufficiently in the project to claim authorship based on international standards for authorship. SWK coordinated the study; RC, AD, TN, BV, BH and SWK collected the data. Data management was provided by SC, CV-R and KC. Analysis was completed by KC, LDK and CA. All authors contributed to editing the manuscript and are able to take responsibility for the finished product.
Funding AIHS (PRIHS-2), Emergency Strategic Clinical Network—AHS, Brain Care Centre. This research was supported by the Emergency Medicine Research Group in the Department of Emergency Medicine at the University of Alberta, Alberta Health Services (AHS) through the Emergency Strategic Clinical Network (AHS), Alberta Innovates Health Solutions (AIHS) through the Partnership for Research and Innovation in the Health System (AIHS PRIHS #201400398) grant and the Brain Care Centre (all in Edmonton, Alberta, Canada). RC was supported by a Summer Studentship from the Alberta Centre for Injury Control and Research in the School of Public Health, University of Alberta, Edmonton, Alberta, Canada. BH was supported by an AIHS Summer Studentship. During this study, CV-R was supported by Canadian Institutes of Health Research (CIHR) in partnership with the Knowledge Translation branch. BHR is supported by the CIHR as a Tier I Canada Research Chair in Evidence-based Emergency Medicine through the Government of Canada. The funders do not take responsibility for the conduct, content and conclusions drawn by the study authors. Funding was secured by DV and BHR.
Competing interests None declared.
Ethics approval Health Research Ethics Board at the University of Alberta.
Provenance and peer review Not commissioned; externally peer reviewed.