Article Text

Abstract
Background Networked organised systems of care for patients with major trauma now exist in many countries, designed around the needs of the majority of patients (90% adults). Non-accidental injury is a significant cause of paediatric major trauma and has a different injury and age profile from accidental injury (AI). This paper compares the prehospital and inhospital phases of the patient pathway for children with suspected abuse, with those accidentally injured.
Methods The paediatric database of the national trauma registry of England and Wales, Trauma Audit and Research Network, was interrogated from April 2012 (the launch of the major trauma networks) to June 2015, comparing the patient pathway for cases of suspected child abuse (SCA) with AI.
Results In the study population of 7825 children, 7344 (94%) were classified as AI and 481 (6%) as SCA. SCA cases were younger (median 0.4 years vs 7 years for AI), had a higher Injury Severity Score (median 16vs9 for AI), and had nearly three times higher mortality (5.7%vs2.2% for AI). Other differences included presentation to hospital evenly throughout the day and year, arrival by non-ambulance means to hospital (74%) and delayed presentation to hospital from the time of injury (median 8 hours vs 1.8 hours for AI). Despite more severe injuries, these infants were less likely to receive key interventions in a timely manner. Only 20% arrived to a designated paediatric-capable major trauma centre. Secondary transfer to specialist care, if needed, took a median of 21.6 hours from injury(vs 13.8 hours for AI).
Conclusion These data show that children with major trauma that is inflicted rather than accidental follow a different pathway through the trauma system. The current model of major trauma care is not a good fit for the way in which child victims of suspected abuse present to healthcare. To achieve better care, awareness of this patient profile needs to increase, and trauma networks should adjust their conventional responses.
- major trauma management
- paediatric injury
- non-accidental injury
- paediatric emergency med
- paediatrics
Statistics from Altmetric.com
Key messages
What is already known on this subject?
Serious injury arising from child abuse mainly affects small infants.
Children severely injured from abuse have a higher mortality and a higher Injury Severity Score, mainly from head injury.
Trauma networks are designed around the needs of adults and rely on early identification of a severely injured patient for maximising survival.
What this study adds?
Infants severely injured through child abuse present late to hospital, and the majority arrive at hospitals designated as non-major trauma centres via non-ambulance transport.
Gold-standard emergency trauma care is less likely to be achieved in these children.
To achieve better patient outcomes, major trauma networks need to adapt their traditional response in order to identify and treat these infants.
Introduction
Many developed countries have created organised networks of hospitals for major trauma care through creating designated specialist centres in order to deliver better outcomes. This process happened in the UK in April 2012, with the formation of trauma networks and designated major trauma centres (MTCs) similar to other countries. The decision of the Emergency Medical Services (EMS) on initial patient destination (MTC or nearest hospital) is based on distances and the patient’s condition. A prehospital triage tool is used to make this decision. The drivers to change in the delivery of trauma care were based mainly on the evidence of improved outcome in adult patients.
Children account for around 10% of major trauma in developed countries and are known to present to the major trauma system in a different way from adults.1 In recent years, non-accidental injury (NAI) has been the fourth most common mechanism of injury in children with major trauma.2 Abused children form a distinct subset of paediatric trauma with different characteristics compared with children who are accidentally injured.3 Differences in patient characteristics may affect the way in which health services need to respond. This is the first paper to compare key points in the patient pathway of children with accidental injury (AI) versus NAI.
Methods
The Trauma Audit and Research Network (TARN) database from April 2012 to June 2015 was examined for patients under 16 years old. The patient demographics and key stages of the patient pathway were compared for cases of suspected child abuse (SCA) versus AI. Subgroup analysis for mortality rate was performed, where the outcome was known. The database records mortality at discharge from hospital; however, in some instances where patients are transferred between hospitals, TARN data may not be complete.
Patients are reported to the TARN database if they suffer an injury and are admitted to the hospital for at least 3 days, are admitted to a critical-care area, are transferred for specialist care, or die in the hospital. Patients who die before reaching the hospital (no hospital resuscitation performed) are not included. Patients admitted to the hospital directly and indirectly (via another hospital) in England and Wales are included. All 189 eligible hospitals contributed data during the time of the study.
TARN data co-ordinators (specifically trained clerical staff or nurses) in submitting hospitals enter ‘intent of injury’ as a compulsory data field. SCA is a subcategory of intent that is used only when there is clear evidence in the hospital notes that the clinical staff were investigating child abuse with a high degree of suspicion. It is not possible for data co-ordinators to know whether abuse was ultimately proven. Children with self-harm were excluded, as being neither AI nor SCA. Also excluded were children categorised as ‘alleged assault’, as previous scrutiny of these children3 demonstrated that they were typically interpersonal injury of a non-abusive nature.
Cases of AI and SCA were compared for age, injury severity, body area most severely injured and crude mortality rate. Key stages in the patient pathway, from the time of injury to definitive specialist care, were compared. The prehospital phase analysis included mode of arrival to the hospital, time of arrival (from the time of injury) and MTC designation of the first and subsequent (secondary transfer) receiving hospitals (whether MTC or not). In the UK, MTCs are subdesignated as adult only, child only or combined; however, this is not the same worldwide, so in the analysis, all MTCs were included as one group. Hospitals without specialist trauma services are designated trauma units (TUs). The inhospital phase of the patient pathway was analysed using the key stages defined in the ‘dashboard’ used for quality assurance within UK trauma networks. This quality dashboard includes time-based indicators for key stages of the patient pathway. These nationally set, time-based markers were therefore used to compare the two groups.
Data extraction and analysis were performed using SQL Server 2012, Excel (Microsoft, Redmond, CA), SPSS V.22.0 (IBM, Armonk, New York) and STATA (Statacorp, College Station, Texas, USA). Demographic and injury data were categorised and reported as numbers (percentage). Pearson’s χ2 test was used to test the distribution and significance of these variables. p Values were derived from Pearson’s χ2 test. TARN has Health Research Authority (PIAGG Section 20) approval to conduct research on anonymised patient data.
Results
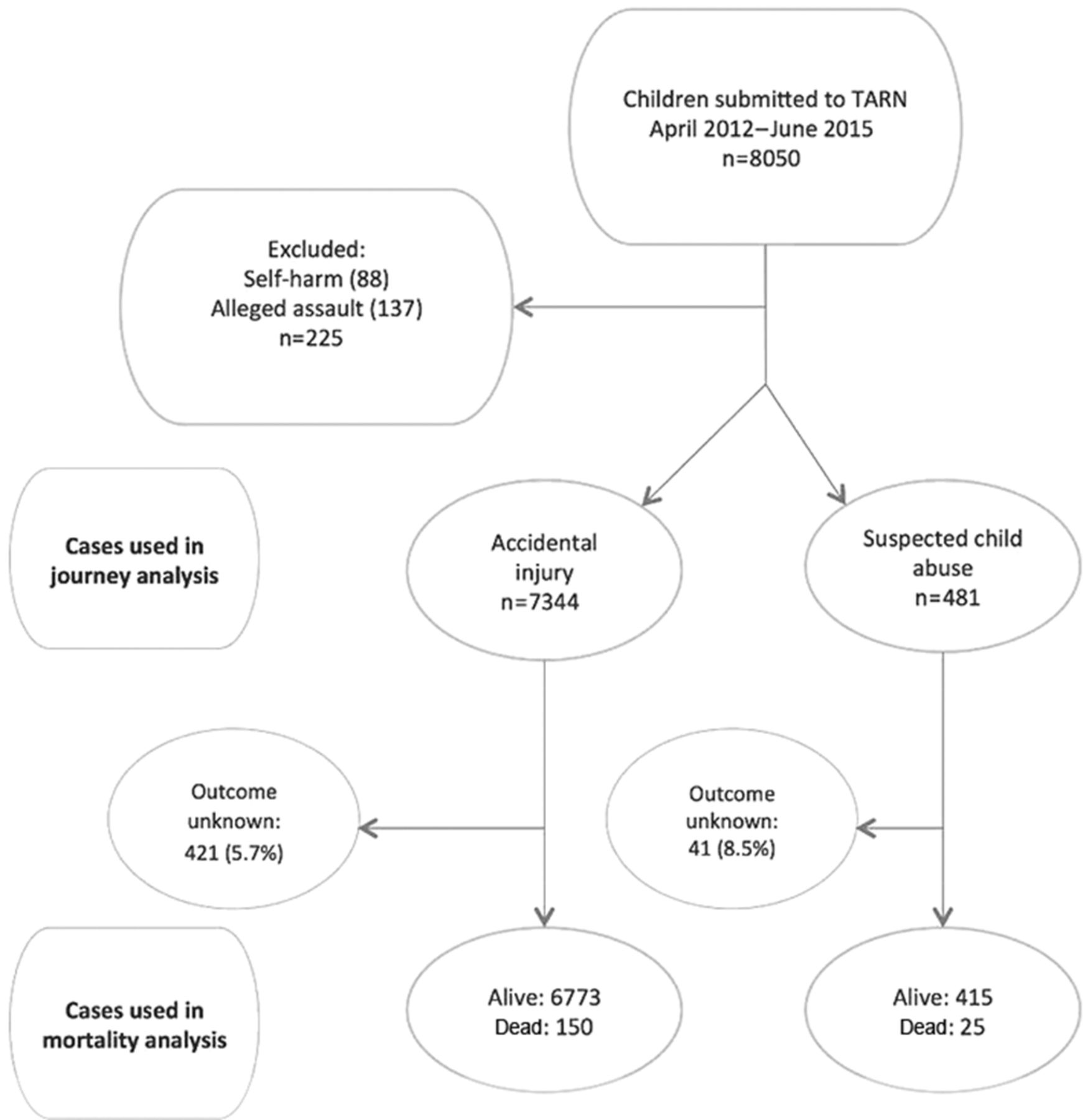
There were 8050 children recorded in the TARN dataset during the study period. There were no cases with missing data for ‘intent’, as this is a compulsory data field. Figure 1 shows the case identification for this study, and the subset of cases used for the mortality calculation.
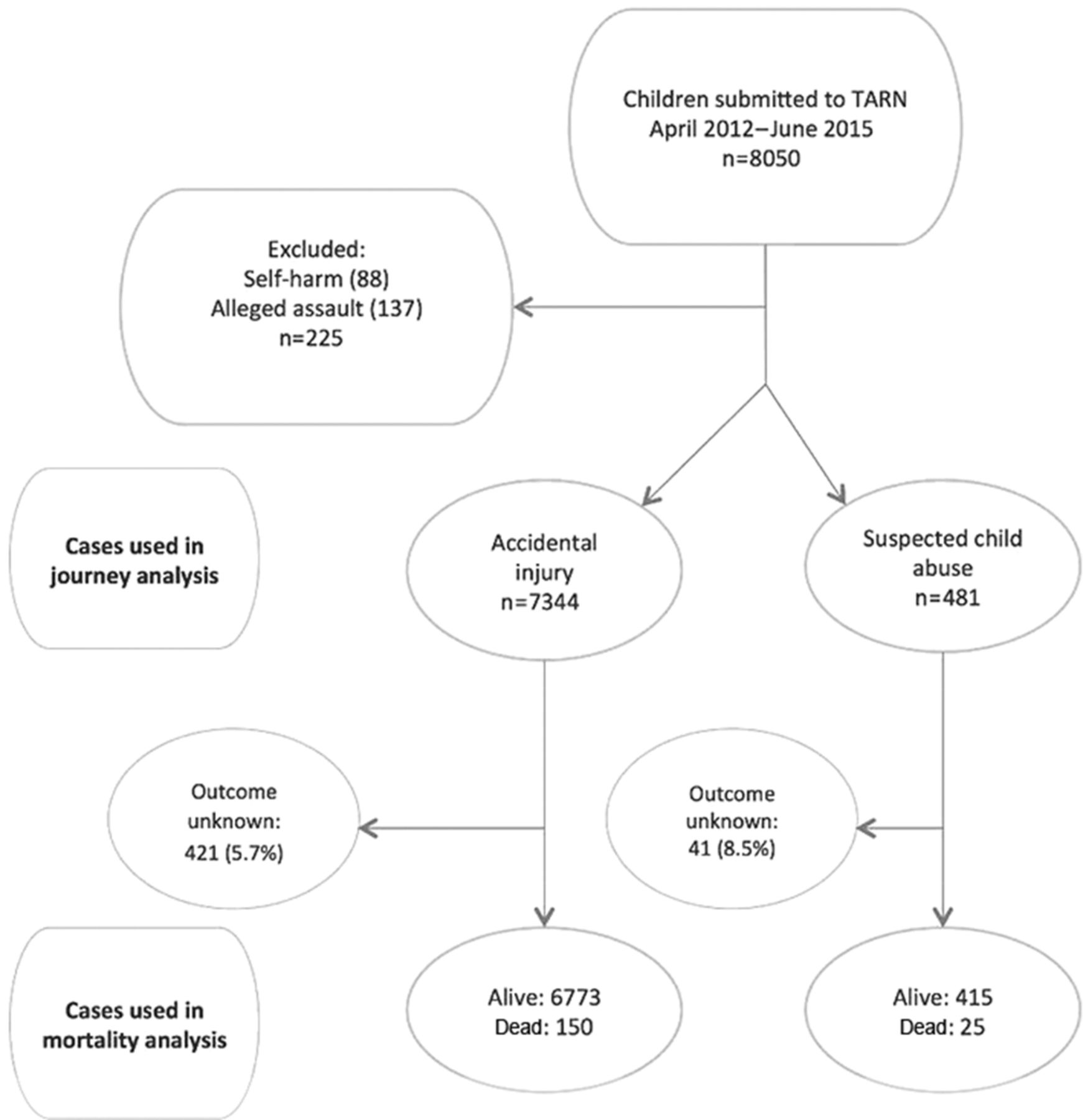
Case identification.
Demographic comparisons between the 7344 cases of AI and the 481 cases of SCA are shown in table 1.
Demographic comparison of AI and SCA cases (95% CIs)
There was a large difference in age range. Children with SCA were younger (median 0.4 years old, IQR 0.2–0.9) versus AI (median 7.2 years, IQR 2.6–12.3). The majority of children severely injured from SCA were under the age of 6 months.
The Injury Severity Score (ISS) for SCA was higher (median 16 versus a median of 9 for AI). The most common body area severely injured (Abbreviated Injury Score 3+) was head injury in the SCA group (56% compared with only 27% for the AI group), whereas limb injury was the most common body area in the AI group (51% compared with 26% in the SCA group).
When patients with ISS>15 were examined by year of age, the highest number of cases of severe trauma were in children aged under 1 year (figure 2), around half of which were SCA cases.

Patients ISS>15 by age. AI, accidental injury; SCA, suspected child abuse.
The higher overall ISS for cases of SCA was reflected in the crude mortality rate, which was 2.2% (95% CI 1.8 to 2.6) for the AI group and nearly three times that figure, 5.7% (95% CI 2.5 to 6.6), for the suspected abuse cases (table 2).
Patient outcome
Table 3 compares the prehospital phase of the patient pathway for both patient groups, from the time of injury to arrival at the hospital, whether MTC or TU.
Fewer children with SCA arrived by organised EMS: ambulance 25.6% (95% CI 21.7% to 29.5%) vs 44% (95% CI 42.9% to 45.1%) or helicopter 0.6% (95% CI 0% to 1.3%) vs 7.6% (95% CI 7% to 8.2%). In many cases, the mode of arrival was not recorded (46.2% of AI cases and 71.5% of SCA cases). Due to the way in which the data entry is structured, if there are no prehospital data from EMS, the mode of arrival is difficult to enter. Therefore, it is likely that all of the ‘unrecorded’ arrivals were outside the EMS system. From previous research within the TARN database, we know that unrecorded cases represent arrival by car (which means that the figure of 25.6% is probably an underestimate of non-use of the ambulance service).
Children with SCA took longer to reach a hospital from the time of injury (table 3), with a median time of 8 hours (CI 1.2 to 21.2) compared with 1.5 hours (CI 1 to 9.3) in AI. The need for secondary transfer to an MTC incurred similar delays in both groups, but combined parental and hospital delays mean that in the SCA group, an MTC was not reached until a median of 21.6 hours (CI 7.9 to 41) after injury.
Prehospital phase (95% CI)
The majority of severely injured children initially arrived at a hospital without designated MTC status. Only 40% of children with AI arrived directly to an MTC and even fewer with SCA (28%). Arrival to an MTC designated with ‘adult-only’ status (without specific paediatric trauma facilities) was seen in a significant number of patients (9% of AI and 8% of SCA cases). Therefore, only 32% of children with SCA arrived initially at an appropriate facility.
There was a difference in time of day of arrival to hospital (figure 3). Arrival time in SCA was fairly evenly spread out between 08.00 and 20.00 hours, whereas children with AI mainly arrive from 15.00 to 20.00 hours (between the end of school and bedtime).

Time of day of arrival.
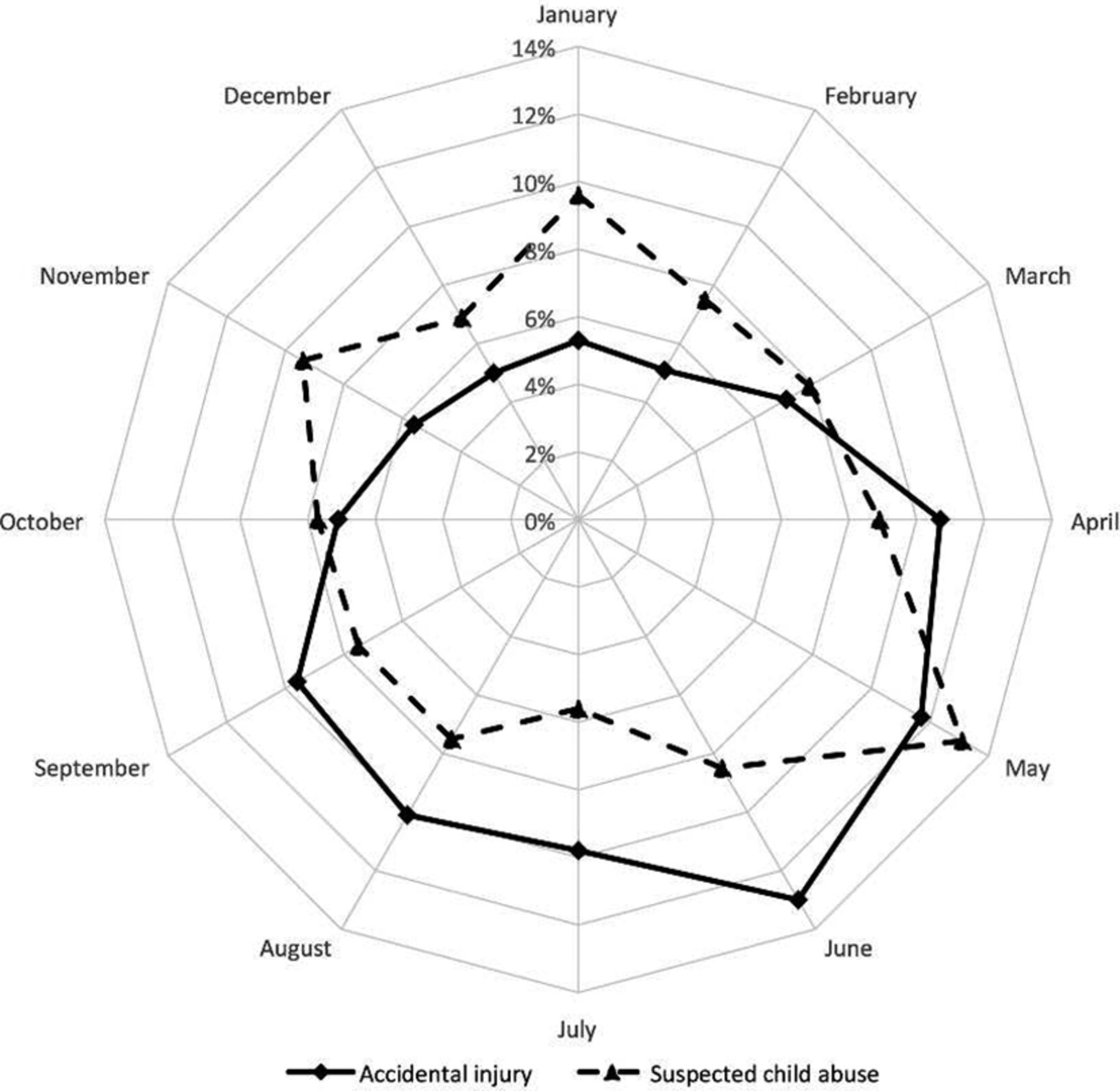
Differences were also seen for the month of arrival. The UK (in the Northern Hemisphere) has more accidental injuries during the summer months (figure 4), whereas SCA presents to hospitals more evenly spread out throughout the year.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Month of arrival.
The inhospital phase of the patient pathway (table 4) shows differences in key treatment goals between the two groups. Children in the SCA group were less likely to be greeted by a consultant-led trauma team (34% in SCA vs 61% in AI); however, this difference was not seen in the subgroup that was identified by the ambulance service as triage tool positive (77% SCA vs 87% AI).
Inhospital phase
Fewer patients with SCA with a GCS of less than 9 received definitive airway management within 30 min of arrival (61% in SCA compared with 78% in AI), and fewer of those who required urgent head CT (GCS of less than 13 or other criteria based on national guidelines) were scanned within 60 min of arrival (28% in SCA compared with 84% in AI).
There were no differences seen in longer term processes such onward transfer to an MTC within 2 days of request, transfer to a paediatric MTC for patients who are more sick or completion of the rehabilitation prescription. In the SCA group, there were no cases of open fracture, and none received tranexamic acid.
Discussion
This paper is the first to consider how children with major trauma resulting from SCA flow through the trauma care system and has found previously unreported differences in the demographics and patient pathway. Networked systems of care for major trauma are based on early identification of severe injury, with transport direct to a specialist centre, and are designed predominantly around the needs of the majority of patients (adults). This improves outcomes for adults4 5 and probably also for children.6 However, this paper shows that the current trauma system design is not optimal for injuries from SCA.
Our analysis of the TARN national dataset shows that children with SCA have very different characteristics from those with AI. In keeping with previous literature,3 6–12 this study confirmed that these infants form a distinct subset of major trauma cases. They are much younger (less than 6 months old), have a higher ISS (particularly severe head injury) and have higher mortality. The injuries do not occur with the typical daily and seasonal pattern of AI (occurring most frequently outside school hours and in the summer).
In the prehospital phase of care, despite sustaining more severe injuries, children with SCA took a long time to arrive in the hospital from the injury event (median 8 hours). Transport to a hospital may be deliberately delayed by the abusers and may require another person (eg, family member) to insist that the child is brought to medical attention. Once a decision to seek medical help is made, the majority of cases will present to a hospital by car, unannounced. EMS was called in only 26% of the SCA cases, compared with 46% of AI. Very unwell infants are often brought to a hospital without EMS involvement (infants are easy for parents to carry), so it may be that the age profile of these cases accounts for some of this difference in EMS use. However, EMS may be deliberately avoided, as EMS professionals will see the home circumstances and enquire into the mechanism of injury.
This combination of characteristics (age, injury pattern, time and mode of arrival) means that this subgroup of severely injured children present to the trauma networks in a different way from those accidentally injured.
Organised trauma care networks rely on prehospital identification of major trauma, followed by triage direct to an MTC rather than the nearest (non-specialist) hospital, and prealert of the MTC to assemble a receiving team of senior clinicians ready to deliver rapid clinical care and perform time-critical procedures. The high car conveyance rate in children (compared with adults) is a worldwide issue for paediatric trauma care. In the Australian New South Wales Trauma Registry7 of 1138 children, only 30% of major trauma cases (all causes) arrived directly to an MTC. We have shown that the size of the problem is magnified in SCA. Delay in obtaining specialist care due to a combination of deliberate delay, non-EMS involvement and subsequent arrival to ‘the wrong place’ is unavoidable; 68% presented to ‘the wrong place’ (local hospital) and 74% arrived unannounced, by car.
This poses a significant organisational problem in delivering high-quality trauma care. If secondary transfer to ‘the right place’ is needed, the median time from the time of injury to MTC arrival was very long (21.6 hours), compared with 13.8 hours in AI.
It seems that the pivotal point in treatment comes in identifying the infant as ‘a major trauma case’. Examining the inhospital phase of care, it seems that if an ambulance was called and the child with SCA was identified as ‘a major trauma patient’ by the prehospital triage tool, this group of patients received almost as good a standard of care (consultant-led trauma team in 77% of SCA and 87% of AI). Similar care was seen in the longer term parameters such as onward interhospital transfer and completion of the rehabilitation prescription.
However, without this initial identification of the patient as a major trauma case, patients with SCA were only half as likely as ones with AI to be received by a consultant-led team (34% vs 61% in patients ISS>15). Identification of an infant with a potentially high ISS is difficult, as ISS is calculated retrospectively, and injury may be occult at the time of first contact with EMS or hospital. The higher ISS in SCA cases was usually due to head injury. It is notoriously difficult to detect the subtleties of a decreased GCS in babies, so this triage trigger may be missing.
Without this pivotal identification of the abused infant as ‘a major trauma patient’, it is likely that a ‘domino’ effect then contributes to the failure to deliver key treatments in a timely manner. The trauma system will not have been activated, and the hospital will be unprepared. A senior-led trauma team will not be already assembled to receive the patient (34% in SCA compared with 61% in AI). This leads to severely injured infants being initially assessed by junior staff, who may often be confused by a misleading history about the mechanism of injury (if injury is mentioned at all) and subtle clinical signs such as drowsiness. In the SCA group, definitive airway management was slower, as was time to CT scan.
If abuse is detected during this process, the additional work this brings may distract staff from staying focussed on time-critical trauma interventions. This work includes close supervision and questioning of the family, escalation to police and social services and contacting paediatricians. Given all of these factors, it is perhaps not surprising that there are long delays to key interventions.
The study limitations are those of any database analysis. While TARN data capture of major trauma cases from EDs is good, there is likely to be missing data, since in clinical practice, some cases of NAI present directly to paediatric wards with non-specific symptoms (drowsiness, vomiting, etc). Some of these cases may not have been notified to the TARN database. Of those cases held within the TARN database, the number of SCA cases examined may be lower than those of actual abuse due to the necessity to have a high degree of suspicion recorded in the medical records for the data clerks to input SCA in the ‘injury intent’ field. In the data showing ISS>15 in the under-1-year population, AI is estimated as the mechanism of injury in 56% of cases. It is difficult in the UK for non-mobile infants to sustain major injury accidentally, so it may be that the number of SCA cases throughout the dataset may be an underestimate (because of the threshold for coding SCA as the injury intent). There is a large proportion of missing data for the mode of arrival (46% of AI cases vs 72% of SCA cases), which is most likely due to arrival by car (the prehospital section of the data contains the mode of arrival, but the section is not completed). Time to arrival on a paediatric intensive care unit was not specifically measured in this study; however, it is likely to be several hours in many cases for those who required secondary transfer from a TU or an adult-only MTC.
Conclusion
Abusive injury forms a significant part of the paediatric trauma workload. As modern care of patients with typical major trauma matures and improves, greater awareness of the ‘atypical major trauma case’ is needed. There are interesting analogies with the elderly, who also present to major trauma networks in a way that means they are not immediately identified as severely injured and also experience delays in care (TARN trauma in older people report – in press).
Although older child victims of SCA attract greater media publicity (as there were potential missed opportunities for intervention by the authorities), seriously abused children are, in fact, much more likely to be under 6 months old. Child protection and trauma teaching must emphasise these characteristics of seriously injured abused infants.
This study shows that trauma care systems need to modify their conventional approach to activation to enable early recognition of these infants and swift escalation up to ‘major trauma patient’ status in order to minimise delays to delivery of definitive care. They will arrive unannounced with serious head injuries, several hours postinjury. This is particularly important for non-MTC designated hospitals (who receive many of these patients). While the early parts of the patient pathway are unmodifiable, swifter activation of the trauma network will deliver better care and, hopefully, better patient outcomes to this vulnerable group.
Supplementary file 1
![[SP1.jpg]](https://emj.bmj.com/content/emermed/34/9/562/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
Supplementary file 2
![[SP2.jpg]](https://emj.bmj.com/content/emermed/34/9/562/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
Supplementary file 3
![[SP3.jpg]](https://emj.bmj.com/content/emermed/34/9/562/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
Supplementary file 4
![[SP4.jpg]](https://emj.bmj.com/content/emermed/34/9/562/DC4/embed/inline-supplementary-material-4.jpg?download=true){kind=link}
Supplementary materials
Press release
Files in this Data Supplement:
Footnotes
Contributors All authors contributed substantially to this paper. The main author for correspondence, FCD, was the main writer of the text and had the original idea to investigate this topic. FEL, TJC and RF helped with the writing and structure of the paper. MF-I supplied and helped analyse the data.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.