Article Text

Abstract
Objectives A major incident is any emergency that requires special arrangements by the emergency services and generally involves a large number of people. Recent such events in England have included the Manchester Arena bombing and the Grenfell Tower disaster. Hospitals are required by law to keep a major incident plan (MIP) outlining the response to such an event. In a survey conducted in 2006 we found a substantial knowledge gap among key individuals that would be expected to respond to the enactment of an MIP. We set out to repeat this survey study and assess any improvement since our original report.
Methods We identified NHS trusts in England that received more than 30 000 patients through the emergency department in the fourth quarter of the 2016/2017 period. We contacted the on-call anaesthetic, emergency, general surgery, and trauma and orthopaedic registrar at each location and asked each individual to answer a short verbal survey assessing their confidence in using their hospital’s MIP.
Results Of those eligible for the study, 62% were able to be contacted and consented to the study. In total 50% of respondents had read all or part of their hospital’s MIP, 46.8% were confident that they knew where their plan was stored, and 36% knew the role they would play if a plan came into effect. These results show less confidence among middle-grade doctors compared with 2006.
Conclusions Confidence in using MIPs among specialty registrars in England is still low. In light of this, we make a number of recommendations designed to improve the education of hospital doctors in reacting to major incidents.
- emergency care systems
- major incident, planning
- guidelines
- education
- disaster planning and response
Statistics from Altmetric.com
Key messages
What is already known on this subject
Major incident plans are documents produced by hospitals in order to lay out the medical response to serious events.
In a previous study conducted in 2006 among NHS trusts in England, we demonstrated that understanding of the major incident plan among hospital registrars was low, highlighting the need for improvement in this area.
What this study adds
A repeat survey has found that confidence among registrars for responding to and using major incidents plans remains poor, and suggests that more education on this topic is required.
Introduction
A major incident is any emergency requiring the implementation of special arrangements by the emergency services and will generally involve large numbers of casualties.1 To respond appropriately to such events, all hospitals are required to keep a major incident plan (MIP) under the Civil Contingencies Act of 2004.2 The plan covers the strategic, tactical and operational management of such scenarios and identifies key commanding members of the emergency team, including the anaesthetic/intensive treatment unit (ITU), emergency medicine, general surgery, and trauma and orthopaedic registrars and consultants.
In 2006, following the 7/7 London bombings, we conducted a survey assessing confidence using MIPs among registrars in specialties that would be expected to respond to a major incident3 and found that many had not even read their hospital’s MIP nor knew where to find it, demonstrating the need for significant improvement. Similar conclusions have been drawn by other studies in the UK.4 5 We concluded by highlighting the importance of educating doctors about MIPs. Since our previous report, several large-scale events (including the Manchester Arena bombing and Grenfell Tower disaster) have demonstrated that major incident planning is more relevant now than ever. We have therefore revisited our earlier research and set out to determine whether there has been a substantive change in knowledge and confidence compared with our original report.
Methods
We identified NHS trusts in England that received more than 30 000 patients through the emergency department in the fourth quarter of 2016/2017 using publicly available data from NHS England.6 In each of these trusts we contacted the on-call registrars (middle-grade doctors in specialty training) in anaesthetics, emergency medicine, general surgery, and trauma and orthopaedics via the hospital switchboard. After gaining verbal consent to participate, we conducted our questionnaire on the phone (online supplementary figure 1). This survey is the same as the one used in our original study and has only three questions in order to maximise response rate. Two contact attempts were made for each individual. Results were then compiled for the group as a whole and by specialty. We determined that three response categories for each question were appropriate for analysis and that the nuance between the ‘in-between’ answers was not substantially different in practice. This also allowed us to compare results with the 2006 paper, where the same process was employed. All data are shown to one decimal place.
Supplemental material
Results
We identified 76 NHS trusts in England that matched our search criteria. Two of these were community healthcare trusts, only accepting minor injuries, and were excluded. We then attempted to contact 296 registrars across the 74 remaining hospital trusts. One hundred and eighty-six (62.8%) individuals consented to being included and gave their responses to the survey, while the remaining 110 (37.2%) either did not consent or were uncontactable after two attempts (online supplementary figure 2).
Supplemental material
The responses of our survey are detailed in table 1 and figure 1. Trauma and orthopaedics had the highest response rate, while emergency medicine had the lowest. Half of the responding individuals had read their hospital’s MIP, with 46.8% being confident they knew where the guidelines were kept. Only 36% of individuals were sure of the role they would play if an MIP came into effect while they were on call. The greatest number of responses came from trauma and orthopaedic registrars, while emergency medicine registrars were generally the most confident in using the MIP. Results were broadly similar to our previous study, although fewer individuals were confident in their role in the MIP (figure 2).

Questionnaire responses separated by question and specialty. (A) Responses to ‘Have you read your hospital’s Major Incident Plan?’; a total of 46 individuals (24.7%) had read all, 47 (25.3%) part and 93 (50.0%) had read none. (B) Responses to ‘Do you know where you can access your hospital’s major incident plan guidelines?’; a total of 87 (46.8%) responded yes, 66 (35.5%) were unsure and 33 (17.7%) responded no. (C) Responses to ‘Do you know what role you would play if a major incident plan came into effect while you were on call?’; 67 (36.0%) responded yes, 69 (37.1%) were unsure and 50 (26.9%) responded no. ITU = Intensive treatment unit
![[emermed-2019-208436supp001.jpg]](https://emj.bmj.com/content/emermed/36/12/762/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
![[emermed-2019-208436supp002.jpg]](https://emj.bmj.com/content/emermed/36/12/762/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
{kind=link}
{kind=link}
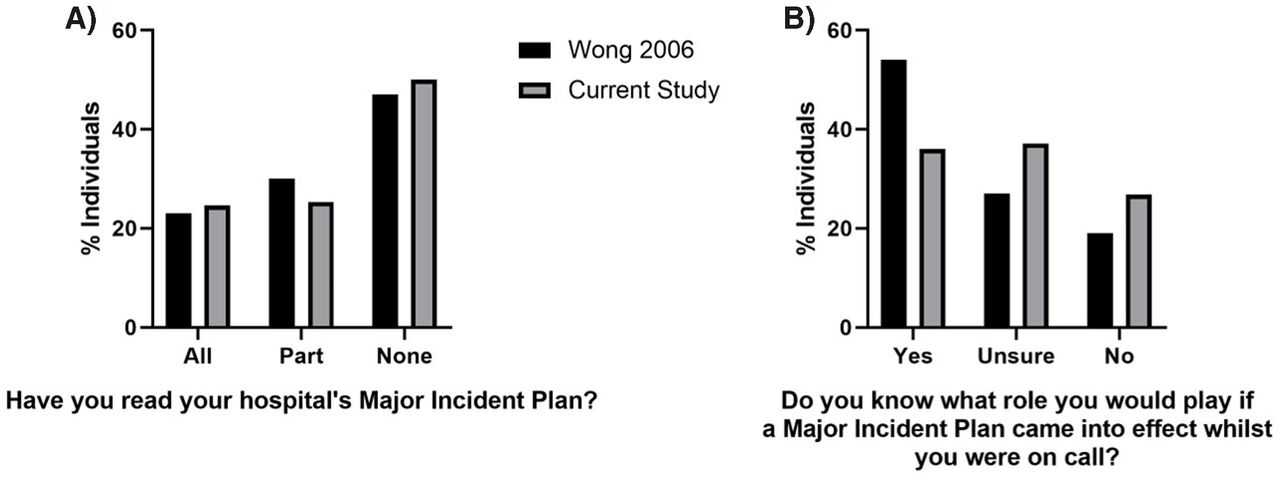
Comparison of results with our previous study (Wong et al 3). (A) Responses to ‘Have you read your hospital’s Major Incident Plan?’; 23% vs 24.7% had read all, 30% vs 25.3% had read part, and 47% vs 50.0% had read none (Wong et al 3 vs current study, respectively). (B) Responses to ‘Do you know what role you would play if a major incident plan came into effect while you were on call?’; 54% vs 36.0% responded yes, 27% vs 37.1% were unsure, and 19% vs 26.9% responded no (Wong et al 3 vs current study, respectively).
Discussion
Since 2004 all hospitals in England have been required to keep an MIP, and the importance of planning for such events has been exemplified in recent tragedies. We did not investigate the content of the MIPs as this would not be practical. Instead the purpose of this study was to assess the propagation and effectiveness of this information, and how it is understood by the individuals it involves rather than an evaluation of the MIP itself. We found that just half of the doctors contacted had read their hospital’s guidelines. Of concern, we found no improvement since 2006: indeed fewer individuals were confident in the role they would play if an MIP came into effect while they were on call. Perhaps unsurprisingly, emergency medicine registrars were the most familiar with their hospital’s protocol. They were closely followed by anaesthetics, with surgical specialties being least familiar. Importantly, doctors had no prior warning of our contact, as would be the case in the real-life enactment of an MIP.
Limitations
The response rate for the study was 63%. A major issue was being connected to the correct individual via the telephone switchboard system; for feasibility it was necessary to limit each potential participant to two call attempts. This may mean ‘busier’ individuals were less represented in our results, although it is likely that our selected group would be representative of the whole. We also found that some individuals were reluctant to answer questions over the phone and found it inappropriate for us to be contacting them in this manner. However, this method allowed us to ensure we were speaking to the correct person and ascertain the individual’s ‘spot response’. We did not routinely collect data on why individuals refused to answer, although some were reluctant to discuss such matters with individuals outside of their own trust.
The study concentrated on registrars, who at the time would likely have been in the position of leading the emergency response. However, major trauma centres are moving towards 24/7 consultant cover, so registrars may be less likely to lead the response in future.
Recommendations
A number of methods may be employed to improve dissemination of MIPs. Some hospitals produce ‘action cards’ to summarise roles for key individuals, and we recommend these are also included in staff induction packs (clinical or otherwise) nationwide (online supplementary figure 3).5 7 We also encourage simulation and specialist seminars, especially at ‘high risk’ hospitals. Some individuals (who tended to be from major trauma centres) had taken part in ‘disaster drills’, and those who did reported that these were very beneficial. Other research has investigated the use of virtual training environments and simulators, a practice which is likely to increase with further technological developments and the advent of augmented reality.8
Supplemental material
We will also be investigating the possibility of introducing this survey methodology as a regular audit and hope that other NHS trusts will do the same, partly to address the issue of individuals being reluctant to take calls from outside their own trust.
We would like to emphasise that our aim in completing this study was not to demean an already overstretched workforce but to assess how successful our approach to major incident preparation is as an organisation and what remains to be done.
Conclusion
We have demonstrated that confidence in using MIPs among registrars in England has not improved since 2006. We have made several suggestions, including the addition of succinct action cards in all trust inductions.
Supplementary materials
Press release
Press release
Footnotes
Contributors JAM planned the study, collected data for the study, performed data analysis and wrote the manuscript. HWR planned the study, collected data for the study and reviewed the manuscript. GAJS and SRT collected data for the study and reviewed the manuscript. TDC designed the study, oversaw the running of the study and reviewed the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.
Linked Articles
- Commentary