Article Text

Abstract
The Scottish Transfusion and Laboratory Support in Trauma (TLST) group previously audited all National Code Red activations between June 1st 2013 and October 31st 2015, generating a number of recommendations to be adopted to optimise the transfusion support given to patients following major trauma in Scotland. A repeat audit was undertaken for all patients for whom a Code Red was activated between 1st November 2015 and 31st December 2017.
A clinical and transfusion lead for each centre entered anonymised data onto a secure electronic database (REDCAP; http://www.project-redcap.org) the server of which is held within the University of Edinburgh. This database was maintained by the Edinburgh study team. Each of Scotland’s pre-hospital trauma teams who take patients to hospitals where Code Red Policy is in place, and the receiving hospitals, agreed to enter data into the National Code Red audit for all patients for whom a Code Red was activated during the study period. The project was deemed a service evaluation by the South East Scotland Research Ethics committee (Ref: NR/1408AB11) and therefore did not require full ethics submission. The project was also registered with each hospital’s clinical effectiveness/governance teams where available, and a favourable Caldicott opinion was obtained.
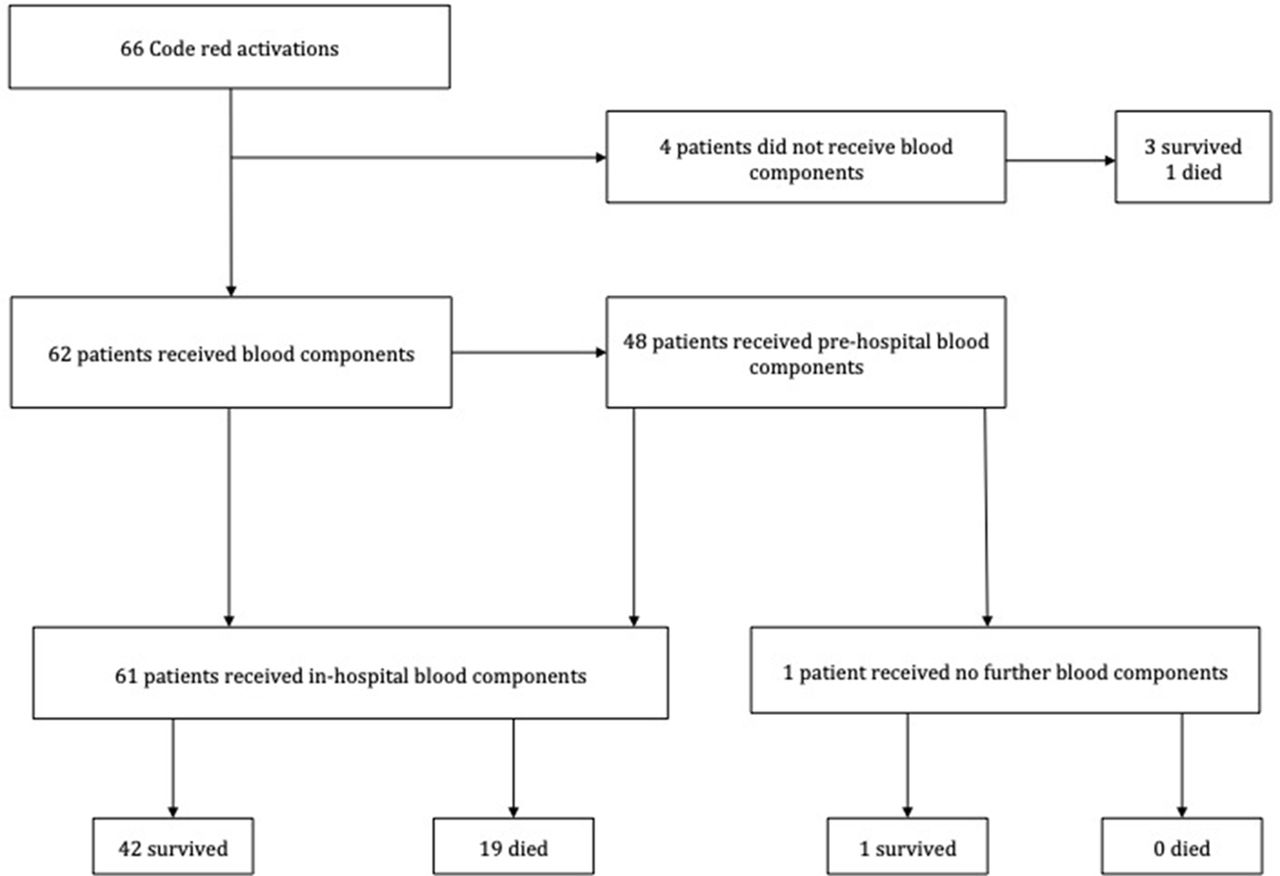
Flow chart showing transfusion events and outcomes of code red patients

{kind=link}
{kind=link}
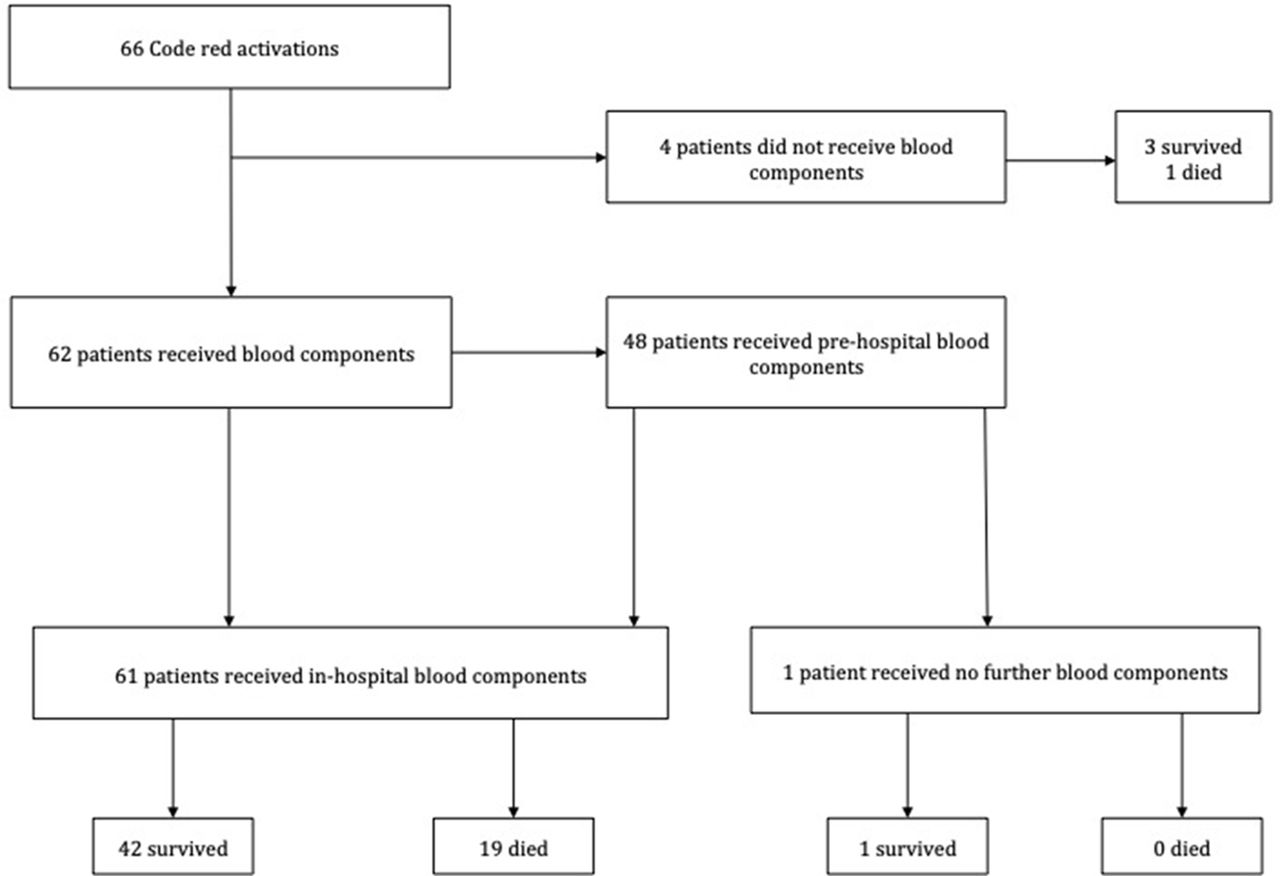
Ratio of the mean number of concentrated red cells (CRC) and fresh frozen plasma (FFP) transfused to code red patients at 30 minute intervals
66 activations (24 South-East of Scotland, 32 West, 10 East). Mean age 45 years, 88% male patients. 93% of Code Red patients received blood components with a 300% increase in pre-hospital transfusion (48 patients; 73%); median time from 999 call to Code Red activation reduced to 37 minutes from 70 minutes; 78% patients received pre-hospital TXA (improved from 70%). CRC:FFP ratios improved in comparison to 2013–15. Survival to discharge increased (63% to 66%) despite increased ISS.
Code Red practice has improved since our last audit. There are still improvements to be made in TXA administration and time to blood products.