Article Text

Abstract
Background There is a pressing need for emergency care (EC) training in low-resource settings. We assessed the feasibility and acceptability of training frontline healthcare providers in emergency care with the World Health Organization (WHO)-International Committee of the Red Cross (ICRC) Basic Emergency Care (BEC) Course using a training-of-trainers (ToT) model with local providers.
Methods Quasiexperimental pretest and post-test study of an educational intervention at four first-level district hospitals in Tanzania and Uganda conducted in March and April of 2017. A 2-day ToT course was held in both Tanzania and Uganda. These were immediately followed by a 5-day BEC Course, taught by the newly trained trainers, at two hospitals in each country. Both prior to and immediately following each training, participants took assessments on EC knowledge and rated their confidence level in using a variety of EC skills to treat patients. Qualitative feedback from participants was collected and summarised.
Results Fifty-nine participants completed the four BEC Courses. All participants were current healthcare workers at the selected hospitals. An additional 10 participants completed a ToT course. EC knowledge scores were significantly higher for participants immediately following the training compared with their scores just prior to the training when assessed across all study sites (Z=6.23, p<0.001). Across all study sites, mean EC confidence ratings increased by 0.74 points on a 4-point Likert scale (95% CI 0.63 to 0.84, p<0.001). Main qualitative feedback included: positive reception of the sessions, especially hands-on skills; request for additional BEC trainings; request for obstetric topics; and need for more allotted training time.
Conclusions Implementation of the WHO-ICRC BEC Course by locally trained providers was feasible, acceptable and well received at four sites in East Africa. Participation in the training course was associated with a significant increase in EC knowledge and confidence at all four study sites. The BEC is a low-cost intervention that can improve EC knowledge and skill confidence across provider cadres.
- emergency care systems
- acute care
- education
- global health
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this subject
There is a significant need for emergency care in low-resource settings, where people suffer from lack of access to timely care and high rates of mortality. Many courses aiming to train providers in these settings are limited by availability of trainers, equipment or cost.
What this study adds
This quasiexperimental pretest and post-test study suggests that the WHO-ICRC Basic Emergency Care course can be implemented in low-resource settings by locally trained providers with local equipment at a low cost.
Introduction
Every day, people seek care for health emergencies. Over 50% of mortality worldwide can be attributed to emergency medical conditions.1 In low-resource settings, the need is particularly great: 90% of injury related deaths occur in low-income and middle-income countries (LMICs), and patients in LMICs suffer the highest rates of mortality from acute complications of chronic diseases.2 3 Overall, 54% of annual deaths in LMICs could be potentially addressed by emergency care (EC), suggesting an opportunity to improve these outcomes.4 Recognising this need, the World Health Assembly Resolution 72.16 called for increased efforts to strengthen the provision of EC, including training.5
Improving patient outcomes for emergency medical conditions requires several conditions to be met including: patient awareness of an emergency medical condition, ability to seek emergency medical care, access to a medical facility capable of providing EC and high-quality care in the emergency unit.6 7 Patients in LMICs face barriers within each of these conditions. Emergency service utilisation rates are extremely low in low-income countries (8 per 1000 population) when compared with high-income countries (264 per 1000 population).8 In one review, 192 emergency facilities were identified in 59 LMICs; in the USA alone, there are roughly 5000 emergency facilities.9 Utilisation and access to a health facility does not guarantee access to quality EC. Overall mortality rates have been estimated to be extremely high in LMIC emergency units (EUs): 1.8% as compared with 0.04% in the USA.9 10 Paediatric mortality in LMIC EUs has been estimated to be even higher at 4.8%.9 Quality of care can be poor due to a lack of resources and variability in provider training.11
In order to strengthen EC delivery in resource-limited settings, the World Health Organization (WHO), in collaboration with the International Committee of the Red Cross (ICRC) and the International Federation for Emergency Medicine (IFEM), developed the Basic Emergency Care (BEC) course in 2015, a 5-day intensive training course covering core EC content, including didactics, practical skills and small groups.12 Participants are taught a systematic (ABCDE) approach to use for every patient encounter and review signs and symptoms and management of life-threatening conditions during the chief complaint-based modules: shock, trauma, difficulty in breathing, and altered mental status. Content is delivered via didactics and small group exercises. A significant portion of the course is dedicated to practical skills stations that re-emphasise the systematic ABCDE approach. The course is designed to be taught by local providers who have previously taken the course and attended an additional 2-day train-the-trainer course after completing the BEC. Here, we describe an early implementation of the BEC Course in two East African countries using a train-the-trainer model.
Methods
Study setting and participants
The BEC Course was implemented in two hospitals in Tanzania and two hospitals in Uganda during March and April of 2017. The implementation was performed with the support of the African Federation for Emergency Medicine (AFEM) in collaboration with the national emergency medicine societies and Ministries of Health of both Tanzania and Uganda. The emergency medicine society leads in each country participated in the development of the BEC Course and identified participating hospital sites based on their high volume of emergency visits, location on major roads and support of hospital leadership. All sites provide EC services, and at all sites these services are delivered in a less formal manner than the standard emergency unit staffed by non-rotating personnel who have received specialised training in trauma and acute care found in high-income countries.
The two participating hospitals in Uganda were Kawolo District Hospital and Mubende Regional Referral Hospital. Kawolo and Mubende are located 40 km and 170 km, respectively, from the nearest tertiary care facility in Kampala. In Tanzania, the two participating hospitals were Kisarawe District Hospital and Bagamoyo District Hospital. Kisarawe and Bagamoyo are located 42 km and 65 km, respectively, from the nearest tertiary care facility in Dar-es-Salaam.
Exposure variable
Participation in BEC Course
The delivery of the intervention in each country followed the same two-step implementation. First, local providers who participated in a BEC pilot course the previous year participated in a 2-day training-of-trainers (ToT) course, qualifying them to become trainers of the BEC Course. The ToT courses were taught by international faculty involved in the development of the BEC Course and the country leads. These local trainers then delivered the 5-day BEC training to frontline providers who participate in the delivery of acute and emergency medical care. All phases of the intervention were supported in person by a representative of the national emergency medicine society, physicians who participated in the development of the BEC Course and support personnel from AFEM.
BEC Course participants were required to attend all sessions, and attendance was taken. The schedule of the course is shown in figure 1. In all, the course involves 8 core lectures, 6 small group sessions and 25 practical skills taught in six skills stations.
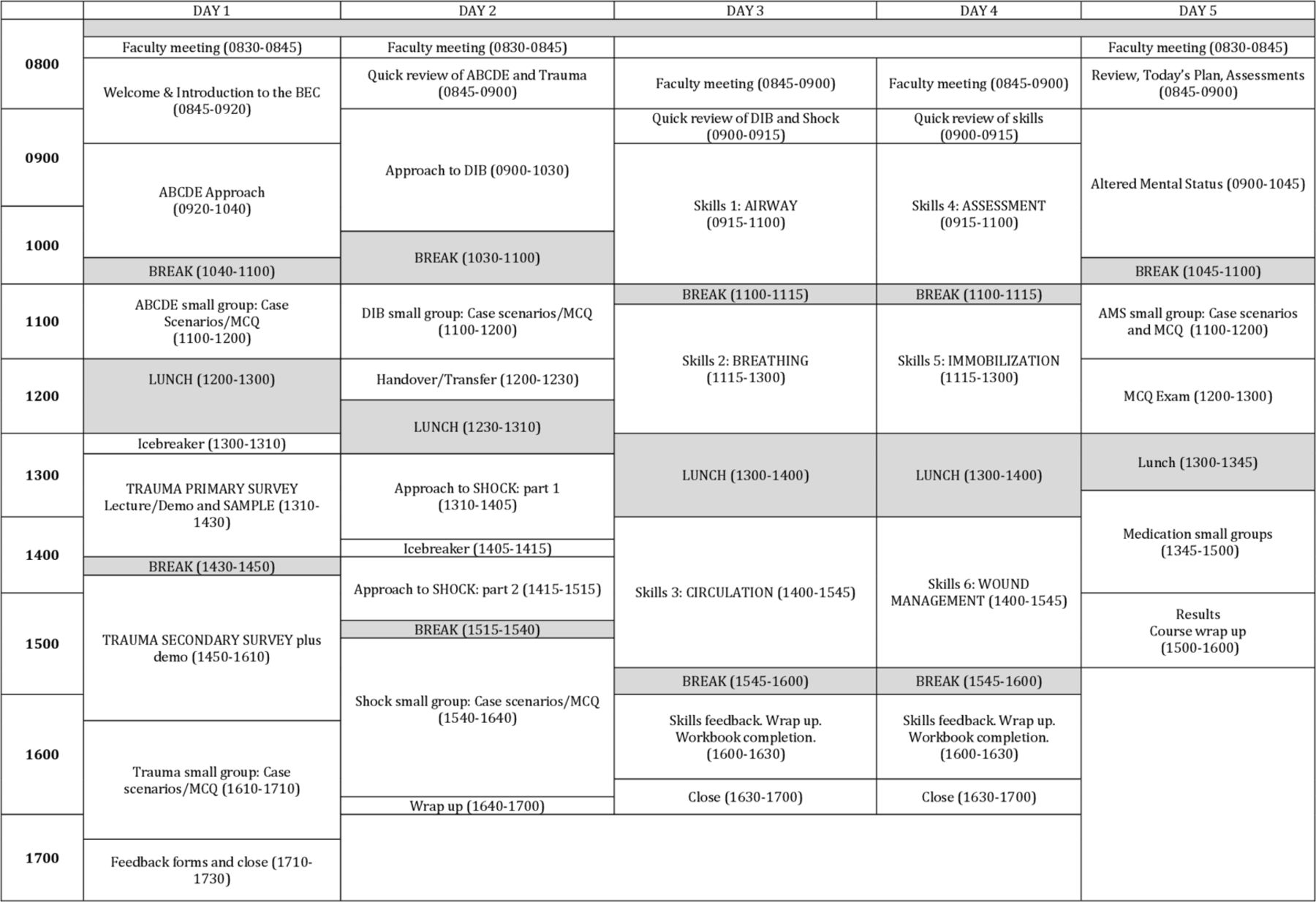
Standard schedule for the 5 day BEC course.
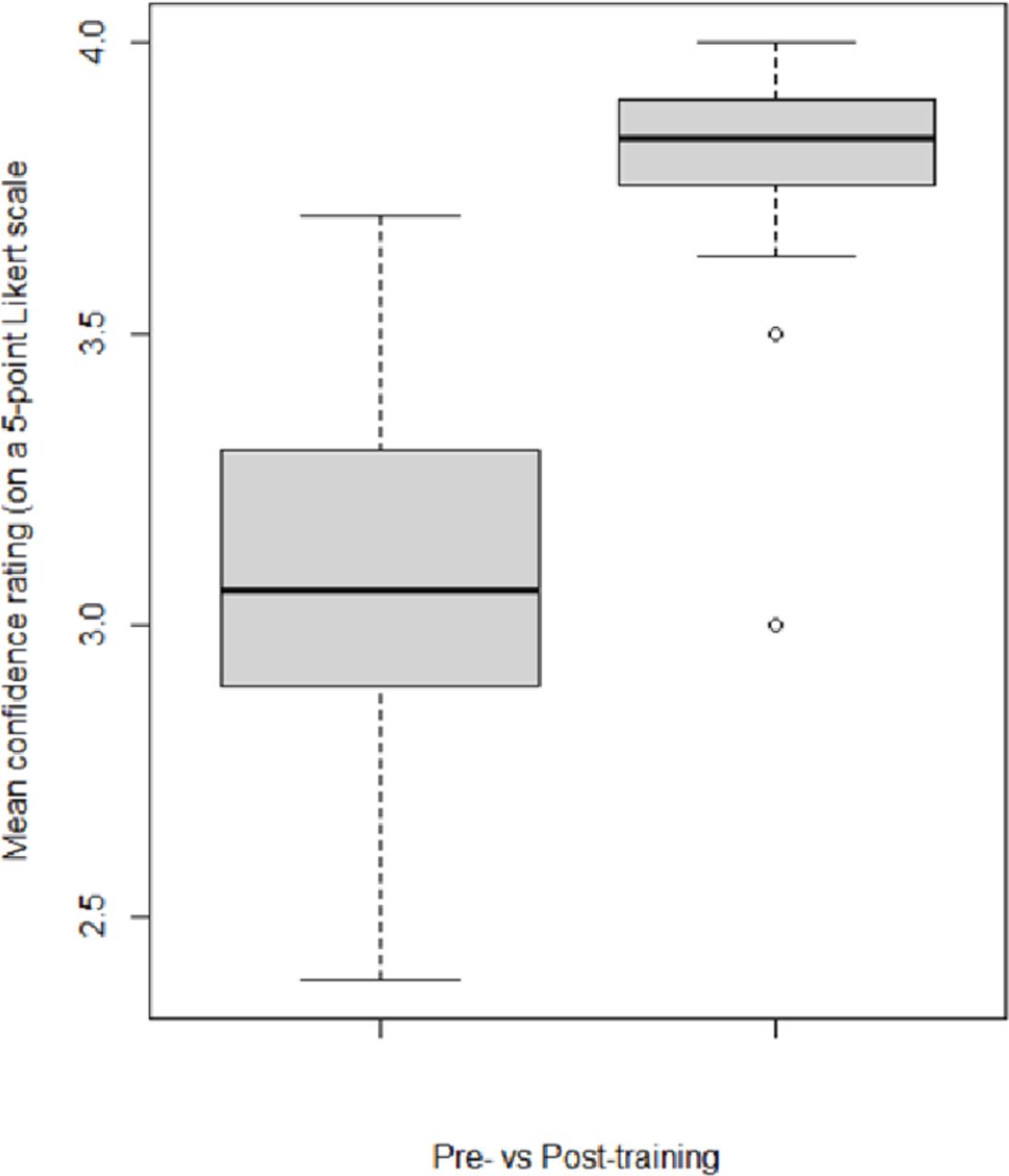
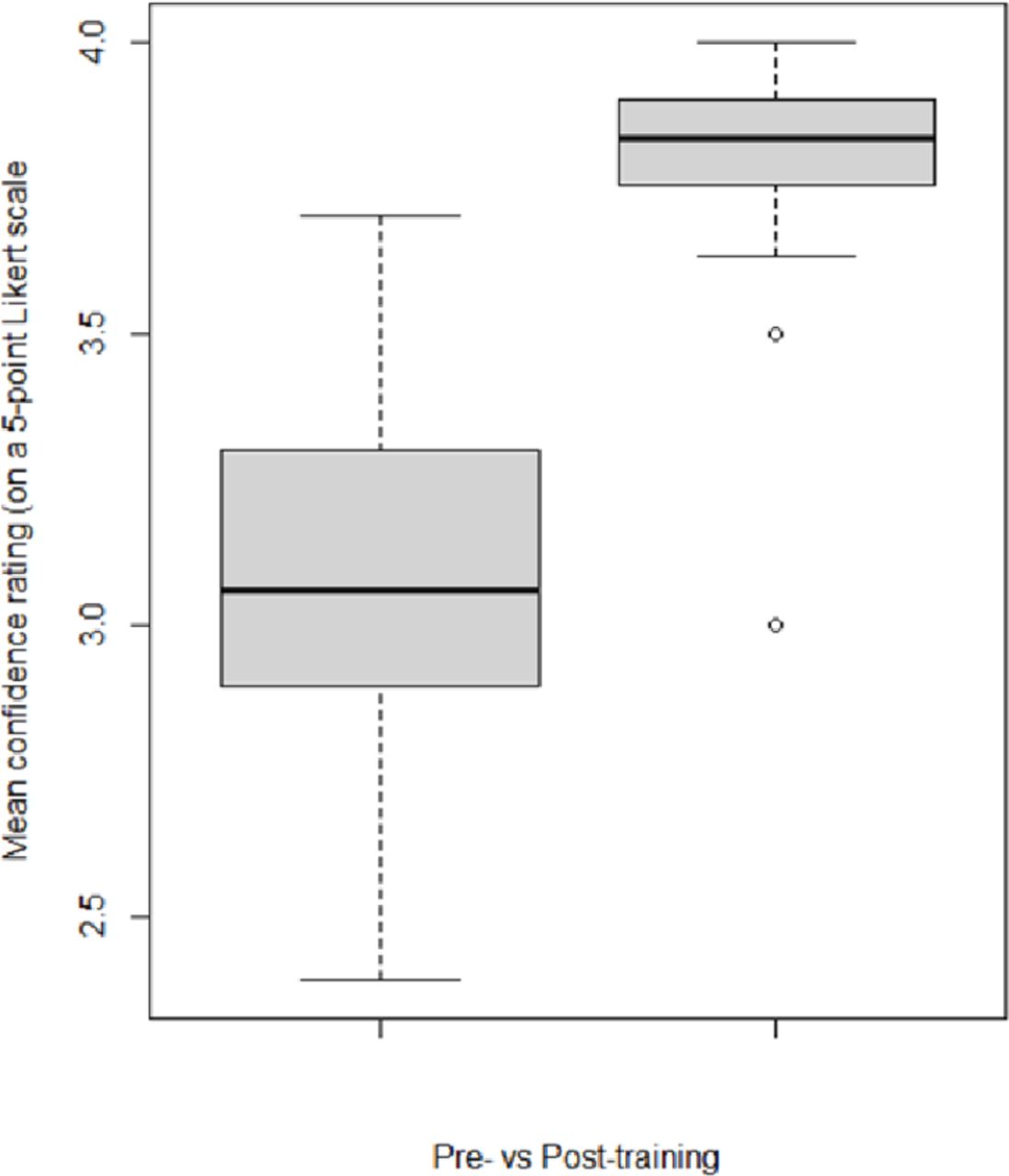
Effect of training on confidence in EC skills. EC, emergency care.
Outcome variables
A multimethod approach was used to evaluate implementation including an assessment, confidence ratings and feedback surveys. These evaluative tools and their content were developed by the WHO and are a standardised part of the BEC Course package. R V.4.0.1 was used for all statistical analyses; code available on request.13
EC knowledge score
Each participant completed a 25-question multiple choice assessment immediately prior to and following the course covering core concepts in BEC. The Wilcoxon sign-ranked test was used, due to non-normality, to assess the difference in the median number of questions answered correctly (called EC knowledge score) for each participant on the assessments completed before and after the training. The data are matched by participant.
EC confidence rating
Each participant also completed a confidence rating questionnaire immediately prior to and following the course. Participants rated their confidence in completing 12 EC actions on a Likert scale of 1 (least confident) to 4 (most confident) (online supplemental appendix 1). The paired samples t-test was used to assess the difference between the mean confidence rating before and after training. Individual responses were not retained at all study sites, precluding the Wilcoxon sign-ranked test from being used to calculate medians or to match based on participant. However, the mean confidence rating for all participants at each of the four study sites for each of the 12 EC actions was available and was matched by skill and site.
Supplemental material
Course feedback
Participants completed structured feedback forms immediately after each BEC module, each block of skills training and the conclusion of the course. Postcourse qualitative data were collected as free text and descriptively analysed by frequency and content of responses. We used the SQUIRE checklist when writing our report.14
Cost analysis
The reported costs of implementing the ToT and BEC courses are the actual expenditures from the project budget. Costs were tracked by site and reported by budget line item, total cost per site and cost per participant.
Patient and public involvement
The BEC Course was developed in response to an identified public need for EC training applicable to low-resource settings by the WHO and its member states. The study sites, research questions and outcome measures were informed by the priorities and experience of local healthcare providers in Tanzania and Uganda. Local study participants were paid a per diem rate. Local healthcare providers, including the public, will be involved in the dissemination of study results through local and regional advocacy groups.
Results
Course participants
Ten participants completed the ToT course: seven in Uganda and three in Tanzania. A total of 59 participants completed the BEC Courses. Forty-six per cent of participants were nurses, 32% doctors and 22% other cadres (table 1). Overall course attendance, taken daily, was 97%.
Trainee roles
Multiple choice assessment
When assessed across all sites, the median number of questions answered correctly on the 25-question EC knowledge assessment was five points higher on the post-training assessment than on the pretraining assessment (Wilcoxon sign-ranked test, z=6.23, p<0.001). When assessed by country, the same median increase of five questions was observed for both Uganda and Tanzania as was seen when assessed overall (table 2 and figure 2). When assessed by study site, the median increase in number of correct answers ranged from a three-question improvement at Kawolo District Hospital and at Mubende Regional Hospital to an eight-question improvement at Bagamoyo District Hospital. Two participants did not complete both the pretest and post-test and were excluded from analysis.
Change in median number of questions answered correctly on the EC knowledge assessment using the Wilcoxon sign-ranked test matched on individual scores

{kind=link}
{kind=link}
{kind=link}
Effect of training on EC knowledge scores. EC, emergency care.
Confidence rating
Confidence in EC skills also improved significantly at all sites with a mean improvement of 0.74 points (95% CI 0.63 to 0.84) and ranging from a 0.38 to 1.05 absolute increase on a 4-point Likert scale (paired t-test, t=14.19, df=47, p<0.001). The largest improvements were seen at Kawolo and Bagamoyo District Hospitals (table 3 and figure 3). The same significant increase in mean confidence rating was observed when assessed by site and by country. The data met the requirements necessary for use of the t-test; the sample size was sufficiently large (n=48 for overall test) and the assumption of normality was satisfied for the difference between pretraining and post-training (Shapiro-Wilk test of normality p=0.24, kurtosis=0.20, skew=−0.39). For the two sites where individual responses were retained, a Wilcoxon sign-ranked test demonstrated a similarly significant improvement in median confidence ratings matched by participant (online supplemental appendix 2).
Supplemental material
Testing the change in mean confidence rating for 12 EC skills using a paired t-test matched on the mean confidence rating per question per site
Qualitative themes/responses
Course feedback
Eighty-six per cent (51/59) participated in the postcourse survey. Ninety-five per cent (19/20) of participants from Uganda returned feedback on the overall course and 82% (32/39) participants from Tanzania provided postcourse feedback. Participants were asked the following questions: (1) what the participants liked about the course, (2) what participants learnt in the course, (3) what participants would change in the course, (4) who participants would recommend the course to and (5) open-ended additional feedback. Overall, the course was wellreceived by the participants at both the Ugandan and Tanzanian sites. Comments representative of the most frequent feedback and from a diversity of sites and cadres are presented in table 4.
Illustrative comments representative of the most common responses to the feedback questions
When asked what they liked and/or learnt from the course, 51.0% (26/51) of participants mentioned the ABCDE approach. While other topics such as shock, trauma or SAMPLE (Signs and Symptoms, Allergies, Medications, Past Medical History, Last Oral Intake, and Events Surrounding the Injury or Illness) survey were mentioned, the ABCDE approach stood out as the most mentioned topic. Of this group, 34.6% (9/26) specifically stated they liked the ABCDE approach, and 84.6% (22/26) specifically mentioned ABCDE as something they learnt from the course. A percentage of 39.2 of participants (20/51) stated that they most enjoyed the skills aspect of the training. Immobilisation, shock and general skills and knowledge in taking care of the emergency patient was the next most cited area of learning from the course followed by topics of trauma, wound care and airway management. A percentage of 25.5 (13/51) of participants stated that the BEC taught them how to better manage emergency patients. Others enjoyed how the course was facilitated as well as the materials provided. A few appreciated that the course was taught in both Swahili and English at the Tanzanian sites.
The most frequent suggestion for improvement was increased time for the course (21.5%, 11/51), while others stated that they would not change anything about the course (13.7%, 7/51). Other suggestions for course changes included training more people, sessions on ectopic pregnancy and other obstetric topics and more skills sessions. Most participants felt that this training should be provided to all health providers including nurses and doctors. Many also stated that police officers should also receive this training (17.6% 9/51). Others stated that all support staff such as security, cleaners and administrators should take this course. Many participants used the open-ended feedback to share that they were planning to apply what they learnt to their clinical work.
Costs
Ten trainers were trained at an average cost of US$335 per participant (range $228–$442). Fifty-nine healthcare providers were trained at an average cost of $237 per participant (range $171–$344). The average overall site cost was $1461 (range $1325–$1596) for the ToT course and $3394 (range $1711–$4419) for the BEC Course. Major budget components were for meals (21% of total budget for ToT and 34% for BEC), daily per diem reimbursement for the participants (34% for ToT and 19% for BEC) and per diem for local trainers (23% for ToT and 16% for BEC) (table 5). Skills equipment was loaned for free from local EC agencies, and space was donated at some sites but required payment at others. Printing was a nominal cost.
Cost (all costs are in US$)
Discussion
This was the first full implementation of the WHO-ICRC-IFEM Basic Emergency Care course, at four hospitals in East Africa, taught by local healthcare providers who completed a ToT course. All sites showed significant improvement in both participant EC knowledge and confidence in performing EC skills after completing the course. Our results were consistent across both parametric and non-parametric statistical tests. The course was well received by participants and supported by hospital administration. Strengths of this study include the recruitment of local healthcare providers to train frontline EC providers at the implementation sites. Attendance was near perfect, and all but two post-tests were completed. Course skills were taught with locally used equipment, often on loan from the facility hosting the training. Ideally, training occurs at the host facility in donated space. Main feedback themes were: an increase in knowledge and skills, positive reception and recall of the ABCDE approach, recommendation to teach the BEC Course to all healthcare workers, an ability to manage sick patients, a willingness to incorporate lessons learnt into actual management and the need for more time to complete the training. Feedback collected was reported to the WHO to inform future course revisions.
The BEC Course is designed to strengthen EC systems by improving the quality of care delivered with existing human and material resources in a low-cost and context-appropriate manner. This study demonstrates that the BEC Course can be implemented in a low-resource setting at a low cost by local trainers. Per diem rates for instructors and participants vary by country and will affect the cost of an implementation, and by extension, sustainability. These rates are set by local governments and emergency medicine societies and may incentivise participation in the course to a higher level than would otherwise be attained. In this experience, the per diem rates were substantially higher in Tanzania than in Uganda. Additionally, costs such as printing, equipment and space will vary by location and affect the cost of implementation. Implementation costs can be lowered with scaling of the ToT programme and subsequent elimination of international faculty expenses. Experienced trainers are eligible to lead future ToTs through a process supported by IFEM.15 Additional training courses can then be held regionally by these local trainers with minimal to no external support further decreasing the cost of each course.
Our study shared strengths found in the implementation of related courses. Implementation of Emergency Triage Assessment and Treatment (ETAT) in Rwandan district hospitals was similarly successful and shared challenges we encountered: intensity of training in a short time period, large clinical responsibilities of students making it difficult to free up time and language barriers.16 17 Similar to our qualitative findings, a study in Tanzania showed that the understanding and perception of EC improved at hospitals without formal emergency units after a short training course on EC.18 A survey on use of the WHO Pocket Book of Hospital Care for Children in Indonesia found challenges with printing and distributing materials despite systematic mailings of the book by the WHO and Ministry of Health.19 While the local EC societies were able to assist in printing and distributing manuals for this implementation, the cost of printing remains a challenge for any future courses. BEC skills are taught using locally sourced equipment and medications, exposing students to the same items used in clinical practice while reducing the supply challenges faced in some other trainings.20 21
This study has limitations, including the lack of an evaluation of impact on patient outcomes, lack of long-term follow-up of knowledge and skill retention and limited data analysis options due to data inconsistencies between sites. The analysis for the confidence ratings is a compromise based on running the best analysis possible with the pooled dataset from both countries. The results, however, are still strongly significant for the pooled dataset, and for further substantiation of our results, an additional analysis was performed on the more complete subset of data (online supplemental appendix 2). Impact on the quality of actual patient care was not assessed due to cost; however, future research will assess this. A late evaluation of knowledge was not completed due to cost. International faculty were required for course implementation and support because this was an early implementation and there was limited availability of local or regional trainers. As an increased number of providers are trained it is expected that the need for international faculty will be reduced or eliminated, improving sustainability and generalisability. These BEC Courses were held immediately after the ToT courses. As the number of trainers grows, there may be increased time separation between ToT courses the BEC Courses that newly trained trainers teach, which could adversely impact quality.
Future research should evaluate the impact of the BEC Course on patient outcomes and EC process measures. Additionally, the BEC Course should be tested for validity in settings outside of East Africa and across different languages as translations occur. Finally, long-term knowledge and skill retention should be evaluated though structured follow-up.
Conclusion
Implementation of WHO-ICRC BEC by local provider-trainers was feasible, acceptable and well received at four sites in East Africa. Knowledge assessment scores and trainee confidence increased significantly at all sites. The BEC is a low-cost intervention that can improve knowledge and skill confidence across provider cadres.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
This project was considered exempt by the Partners Human Research Committee and was approved by the Uganda Ministry of Health and the Tanzania President’s Office.
Acknowledgments
We would like to thank the African Federation for Emergency Medicine, the Emergency Medicine Association of Tanzania and Emergency Medicine Uganda for their logistical support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Richard Body
Twitter @Sean_Kivlehan
Presented at An early version of this manuscript was published as a preprint at https://doi.org/10.21203/rs.2.19074/v1.
Contributors SK, JD, HS, JK, LW and TAR contributed to the design of the study. SK, JD, EC and JR collected and analysed data. SK drafted the manuscript. All authors critically reviewed and edited the article and have approved this final version.
Funding This work was supported by the Esther B. Khan Young Investigator in Emergency Medicine Award and a Research Seed Grant, both administered by the Department of Emergency Medicine at the Brigham and Women’s Hospital in Boston, Massachusetts, USA.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.