Article Text

Abstract
Objective To compare the efficacy of continuous positive airway pressure (CPAP) versus usual care for prehospital patients with severe respiratory distress.
Methods We conducted a parallel group, individual patient, non-blinded randomised controlled trial in Western Australia between March 2016 and December 2018. Eligible patients were aged ≥40 years with acute severe respiratory distress of non-traumatic origin and unresponsive to initial treatments by emergency medical service (EMS) paramedics. Patients were randomised (1:1) to usual care or usual care plus CPAP. The primary outcomes were change in dyspnoea score and change in RR at ED arrival, and hospital length of stay.
Results 708 patients were randomly assigned (opaque sealed envelope) to usual care (n=346) or CPAP (n=362). Compared with usual care, patients randomised to CPAP had a greater reduction in dyspnoea scores (usual care −1.0, IQR −3.0 to 0.0 vs CPAP −3.5, IQR −5.2 to −2.0), median difference −2.0 (95% CI −2.5 to −1.6); and RR (usual care −4.0, IQR −9.0 to 0.0 min-1 vs CPAP −8.0, IQR −14.0 to −4.0 min-1), median difference −4.0 (95% CI −5.0 to −4.0) min-1. There was no difference in hospital length of stay (usual care 4.2, IQR 2.1 to 7.8 days vs CPAP 4.8, IQR 2.5 to 7.9 days) for the n=624 cases admitted to hospital, median difference 0.36 (95% CI −0.17 to 0.90).
Conclusions The use of prehospital CPAP by EMS paramedics reduced dyspnoea and tachypnoea in patients with acute respiratory distress but did not impact hospital length of stay.
Trial registration number ACTRN12615001180505.
- prehospital care
- clinical management
- respiratory
- ventilation
- non invasive
- respiratory
- COPD
Data availability statement
No data are available. Current ethics approvals do not include sharing of individual patient data. However, it may be possible to share aggregated results on reasonable request.
Statistics from Altmetric.com
Key messages
What is already known on this subject
Acute respiratory failure, presenting as dyspnoea, is a common reason for patients to contact emergency medical (ambulance) services.
Non-invasive positive pressure ventilation techniques such as continuous positive airway pressure (CPAP) provide ventilatory support without the need for an (invasive) endotracheal tube, and is commonly used in the hospital setting as a treatment for acute respiratory failure and alleviating respiratory distress.
The current evidence base for the efficacy and safety of the use of CPAP by emergency medical service (EMS) paramedics is limited by observational studies and small clinical trials.
What this study adds
Our large prehospital randomised controlled trial showed that the use of CPAP by EMS paramedics was more effective than usual care in reducing dyspnoea and tachypnoea in patients with acute respiratory distress, with no increased risk of adverse outcomes.
CPAP is a safe and effective prehospital intervention for symptom management in patients with acute respiratory distress.
We recommend CPAP to be included as an option for managing dyspnoea in selected patients in the clinical practice guidelines of EMS.
Introduction
Acute respiratory failure (ARF), presenting as dyspnoea, is a common reason for patients to contact emergency medical (ambulance) services (EMS).1 It may arise from a variety of cardiorespiratory conditions,2 such as acute pulmonary oedema (APO), asthma and chronic obstructive pulmonary disease (COPD). Current EMS guidelines in our jurisdiction (Western Australia) recommend optimising patient positioning, titrated oxygen therapy and specific management options directed at the underlying disease,3 such as bronchodilators for COPD and glyceryl trinitrate for APO.4
Non-invasive positive pressure ventilation (NIPPV) techniques such as continuous positive airway pressure (CPAP) provide ventilatory support without the need for an (invasive) endotracheal tube and have been increasingly used in the hospital setting as a treatment for ARF and alleviating respiratory distress.5 Some EMS (eg, Ambulance Victoria, Australia) have introduced the use of CPAP by paramedics in the prehospital setting. However, the evidence of efficacy is limited by mostly observational studies and small clinical trials, and remains inconclusive, particularly in EMS without direct physician support, or across the spectrum of underlying pathology.6 The objective of this study was to assess whether the prehospital use of CPAP by paramedics reduces breathlessness (dyspnoea score and RR) and reduces hospital length of stay in patients with severe respiratory distress attended by EMS.
Methods
Study design and setting
This individual patient, parallel group randomised controlled trial (RCT) was conducted by St John (Ambulance) Western Australia (SJ-WA) in the greater metropolitan area of Perth and selected rural areas in Western Australia (WA). SJ-WA is a single-tier ambulance service that is the sole provider of emergency road ambulances in WA. There were 170 331 ambulance attendances in the Perth metropolitan area in the year ending 30 June 2018, 83% of which were deemed emergency/urgent.7 Within metropolitan Perth (and the rural areas involved in this study), SJ-WA ambulances were staffed by two crew members, at least one of whom was a qualified (3-year University Bachelor degree) paramedic.7 The WA population in 2017 was 2 574 193 and 1 165 850 (45.3%) were aged 40 years or older, and 2 037 902 (79.2%) lived in the capital city of Perth.8 Patients enrolled in the study were transported to one of the nine metropolitan (adult) EDs or five rural acute hospitals.
Selection of participants
Enrolment commenced on 5 March 2016 and concluded 31 December 2018. Patients were screened for eligibility by the attending study paramedic. Patients were eligible for enrolment if they were aged >40 years, with acute severe respiratory distress (as defined by the St John WA Clinical Practice Guideline (CPG) for Dyspnoea & Respiratory Distress)9 of non-traumatic origin, had a RR of >22 breaths/min and were unresponsive to at least 5 min of initial treatment. Patient ‘responsiveness’ was assessed by paramedics based on the overall patient condition, including improvement in the dyspnoea score, reduced RR and improvement in oxygen saturation, guided by the St John CPG relating to respiratory distress.9 Patients were excluded if they had reduced consciousness (only responsive to Pain or Unresponsive)10; a systolic BP <90 mm Hg; were being uncooperative; or thought to have a possible pneumothorax, anaphylaxis, drowning, smoke inhalation, aspiration or pregnancy.
Interventions
Randomisation and masking
Patients were randomly assigned (1:1) to CPAP (intervention) or usual care. A computer-generated randomisation sequence using block randomisation (with variable block size) was generated (TW). Allocations were concealed by placing them in sequentially numbered, opaque, sealed, tamper-evident envelopes. Randomisation was achieved by the trial paramedic opening the envelope after eligibility was confirmed. The trial was ‘open label’ as it was not possible to conceal treatment allocation to the patient or trial paramedic after randomisation. The research nurse (NM) extracting the trial outcome data from clinical records was not blinded to allocation because she had access to the patient’s treatment record indicating whether CPAP was delivered or not.
Procedures
A total of 195 paramedics volunteered to recruit patients into the RCT (approximately 25% of the SJ-WA paramedic workforce). Study paramedics received 4 hours of face-to-face training, which included implementation of the study protocol, recognition of the inclusion/exclusion conditions, the practical use of CPAP and accurate recording of the outcome measures. CPAP was provided using the Flow-Safe II CPAP mask (Mercury Medical, Florida, USA). This disposable, oxygen-driven CPAP system provides positive airway pressures of between 2 and 12 cm H2O according to the oxygen flow rate. The pressure delivered to the patient is displayed through a manometer built into the mask. Patients in the CPAP group were commenced on 10 cm H2O CPAP. The level of CPAP was titrated in 1 cm H2O increments according to the patient’s response. Response was assessed according to peripheral oxygen saturations, RR and patient comfort. As per the SJ-WA CPG11 for oxygen therapy, the target peripheral oxygen saturation (SpO2) was 88%–92% for patients with known COPD and 94%–96% for those without a history of COPD. CPAP was reduced to 5 cm H2O if the patient became hypotensive. CPAP was discontinued if the patient was unable to maintain their airway, systolic BP fell to <90 mm Hg, the patient could not tolerate the mask, vomiting occurred, the patient no longer responded to voice indicating decreased consciousness level or a suspected pneumothorax developed. Otherwise, treatment continued until arrival at the ED.
Both the intervention and the control groups received the standard medical care for the presumed underlying condition in accordance with the relevant SJ-WA CPG,12 which included titrated oxygen plus: glyceryl trinitrate for APO; salbutamol±ipratropium bromide nebulised for COPD and asthma; and intramuscular epinephrine for life-threatening asthma.12
Measurements and outcomes
The primary patient-centred outcomes were (1) change in RR and (2) change in dyspnoea score (patient-defined using a Visual Analogue Scale (VAS): 0–10 cm). The recruiting paramedic recorded on the study card the patient’s initial score and final score (immediately prior to ED arrival) for RR and the dyspnoea score. Paramedics participating in the trial were advised to use the Dyspnoea VAS in a similar manner to the pain score.13 If the initial or final RR or dyspnoea score were missing from the study card, the values were imported from the electronic patient care record (e-PCR). The health system centred primary outcome was hospital length of stay.
Secondary outcomes were oxygen saturation (pulse oximetry), prehospital care duration (minutes from EMS arrival on scene until ED arrival), intubation prior to discharge from ED, intensive care admission, adverse events, and in-hospital and 30-day mortality (the latter ascertained from WA death records). In-hospital outcomes were obtained from medical record review by the study research nurse (NM) for patients transported to one of the participating metropolitan hospitals.
Analysis
We initially determined that only 60 patients were required in each group (intervention and control). However, to ensure sufficient power for subgroup analyses, we undertook preliminary analysis (applying similar study inclusion criteria to an earlier cohort of patients) to determine the likely frequency of subgroups. The three most common paramedic-determined problem codes were APO, COPD and respiratory infections, with the least common of these (respiratory infections) having a frequency of 16%. With the aim of having sufficient power for the subgroup analysis of APO, COPD and respiratory infections, we determined the total sample size required for the least common subgroup to comprise 60 patients. For this calculation, we rounded the frequency of the minimum subgroup of interest to 1/6. Thus, we planned to recruit 360 patients for each of the intervention and control groups (ie, so that for each arm of the study, 1/6 × N=60, where N is the target sample size).
A planned single blinded interim analysis was conducted at the midway point of the study (2017) and did not invoke the Haybittle-Peto interim stopping rule.14
Baseline characteristics were reported as counts (n) with percentages (%) for categorical variables and medians with IQR for continuous variables. Outcome differences between treatment and control groups were tested using the Mann-Whitney U test for continuous variables and χ2 test for categorical variables. The median differences (and 95% CI) were calculated using the Hodges-Lehmann estimate.15 We performed intention-to-treat analyses.
Because there was no way for the study paramedics to check prior study enrolment, it was anticipated that there might be some patients who were recruited more than once over the study period. A sensitivity analysis was therefore conducted to compare outcomes if only the first (index) randomisation was used. An ‘a priori’ subgroup analysis of patients with APO, COPD and respiratory infection was also conducted. All data analyses were conducted using IBM SPSS Statistics (V.24; SPSS).
Ethics approval
Approval was obtained from the Curtin University Human Research Ethics Committee (HREC) (#HR220/2015) for the prehospital RCT with waiver of consent; and HREC approval with waiver of consent for the in-hospital medical record review follow-up was obtained from each of the participating metropolitan hospitals, with the following lead sites: Sir Charles Gairdner and Osborne Park Healthcare Group (HREC 2016-148); Joondalup Health Campus (Ref 1715); and St John of God Midlands (Ref 1477).
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting or dissemination plans of our research. However, this will be rectified for future Prehospital, Resuscitation and Emergency Care Research Unit (PRECRU) studies.
Results
Characteristics of study subjects
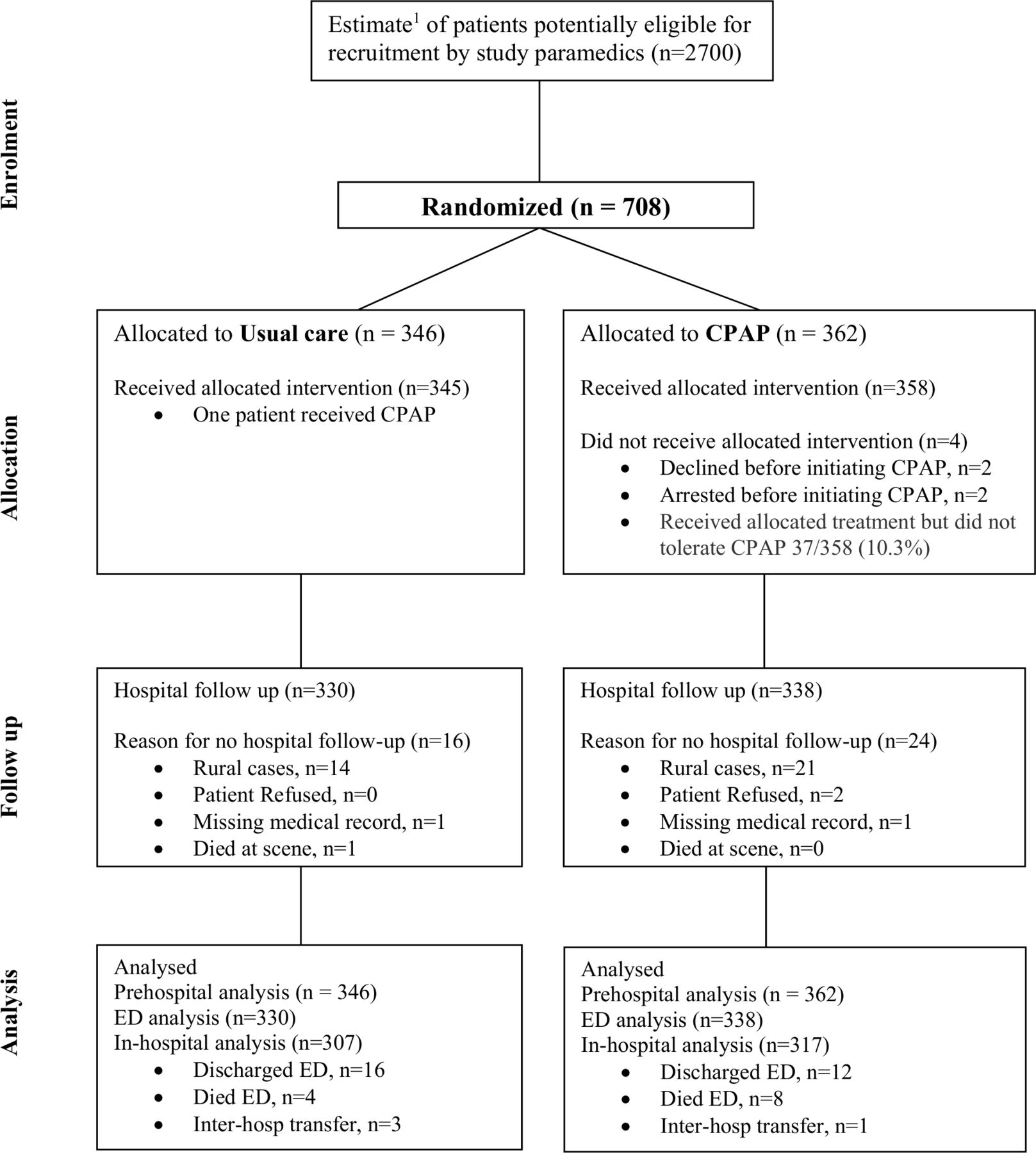
A total of 708 patients were assigned to either usual care (n=346) or CPAP (n=362) (figure 1). The median age of the study participants was 77.3 (IQR 68.3–84.3) years, with 56% males. A total of 668 patients (usual care 330; CPAP 338) recruited in the metropolitan area had in-hospital follow-up (see figure 1). A total of 47 patients were recruited in the study more than once, hence the sensitivity analysis consisted of 661 index cases.
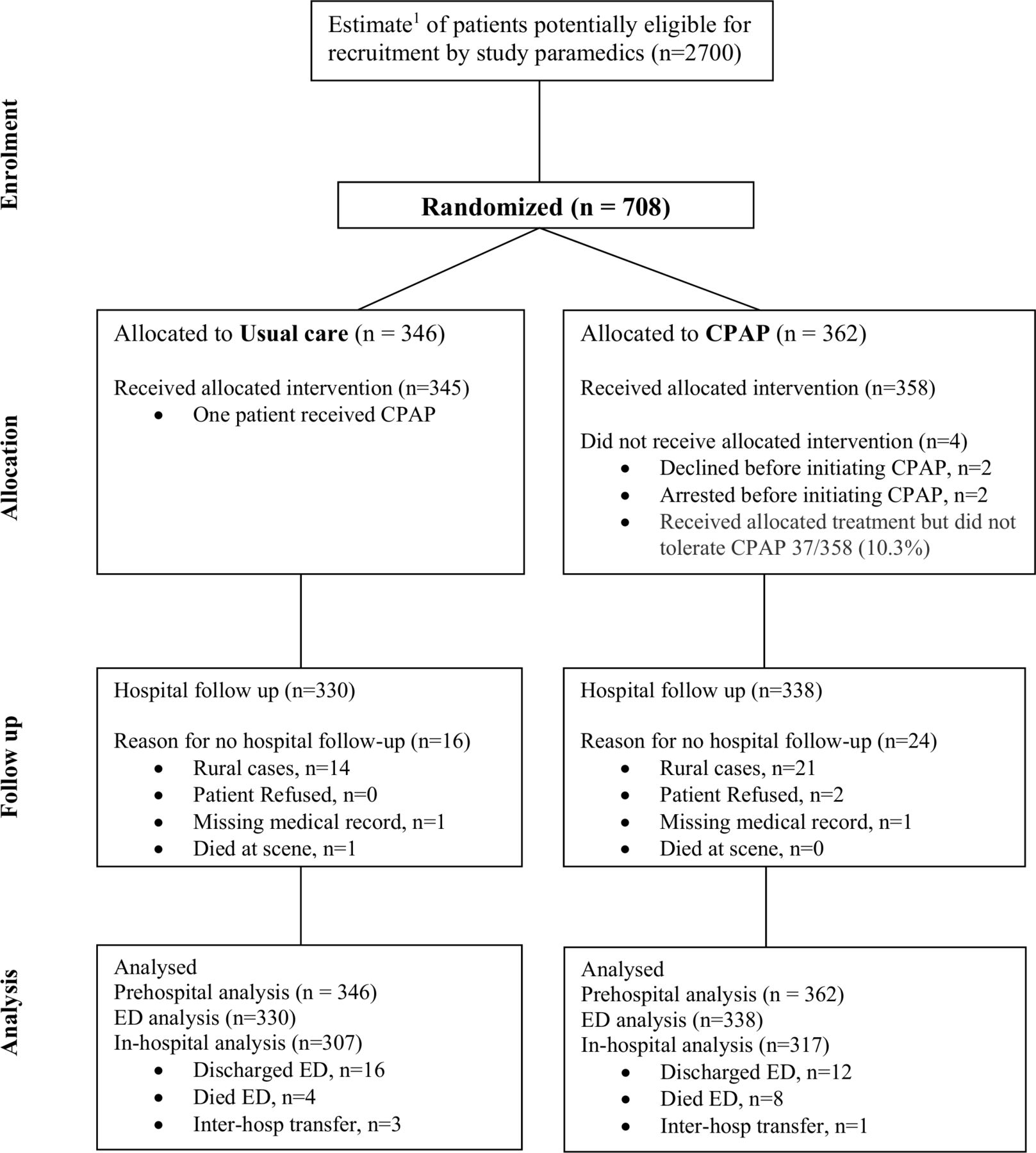
CONSORT (Consolidated Standards of Reporting Trials) flow diagram. 1Estimation based on (total of number of patients attended during the study period) minus (interhospital transfers, patients aged less than 40 years, RR<=22/min or GCS<15 or BP<90 mm Hg, cases with a problem code other than APO, COPD, asthma, respiratory infection or other respiratory problem), divided by 4 (since only 25% of the paramedics participated in the study). APO, acute pulmonary oedema; COPD, chronic obstructive pulmonary disease; CPAP, continuous positive airway pressure, n, represents the total sample number.
Of the 362 patients allocated to the CPAP group, 4 (1.1%) did not receive CPAP (2 improved and 2 deteriorated before mask application). Of the 358 patients who had a mask applied, 37 (10.3%) did not tolerate CPAP and had it removed (prehospital) after undocumented periods of time. Of these 37 patients, the only details recorded for 19 were ‘unable to be tolerated’. Of the remaining 18, the stated reason for removal of the mask was as follows: n=8 patient anxiety/claustrophobia; n=7 the patient’s condition deteriorated; n=2 mask unable to be fitted due to face size or skin cancers; and one due to nausea. Of the 346 cases allocated to usual care, 1 patient (incorrectly) received CPAP.
There were no important differences between the study groups in baseline characteristics nor initial observations (table 1). The initial dyspnoea score was rated as severe in both groups (median VAS of 9, IQR 8–10); and most patients (86.0%; 95% CI 83.5% to 88.6%) had severe tachypnoea, with an RR ≥30 per minute. Similarly, the initial SpO2 was indicative of significant hypoxaemia, with a median SpO2 of 85.0% (IQR 78.0%–90.0%). The two most common prehospital presenting problems (as determined by the paramedics) were APO (31.9%) and COPD (30.1%), with a similar distribution between the treatment groups.
Baseline characteristics of patients by treatment group
Main results
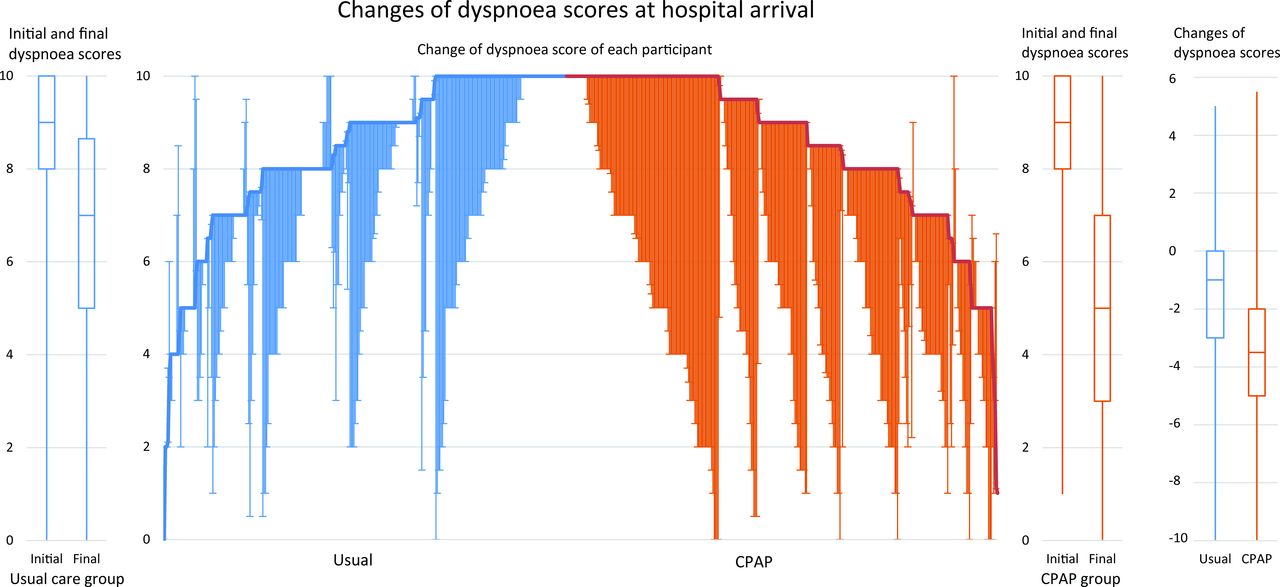
The main results are displayed in table 2 (prehospital outcomes), table 3 (in-hospital outcomes) and figure 2 (hybrid parallel line plot of dyspnoea score reduction).
{kind=link}
{kind=link}
Change of dyspnoea scores at hospital arrival. The drop lines show the initial and final dyspnoea score of each participant on the verbal rating scale (0–10) in ascending order of the initial dyspnoea score for the usual care group and in descending order for the continuous positive airway pressure (CPAP) group. The thick lines indicate the initial dyspnoea scores. The box plots beside the drop lines depict the dyspnoea score at the initial and final assessments for the group, whereas the box plots to the right of the graph summarise the change in dyspnoea score for each group.
Comparison of PREHOSPITAL primary and secondary outcomes by treatment group (N=708)
Comparison of IN-HOSPITAL primary and secondary outcomes by treatment group (N=668)
Primary and secondary outcomes
For the primary outcomes, patients randomised to CPAP had a greater reduction in dyspnoea score (ie, less difficulty breathing) at ED arrival (median change −3.5, IQR −5.2 to −2.0) compared with those randomised to usual care (median change −1.0, IQR −3.0 to 0.0), median difference=−2.0 points (95% CI −2.5 to −1.6) (table 2). Figure 2 illustrates this greater reduction in dyspnoea scores in the CPAP group compared with the usual care group. There was also a greater reduction in RR in the CPAP group compared with the usual care group at ED arrival (table 2). At baseline, the percentage of patients with an RR of >30 per min was comparable in both groups, whereas at ED arrival 46.7% of patients in the CPAP group had an RR of >30 per min compared with 64.2% in the usual care group; −17.5% difference (95% CI −24.7% to −10.3%). There was no clinically important difference in the median (IQR) hospital length of stay for the CPAP group (4.8 days; 2.5 to 7.9) compared with the usual care group (4.2 days; 2.1 to 7.8), median difference 0.36 days (95% CI −0.17 to 0.90) (table 3).
The results for the primary outcomes were consistent with those of the overall study even if the study cohort was restricted to only index cases (online supplemental tables 1 and 2) or only those patients admitted to hospital (online supplemental table 3). Similarly, results in each of the subgroups (APO, COPD and respiratory infection) were consistent with the overall study (online supplemental table 4).
Supplemental material
For the secondary outcomes (table 2), oxygen saturation improved at ED arrival in both groups, and there was no clinically meaningful difference between the groups. Intubation rates were low in both groups (total of 22 cases). Although twice as many patients in the usual care group (4.5%) were intubated than in the CPAP group (2.1%), the difference was not statistically significant. As shown in table 3, of the 624 patients admitted to hospital, there was no significant difference in the percentage of patients admitted to intensive care unit (ICU); nor was there any difference in survival to discharge (CPAP 89.0% vs usual care 89.3%) or death within 30 days (CPAP group 16.1% vs usual care group 14.0% table 3). While the median time from arrival at the scene to arrival at ED was slightly longer in the CPAP group (37 min) than the usual care group (35 min), it is not likely to be clinically important.
Adverse events
Adverse clinical events were rare. There were 2 out of 362 (0.56%) prehospital cardiac arrests in the CPAP group; one before CPAP was commenced, the other after the mask was applied. In the usual care group, 3 out of 346 (0.87%) sustained a cardiac arrest in ED. There were two cases of pneumothorax diagnosed in ED (both in CPAP patients). One patient was receiving bilevel NIPPV in ED at the time the pneumothorax was diagnosed. There was no suggestion in the medical record of either case that the pneumothorax was caused by the prehospital CPAP.
Discussion
In this prehospital RCT, CPAP use by EMS paramedics was more effective in reducing dyspnoea and tachypnoea in patients with acute respiratory distress than usual care. While twice as many patients in the usual care group were intubated (4.5%) than in the CPAP group (2.1%), the overall intubation rate (n=22; 3.3%) was very low and the percentage difference between groups was not significantly different (−2.4%; 95% CI −5.1 to 0.3). There were no differences in clinical complications, hospital mortality or hospital length of stay.
There have been several RCTs of CPAP use in the prehospital setting, which have been summarised in systematic reviews.6 16 17 The reviews varied in the types of studies that were included, and the underlying causes of ARF. The Goodacre network meta-analysis6 included six prehospital CPAP studies with participant numbers ranging from 36 to 207. This showed that prehospital CPAP substantially reduced mortality (in-hospital or 30 days) compared with standard care in patients with ARF (OR=0.41; 95% credible intervals (CrI) 0.20 to 0.77). However, of the six studies included in the network meta-analysis,6 only two small studies18 19 showed a significant difference between treatment groups. Of note, four of the studies were conducted in centres with physician-staffed EMS but it was only the two paramedic-staffed studies18 19 that showed a significant difference in mortality rates.
More recently, a small pilot study20 conducted in the UK randomised 77 patients with ARF to prehospital CPAP versus standard oxygen therapy. While the study was underpowered to detect differences in the primary outcome (30-day mortality from ARF), the mortality in both study groups was higher than expected (27.3% vs an estimated 12%). The authors concluded that it was not feasible to conduct a larger study in the context of the NHS ambulance services. However, they did note that ‘CPAP could also affect important patient-centred outcomes such as symptom relief, which might be detected by differences in dyspnoea VAS scores’.20
We did not find any indication of differences in mortality between the treatment groups (15% vs 16%) in our study. While intubation rates were low in each of the studies included in the Goodacre et al 6 review, similar to our study, they all showed at least double the number of intubations in the usual care group compared with the CPAP group. Indeed, the Goodacre et al 6 network meta-analysis showed a significant reduction in intubation in the CPAP group compared with the usual care group (OR 0.32; 95% CrI 0.17 to 0.62).
We chose, a priori, to use a patient-centred outcome of dyspnoea as our primary outcome rather than ‘intubation’ or ‘mortality’. The American Thoracic Society acknowledges the utility of dyspnoea measures as patient-reported endpoints for clinical trials2 and states that as with pain, adequate assessment of dyspnoea is a subjective experience that requires self-report.2 In addition to having particular relevance to patient comfort, dyspnoea scores have been shown to predict hospital admissions, in-hospital mortality and early readmission in acute exacerbations of COPD.21 As such, it has been argued that dyspnoea scores are an appropriate primary outcome measure for prehospital research in patients with respiratory distress.22 Furthermore, intubation numbers are so low that large study recruitment numbers would be required to ensure adequate study power.
As reported for other EMS,3 the current SJ-WA CPG recommend a standard management approach for the treatment of ARF, supplemented by specific management options directed at the underlying disease.4 However, we have shown that in the prehospital setting, it can be difficult to determine the differential diagnosis underlying a patient’s respiratory distress.23 As previously suggested,23 it may be more pragmatic to have a single CPG for the clinical management of respiratory distress. Based on our current study results, this should include the option of using CPAP.
Limitations
Our study has several limitations. First, the RCT was conducted in a single (although large) EMS staffed by paramedics in a predominantly metropolitan setting. This may impact on external validity for other EMS with different settings/staffing profiles (eg, physician-led).24 Second, only some paramedics (around 25%) volunteered to contribute to the study. While there is no reason to suspect these study paramedics differed in any meaningful way from those who did not volunteer, there is the possibility that outcomes might be different if the trial were to have involved all paramedics. Third, neither the intervention nor in-hospital data extraction was blinded and hence there was a risk of observer bias. Training of the study paramedics (and research nurse) emphasised the importance of accurate documentation of outcomes to ensure internal validity of the study.25 Furthermore, the study was not powered for the secondary outcomes, particularly of intubation, ICU care or mortality.
While a strength of our study is that we do have in-hospital follow-up for most cases, there was a small proportion (5.6%) of cases who were not followed up (mostly rural cases). There was no difference in the baseline characteristics of the rural versus metropolitan cases; and when analysed as a separate subgroup, the rural cases alone similarly produced significant differences in both primary outcomes, that is, improved dyspnoea score and reduced tachypnoea (results not shown). While there were a very small number of missing values for the primary outcome of change in RR (0.3%), there were more missing values for the change in dyspnoea scores (8%). However, the characteristics of patients with and without missing dyspnoea scores were similar (online supplemental table 5).
A further limitation is that there was incomplete recording of timing of CPAP mask placement and removal. This made the assessment of two initially defined secondary outcomes in the study protocol, namely, ‘duration of CPAP (prehospital)’ and ‘continuation of CPAP in ED for at least 30 min’ impossible to report. Finally, it was not possible to ascertain the total number of patients who were assessed for inclusion in the study because we did not ask paramedics to keep records of patients who they considered might have been suitable for enrolment in the study or not.
Conclusions
The use of CPAP by EMS paramedics was more effective than usual care in reducing dyspnoea and tachypnoea in patients with acute respiratory distress, with no increased risk of adverse outcomes. There was no difference in hospital length of stay or mortality between the treatment groups. This study adds to a growing body of evidence that CPAP is a safe and effective prehospital intervention for symptom management in patients with acute respiratory distress.
Data availability statement
No data are available. Current ethics approvals do not include sharing of individual patient data. However, it may be possible to share aggregated results on reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
Ms Alani Morgan for coordination of HREC approvals and manuscript formatting. St John Western Australia CPAP study paramedics for recruitment and randomisation of patients.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Caroline Leech
Twitter @judith_finn, @CCREM2, @EM_VATA
Contributors TW and DB were responsible for identifying the research question and TW drafted the initial study protocol for the randomised controlled trial (RCT). TW, JF, GA, DF, BM, GDP, DH, PB, QS and DB contributed to further development of the RCT study protocol and were all listed as investigators on the (successful) grant application for funding for the in-hospital follow-up. TW and DB undertook the training of the paramedics who volunteered to participate in the study. DB, PB and AG oversaw the conduct of the prehospital RCT and AG collected the ambulance data. GA, DF, AC, AM and BS enabled access for the in-hospital patient follow-up, which was undertaken by NM. GP undertook the interim analysis and subsequently advised on the statistical methods for the final analyses. HT analysed the data and produced the tables and figures. All authors contributed to data interpretation. JF was responsible for drafting the article. All authors provided comments on the drafts, read and approved the final version of the article. JF takes responsibility for the paper as a whole. All authors attest to meeting the four ICMJE.org authorship criteria: (1) substantial contributions to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work; and (2) drafting the work or revising it critically for important intellectual content; and (3) final approval of the version to be published; and (4) agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding Western Australian Department of Health, State Health Research Advisory Council (SHRAC) Research Translation Project funding—RTP2016R10. There was no external funding of the prehospital RCT—it was supported collaboratively by St John Western Australia and PRECRU at Curtin University. Funding for the in-hospital follow-up was provided by the Western Australian Department of Health, State Health Research Advisory Council (SHRAC) Research Translation Project funding. The funder of the study had no role in study design, data collection, data analysis, data interpretation or writing of the report; nor did the manufacturer of the CPAP masks.
Competing interests Several of the authors are affiliated with St John Western Australia, as follows: DB, AG, PB (employees); JF, SB (adjunct research positions); JF (research funding).
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.