Article Text

Abstract
Aims, Objectives and Background Corticosteroids can be used to treat idiopathic facial paralysis (Bell’s palsy) in children, but their effectiveness is uncertain.
Aims To determine if prednisolone improves recovery of children with Bell’s palsy at one month.
Method and Design Double-blind, placebo-controlled, randomised, trial of prednisolone in children presenting to ED with Bell’s palsy.1Patients 6 months to <18 years, recruited <72 hours after symptom onset, were randomly assigned to receive 10 days of treatment with oral prednisolone (1 mg/kg) or placebo. The primary outcome: complete recovery of facial function at 1 month on the House-Brackmann scale.2 Secondary outcomes: facial function, adverse events and pain to 6 months.
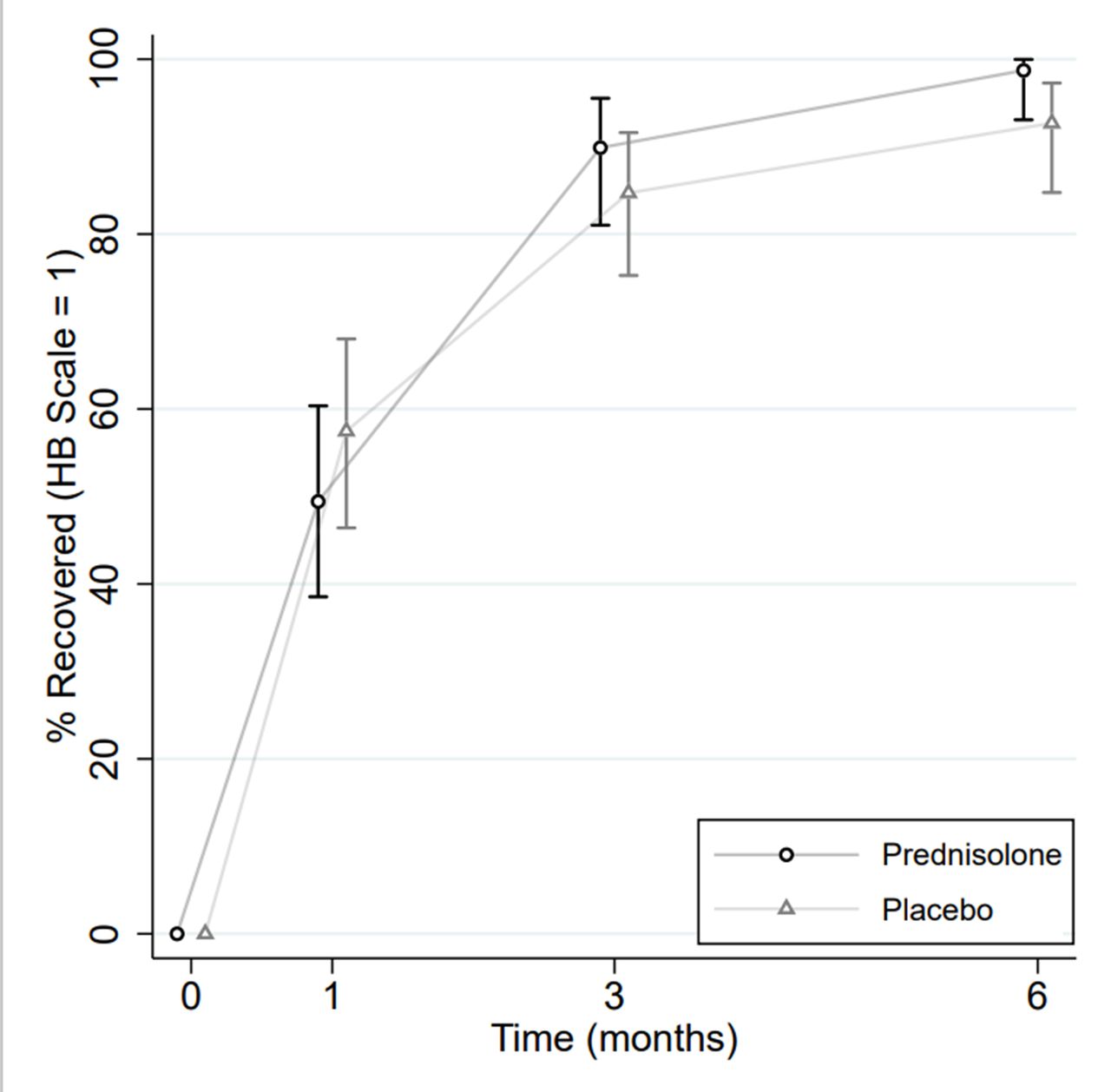
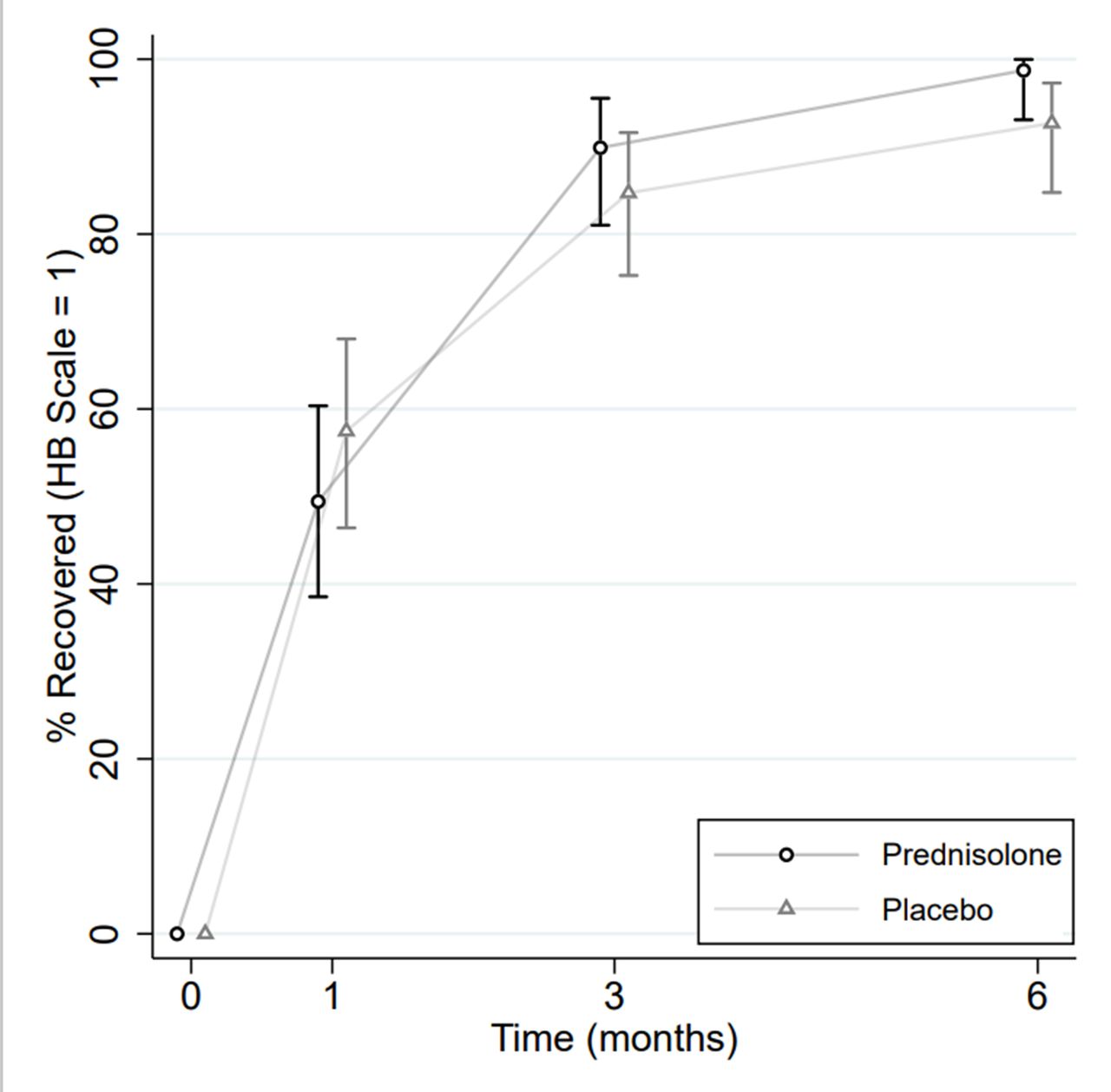
Results and Conclusion Between October 2015 to August 2020, 187 children were randomised (94 to prednisolone and 93 to placebo) and included in the intention-to-treat analysis. At 1 month, the proportions of patients who had recovered facial function were 49% (n=43/87) in the prednisolone group compared with 57% (n=50/87) in the placebo group (risk difference -8.1%, 95% CI -22.8 to 6.7; adjusted odds ratio [aOR] 0.7, 95% CI 0.4 to 1.3). At 6 months these proportion were 99% (n=77/78) for prednisolone and 93% (n=76/82) for placebo respectively (risk difference 6.0%, 95% CI -0.1 to 12.2; aOR 3.0 95% CI 0.5 to 17.7) (figure 1). There were no serious adverse events and little evidence for group differences in secondary outcomes.
{kind=link}
In children with Bell’s palsy the vast majority recover without treatment. The study does not provide evidence that early treatment with prednisolone improves complete recovery.
References
Sullivan F, Swan I, Donna P, Morrison J, Smith B, McKinstry B, et al. Early treatment with prednisolone or acyclovir in bell’s palsy. N Eng J Med 2007;357(16):1598–607.
House JW, Brackmann DE. Facial nerve grading system. Otolaryngol Head Neck Surg. 1985;93(2):146–7.