Article Text

Abstract
Objectives With the 'teach-back' method, patients or carers repeat back what they understand, so that professionals can confirm comprehension and correct misunderstandings. The effectiveness of teach-back has been underexamined, particularly for older patients discharged from the emergency department (ED). We aimed to determine whether teach-back would reduce ED revisits and whether it would increase patients’ retention of discharge instructions, improve self-management at home and increase satisfaction with the provision of instructions.
Methods A nonrandomised pre–post pilot evaluation in the ED of one Dutch academic hospital including patients discharged from the ED receiving standard discharge care (pre) and teach-back (post). Primary outcomes were ED-revisits within 7 days and within 8–30 days postdischarge. Secondary outcomes for a subsample of older adults were retention of instructions, self-management 72 hours after discharge and satisfaction with the provision of discharge instructions.
Results A total of 648 patients were included, 154 were older adults. ED revisits within 7 days and within 8–30 days were lower in the teach-back group compared with those receiving standard discharge care: adjusted odds ratios (AORs) of 0.23 (95% CI 0.05 to 1.07) and 0.42 (95% CI 0.14 to 1.33), respectively. Participants in the teach-back group had an increased likelihood of full knowledge retention on information related to their ED diagnosis and treatment (AOR 2.19; 95% CI 1.01 to 4.75; p=0.048), medication (AOR 14.89; 95% CI 4.12 to 53.85; p>0.001) and follow-up appointments (AOR 3.86; 95% CI 1.33 to 10.19; p=0.012). Use of teach-back was not significantly associated with improved self-management and higher satisfaction with discharge instructions. Discharge conversations were generally shorter for participants receiving teach-back.
Conclusions Discharging patients from the ED with a relatively simple and feasible teach-back method can contribute to safer and better transitional care from the ED to home.
- emergency department
- teach-back
- older adults
- discharge instructions
Data availability statement
Data are available upon reasonable request. The original quantitative SPSS datasets generated during and/or analysed during the study are available upon reasonable request from the corresponding author. Datasets will contain individual deidentified data of participants who gave written consent.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this subject
The use of the teach-back method showed positive effects on a variety of outcomes for different patient populations across inpatient and outpatient healthcare settings. This communication method is, however, largely underexamined for patients, particularly for older adults, discharged from the emergency department (ED).
What this study adds
Our pilot study suggests that teach-back in the ED is a feasible method that supports professionals in the ED with discharge communication with patients and carers. Teach-back is associated with improved retention of discharge instructions by older adults at home and findings indicate that teach-back may contribute to fewer short-term ED revisits. These findings warrant further investigation to provide more evidence for the structural implementation of teach-back in the ED.
Introduction
Providing patients and carers adequate discharge instructions is an important task of healthcare professionals to ensure a safe discharge from hospital to home.1 Educating patients and carers at discharge can, however, be challenging for professionals working in the emergency department (ED) due to various reasons. First, an ED visit is usually an unexpected and stressful event for patients. They often experience ongoing acute pain and fatigue and are worried about their health situation,2 3 which makes it difficult to concentrate on the provided information. Second, the ED can be a crowded and hectic working environment where discharge instructions are provided quickly and piecemeal in-between other care activities, thereby making it difficult for patients and carers to remember or reproduce them.4 5
Many studies have demonstrated that patients often leave the ED unprepared because of comprehension deficits in key information domains such as the diagnosis and cause, ED treatment, post-ED care and return precautions.6–10 The results from a cross-sectional analysis demonstrated, for example, that three out of four patients were unable to recall important information for at least one of these domains.6 Furthermore, patients may not recognise when they have limited understanding,6 11 suggesting an inability to seek help when needed. Incomprehension of discharge instructions has been associated with negative outcomes such as unmet needs,12 poor compliance,12–14 deterioration of health10 15 16 and increased use of health services postdischarge.10 15 16
A variety of strategies have been developed and tested to improve comprehension and recall of discharge instructions, primarily focusing on the content of the instructions and the method of delivery (eg, verbal, written, pictorial, video, telephone).1 8 Another improvement strategy is the ‘teach-back’ method, whereby patients or carers are asked to repeat back, in their own words or in demonstrations, the instructions that healthcare professionals provided them, so that full comprehension of the instructions can be confirmed, misunderstandings can be corrected and additional information can be provided if needed.17 18 As mentioned by Griffey and colleagues,11 the teach-back approach has a basis in cognitive psychology experiments showing that repeating short sequences of information helps to improve the recall of information.19–21 The use of the teach-back method showed positive effects on a variety of outcomes for different patient populations across inpatient and outpatient healthcare settings.18 22 23 However, this communication method has been largely underexamined for patients, particularly older adults, discharged from the ED. This is remarkable considering that older adults are extra vulnerable for not comprehending and retaining important discharge information due to cognitive, hearing and visual impairments.10 Older adults are also more prone to the negative consequences of comprehension deficits than their younger counterparts.10 24–28 With EDs as the common entry point to healthcare for the ever-increasing elderly population, the problem of poor patient comprehension of ED discharge instructions and related adverse outcomes are expected to increase further. Better insight into the effects of teach-back at ED discharge on service utilisation and on outcomes for older adults could help health professionals and policymakers decide whether or not to structurally implement this communication method as part of ED discharge care.
Therefore, our pilot study aimed to determine whether teach-back in the ED is feasible and might reduce (unplanned) ED revisits. In addition, we sought to determine whether teach-back would improve older patients’ comprehension and retention of discharge instructions, self-management at home and satisfaction with the provision of the discharge instructions. Besides evaluating the intervention effects, we conducted this pilot study to test the study logistics, to gain information for optimising intervention delivery and adherence and to obtain empirical evidence of study parameters to help design a future (larger) clinical trial.
Methods
Study design
We performed a nonrandomised, pre–post pilot study using the guide for Transparent Reporting of Evaluations with Nonrandomized Designs.29 The study was conducted from 1 March to 31 October 2019 and consisted of two phases: the preintervention phase (4 months) and the postintervention phase (4 months). The preintervention phase investigated data of patients who received standard discharge care (ie, the provision of verbal discharge instructions and preformatted written discharge information). The postintervention phase investigated data from patients who received teach-back in addition to the standard discharge care. The local medical ethical committee ‘CMO Arnhem-Nijmegen’ approved this study (identification number: 2019-5166). Deidentified data sets are available from the corresponding author on reasonable request.
Study setting and population
The study was performed in the ED of the Radboud University Medical Center (Radboudumc), an urban academic hospital with an annual ED census of 22 000 visits. We deliberately performed this study in a period when no major policy changes were scheduled that could have influenced healthcare delivery in the ED. Throughout the study period, we were alert to unexpected changes. We also chose this period to minimise the impact of seasonal effects on study group differences (eg, size and characteristics).
Two medical residents (NK and CT) scanned for potential eligible patients in consecutive order of appearance from Monday to Friday from 10 am to 7 pm. Eligible patients were identified in consultation with the ED triage nurse and the ED physician on duty after scanning the hospital information system (HIS). Patients were included if they were discharged from the ED to home, including outpatient-assisted living facilities such as a senior home or a rehabilitation centre. Patients unable to speak the Dutch language, discharged to another medical facility or ward or with a severe mental/cognitive impairment (eg, advanced dementia) without being accompanied by a caregiver at the ED were excluded from the study. In the postintervention phase, patients were only included if the use of teach-back was reported by a health professional through ticking off a check box in the HIS. Eligible patients were informed about the study and asked to participate before discharge instructions were given. Written informed consent was obtained from all patients or carers before enrolment.
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of our study.
Protocol
After completion of the preintervention phase, 1-week period was used for teach-back training and practice behaviour adoption for nurses, physicians and residents working in the ED. These professionals were informed about the study and the teach-back method via an online newsletter and the display of posters and information cards in the ED. NK, CT and one ED physician (OS), all familiar with the principles of teach-back, initially trained the professionals on using the teach-back method at discharge by demonstrations and role play. A pocket-size booklet with teach-back instructions was used for training purposes and functioned as a reminder on how to perform teach-back in clinical practice. For example, professionals were instructed to create a shame-free environment for teach-back (ie, to highlight that teach-back is not intended to test patient knowledge but is instead a method to enhance patient comprehension and recall of instructions) and to use plain language to facilitate understanding. Multiple individual and group training sessions were held to cover all nurses, physicians and residents working in the ED at that time. online supplemental file 1 illustrates the elements of the teach-back training. Additional training sessions in the postintervention phase were held for new employees, especially a large group of residents working for several weeks in the ED as part of their residency programme. In total, 37 ED nurses, 7 ED physicians and 37 medical residents were trained. During the postintervention phase, CT and NK randomly attended discharge conversations. For the subsample of older participants, all discharge conversations were attended. Immediate feedback to professionals was provided to enhance awareness of and improvement of teach-back.
Supplemental material
Outcome measures and sample size
The primary outcomes were ED revisits within 7 days and within 8–30 days postindex visit. Previous studies reported that teach-back can reduce hospital readmissions by 4%–12% for hospitalised patients at high risk of acute conditions.30 31 Based on these findings, the annual ED revisit rate within 30 days in our hospital,32 and taking into account that this study was performed in the ED setting, we estimated at least a 7% reduction in ED revisits from 14% to 7%. To achieve 80% power to detect this 7% difference in the primary outcome between study groups, with the two-tailed alpha set at 0.05, we calculated that a minimum of 300 patients in each study group would be required.
Secondary outcomes included older participants’ knowledge retention of discharge instructions across the five information domains, reported self-management at home and satisfaction the with discharge instructions provided by professionals in the ED.
Data collection
Medical chart review
Baseline data on age, sex, urgency level (based on the urgency classification levels of the Manchester Triage System; MTS), comorbidity level (based on the Charlson Comorbidity Index; CCI), polypharmacy (defined as ≥5 different types of prescribed medications), ED length of stay (LOS) and time of ED discharge were obtained from the patient’s electronic medical record (EMR) along with the noted discharge instructions. Furthermore, data about ED revisits within 7 days and within 8–30 days postindex visit were collected from the EMR.
Observation of discharge conversations
NK and CT attended discharge conversations between professionals and older patients (aged ≥70 years) or their carers. The duration of the discharge conversation was timed, and the provided instructions were noted according to a structured format (online supplemental file 2), focusing on five critical information domains: (1) ED diagnosis and treatment, (2) (prescribed) medication in the ED, (3) post-ED care (eg, wound care, lifestyle advice), (4) follow-up appointments (eg, with their general practitioner or another specialist) and (5) return precautions. They also noted whether patients were accompanied by an informal carer and if they were cognitively impaired at the moment of receiving discharge instructions (ie, signs of early stage dementia, poststroke, disorientation and confusion). Cognitive impairment was determined after reviewing relevant information in the medical records and observing the patient during the discharge conversation. Both researchers were trained in recognising predefined cognitive impairment conditions (ie, signs of early stage dementia, poststroke symptoms, disorientation, confusion).
Supplemental material
Telephone interview
NK and CT interviewed older patients or a carer via telephone within 72 hours after discharge from the ED. The conversations were audio recorded after receiving consent. First, a standardised question-based script was used to ask interviewees to state in their own words what discharge instructions were given (online supplemental files 3 and 4). Questions were open ended and interviewees were allowed to refer to their written discharge instructions. Knowledge retention of the instructions was determined by listening to the audio recordings and comparing interview answers with the notes from the medical chart and the observed discharge conversations. For each of the five information domains, knowledge retention was rated on a 4-point scale: (1) full, (2) partial, (3) minimal or (4) none. Data were considered ‘not available’ if discharge information was not provided to the participant. Second, interviewees were asked to rate their satisfaction with the ED discharge process on a range from 1 (‘very dissatisfied’) to 10 (‘very satisfied’) and to explain their satisfaction score. Interviewees who received teach-back were also asked if and why (not) they were annoyed by this method of repeating instructions. Finally, we assumed that teach-back could have a positive effect on activating and improving self-management by older patients. Therefore, interviewees were asked to rate four statements from a validated Dutch version of the Patient Activation Measure (PAM), which assesses a person’s beliefs about, confidence in and knowledge and skills for managing health-related care tasks.33 34 The research team selected four relevant statements from the PAM to minimise response fatigue.
Supplemental material
Supplemental material
Data analysis
We used descriptive statistics to summarise the baseline characteristics and outcomes of the preintervention and postintervention groups. Characteristics and outcomes were summarised using means (with a SD) and medians (with an IQR) for continuous variables, depending on the normality of distribution. Frequencies and percentages were used for categorical variables. Cohen’s kappa scores were calculated to determine the interrater agreement on knowledge retention. Scores on knowledge retention for each information domain were plotted over time (ie, date of the interview) to see whether there was not already a secular trend in improved retention prior to the teach-back intervention. To facilitate modelling, scores on ED discharge time were dichotomised into outside and during peak hours (noon to 6 pm). MTS urgency level scores were dichotomised into high (MTS category ‘immediate’ and ‘very urgent’) and low (MTS category ‘urgent’ and ‘standard’ and ‘nonurgent’).35 Knowledge retention scores were dichotomised into: ‘full retention’ and ‘partial, minimal or no retention’. Scores on the self-reliance statements were dichotomised into ‘(strongly) agree’ and ‘(strongly) disagree’. We used Pearson’s χ2 test for the comparison of dichotomous data and the unpaired t-test for continuous data. Nonnormally distributed data were compared by a Mann-Whitney U test after determining the normality of the data by the Kolmogorov-Smirnov test and the assessment of skewness and kurtosis. Univariable and multivariable logistic regression analyses were then performed to yield ORs and adjusted odds ratios (AORs) with 95% CIs. Covariates adjusted for in the multivariable models were age, sex, urgency triage level, ED LOS, ED discharge during peak time, comorbidity level and cognitive impairment. The Hosmer-Lemeshow goodness-of-fit test was applied to evaluate the model fit. Statistical significance was set at p≤0.05. Analyses were conducted using SPSS StatisticsV.23.0. Finally, interview audio recordings were analysed by one researcher to explore participants’ experiences with teach-back. Illustrative quotes were selected and transcribed.
Results
Description of the study sample
Throughout the study period, 13 388 visits were registered at the ED and these cases were assessed for eligibility. In total, 648 patients were eligible to participate and consented, with 343 (52.9%) who received standard discharge care and 305 (47.1%) who received teach-back at discharge (figure 1). The baseline characteristics of the preintervention and postintervention groups are shown in table 1. No statistically significant differences were observed for age, sex, urgency triage level, comorbidity level, polypharmacy, duration of discharge instructions or ED discharge during busy hours. However, patients in the standard discharge group stayed significantly longer in the ED (median of 143 vs 131 min; p=0.03).
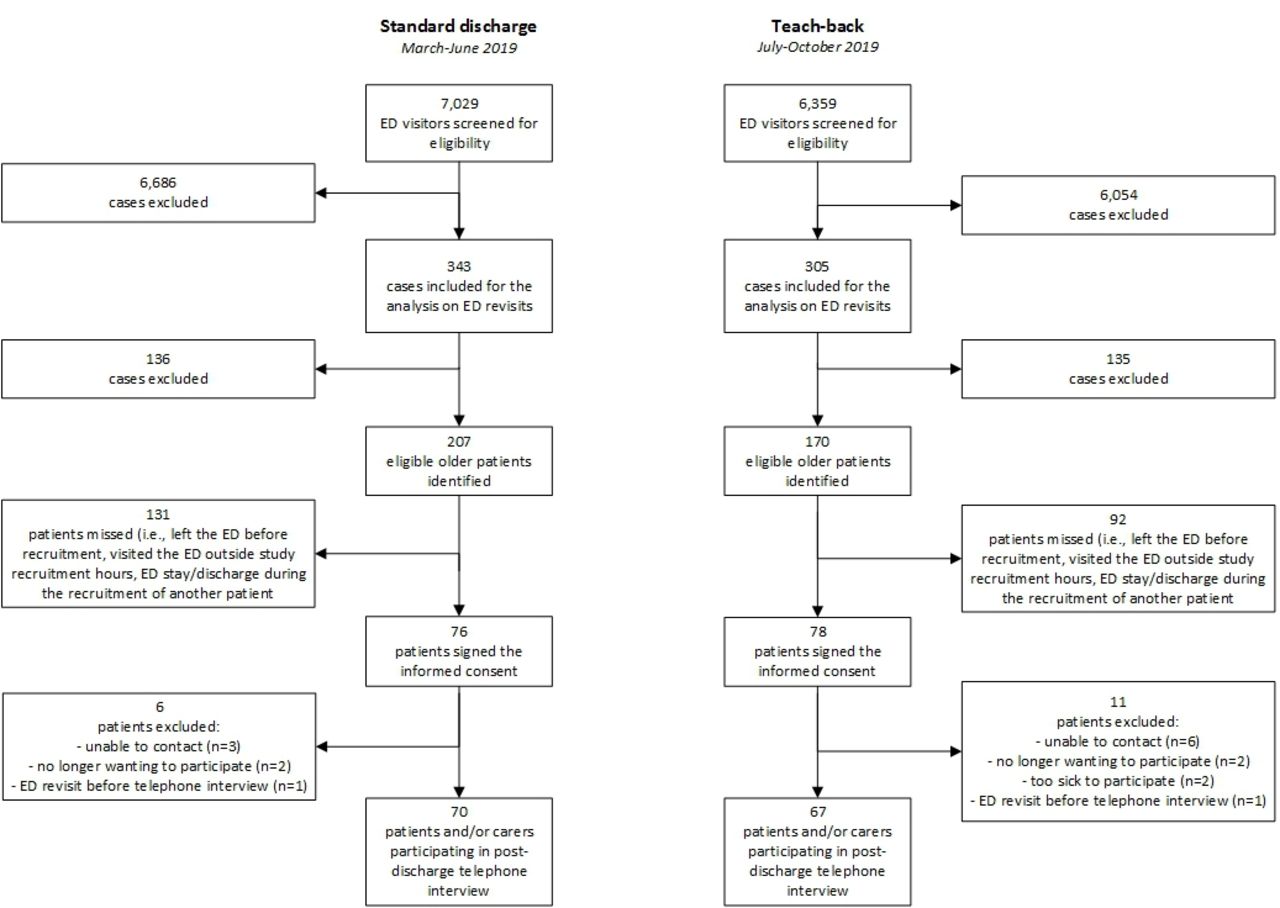
Flow diagram of the study selection process. ED, emergency department.
Baseline comparison of study samples receiving standard discharge care and teach-back
Of the 648 eligible participants, 377 were older adults (figure 1). Two hundred and twenty-three cases were not recruited for secondary analyses due to various reasons. Seventeen older adults were lost to follow-up, resulting in 70 (51.1%) in the standard discharge group and 67 (48.9%) in the teach-back group. No significant baseline differences were found between the groups except for older adults having a higher CCI in the standard discharge group and more older adults with cognitive impairment at the time of ED discharge in the teach-back group (table 1). Discharge conversations lasted longer for participants receiving standard discharge care than for those receiving teach-back, with medians of 7 min (IQR, 5–10) and 5 min (IQR, 3–9), respectively.
ED revisits
We observed pre–post differences in ED revisits within 7 days and within 8–30 days postindex visit (table 2). Participants receiving teach-back had a reduced likelihood of an ED revisit within 7 days and within 8–30 days compared with participants receiving standard discharge care. These associations were not statistically significant after controlling for age, sex, urgency triage level, comorbidity level, ED LOS and ED discharge during peak time.
Associations between the use of teach-back (vs standard discharge care) and ED return visits
Knowledge retention of older adults
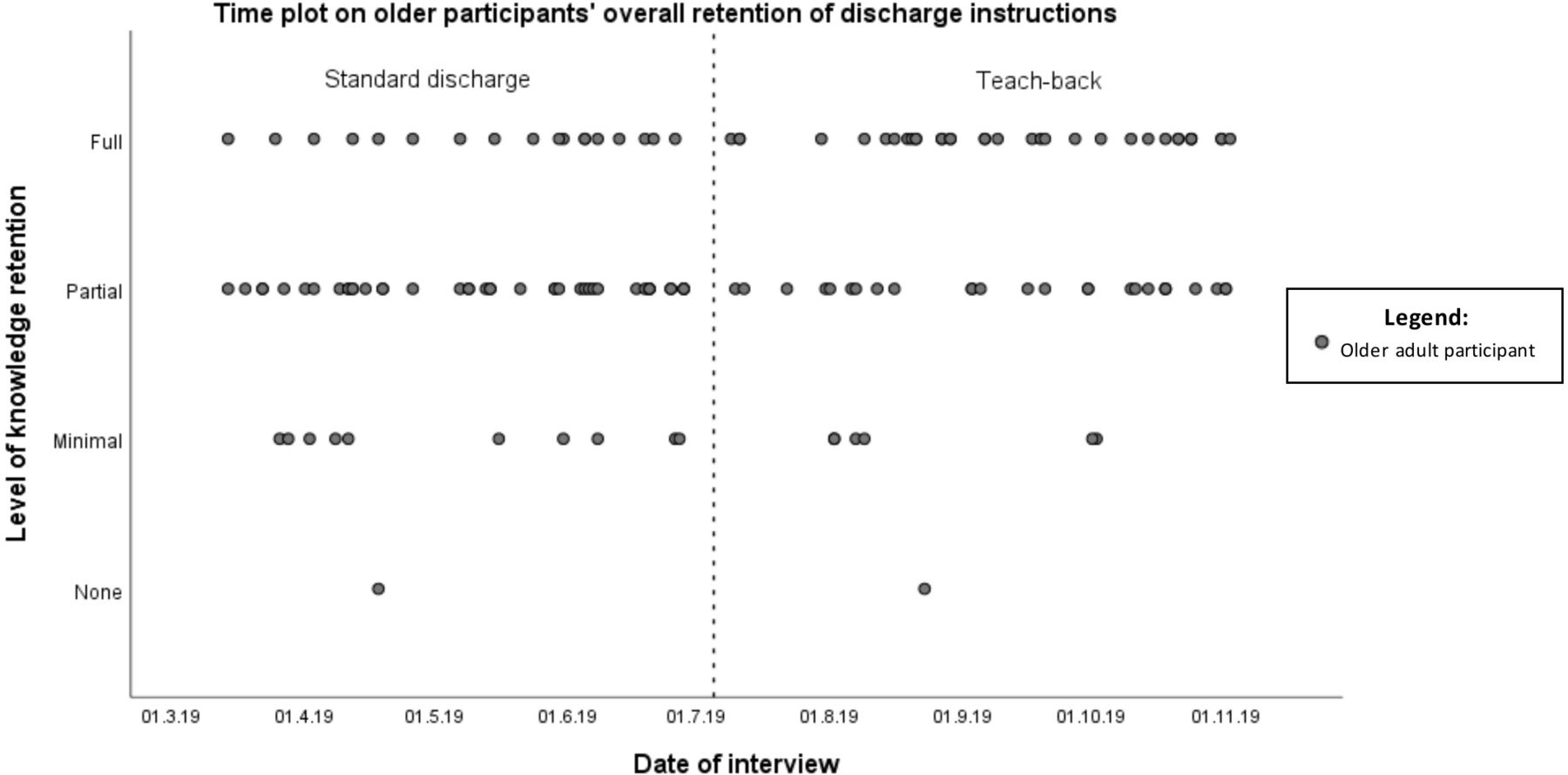
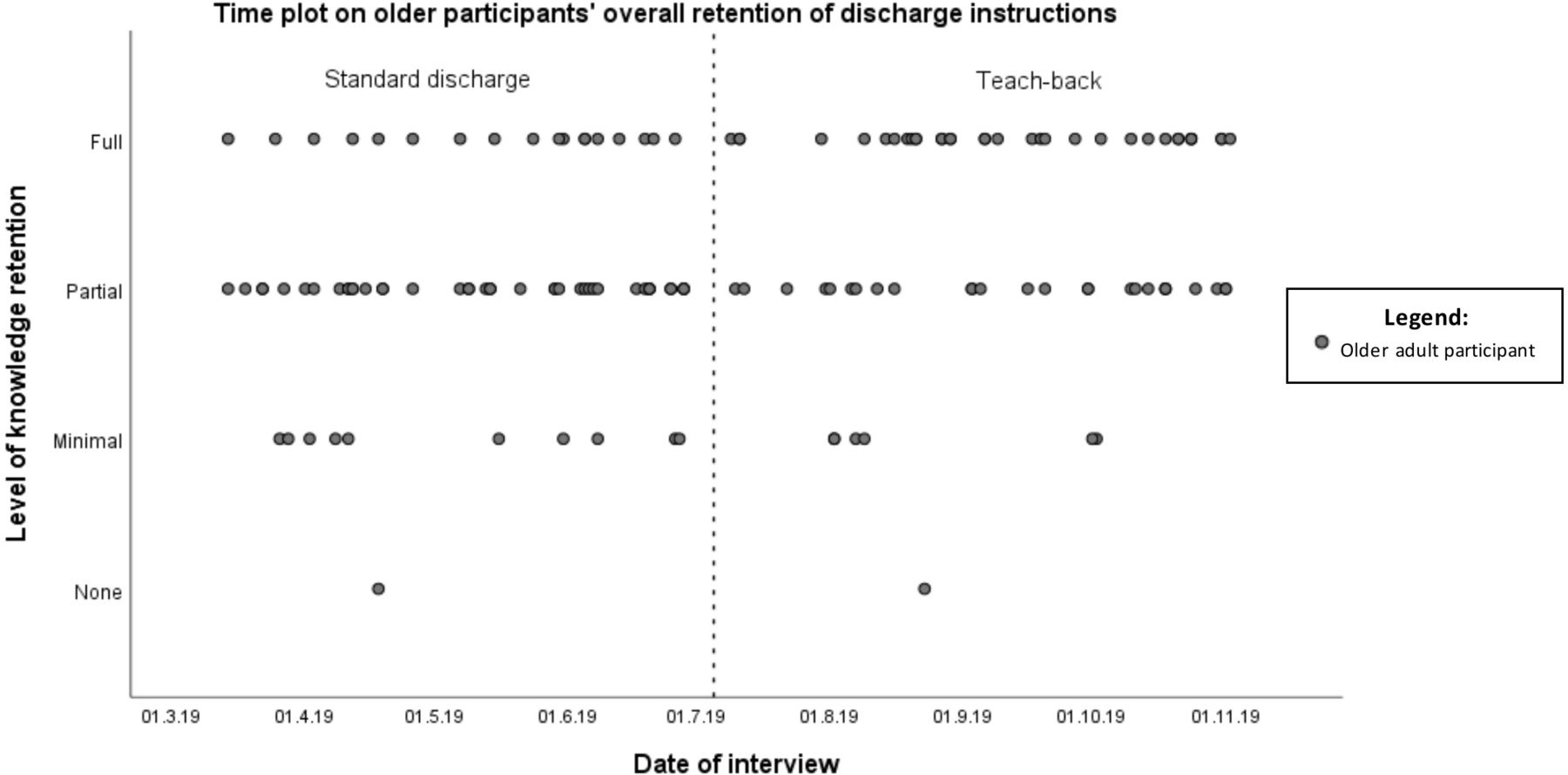
Interrater agreement of knowledge retention on the five domains varied between 0.7 (ie, instructions on ED diagnosis and treatment) and 0.9 (ie, instructions on return precautions). Time plots and histograms do not show clear secular trends in improved retention prior to the use of teach-back (figure 2; online supplemental file 5). Deficits in knowledge retention were noted between the study groups in each information domain (table 3). Almost one-third of the participants receiving standard discharge care showed partial to no retention on each of the five information domains. Full knowledge retention of the instructions was numerically higher in all five information domains for participants receiving teach-back. After controlling for comorbidity level and cognitive impairment at the time of ED discharge, participants receiving teach-back had a higher likelihood of full retention of information regarding the diagnosis and treatment at the ED (AOR 2.19; 95% CI 1.01 to 4.75; p=0.048), medication (AOR:14.89; 95% CI 4.12 to 53.85; p<0.001) and follow-up appointments (AOR: 3.68; 95% CI 1.33 to 10.19; p=0.012).
Supplemental material
{kind=link}
{kind=link}
Time plot on older participants’ overall retention of discharge instructions.
Associations between the use of teach-back (vs standard discharge care) and retention of discharge instructions by older participants per information domain
Perceived self-management and satisfaction with discharge instructions of older adults
No significant group differences were observed on items related to perceived self-management postdischarge, except for one item (table 4). Participants who received teach-back appear to be more confident in determining when they needed to receive medical care (and when to handle a health problem themselves). However, we were unable to detect a reliable association between this aspect of self-management and the use of teach-back at ED discharge (OR 13.24; 95% CI 1.67 to 105.01; p=0.014).
Associations between the use of teach-back (vs standard discharge care) and perceived self-management by older participants at home
Satisfaction with discharge instructions was high in both study groups with mean scores of 8.5 (SD 1.2) and 8.7 (SD 0.9) in the standard discharge group and the teach-back group, respectively. No significant score differences between the two groups were found (p=0.41). Of the 67 interviewed participants receiving teach-back, 65 (97%) did not address negative feelings about repeating the discharge instructions. Teach-back was considered by many of them to be a logical element in the discharge process and was perceived as a useful educational tool to learn key information needed to continue care after discharge. For example, one patient expressed, ‘It [teach-back] is a very useful check to see if I understood it (discharge instructions) correctly’. According to participants, teach-back also helped them leave the ED more self-assured about performing self-care tasks. One patient illustrated this by saying, ‘This confirmation made me more confident to go home and take care of myself’.
Discussion
This study evaluated the effects of teach-back at ED discharge on ED revisits and on outcomes for older patients. Although no significant associations were found between the use of teach-back and a reduction in short-term ED revisits, the pre–post differences in ED revisits indicate that teach-back may be a useful strategy to reduce potentially unnecessary use of medical services.30–32 36 37 The results of this pilot study also suggest that the use of teach-back has positive effects on older patient outcomes. We found associations between the use of teach-back and better short-term knowledge retention of discharge instructions by older patients, regardless of their clinical and cognitive condition. Improved knowledge retention was particularly found in the domains where recall deficits and incomprehension of instructions most frequently occur,6 38 39 namely, instructions related to prescribed medication and follow-up appointments. Better knowledge retention of instructions in these domains could reduce postdischarge noncompliance,12 14 adverse drug events,40 41 deterioration of health10 15 16 and the use of health services.10 15 16 The relatively large proportion of older patients with partial to no retention of instructions provided at the ED is in line with previous studies,6–10 37 38 and shows once again that further effort is needed to improve patient understanding and retention of instructions provided during an ED visit. We found no strong evidence for teach-back as a supportive method for improving the overall activation of self-management of health and healthcare postdischarge. A positive, although not very reliable, association was found between teach-back at ED discharge and a higher confidence among older patients to determine when to seek medical care (and when to handle a health problem themselves). With this improved level of activation, patients may be able to make better decisions affecting their health42 43 and are less likely to be in need of emergency care and hospitalisation.44 45
Our findings support previous literature reporting satisfaction with teach-back by patients and carers.23 46 Although satisfaction was already high in both study groups and the between-group differences were small, participants seemed more satisfied with the discharge conversation after receiving teach-back; the vast majority described teach-back as a self-evident and useful tool to help confirm learning and to avoid forgetting key information. This finding contradicts concerns by both patients and professionals that teach-back might be perceived as a patronising or condescending way of determining if information is understood.46 47 Contrary to previous studies questioning the feasibility of teach-back in the ED setting,48 49 our study did not show an extension of discharge time as a result of teach-back. Interestingly, discharge conversations with teach-back were generally shorter than ‘standard’ discharge conversations. This suggests that teach-back may contribute to more efficient care in a setting where professionals often need to work under time constraints.
Our study had several limitations. First, we conducted a pre–post design without randomisation. Although causation cannot be determined in this type of study design,50 there were no major policy changes in the delivery of care or other healthcare quality improvement initiatives in the ED during our study period that could have confounded the findings. Also, the created time plots and histograms illustrate that retention of discharge instructions was not already changing in the desired direction prior to the implementation of teach-back and suggest that found effects were most likely related to the use of teach-back rather than a general ongoing trend over time. Second, the study was performed in a single ED site. The findings may, therefore, not be generalisable to other sites. Third, the relatively small sample of older participants limits the precision of the associations on knowledge retention and self-management. Although this was a limiting factor, we deliberately chose to use the available research time and capacity to ensure provider compliance with teach-back, perform a reliable pre–post analysis of outcomes and provide an accurate determination of knowledge retention of discharge instructions provided at ED discharge. Fourth, data were collected by two investigators who were not blinded to the phase of the study. This may have introduced interinvestigator variation and bias in the collection of interview data and in the assessment of knowledge retention. However, we tried to control for these aspects by using a standardised interview protocol and scoring system. In addition, interrater agreement of knowledge retention was tested and the tests showed acceptable kappa scores. Fifth, participants may have been aware of a change in the discharge process. Self-reported findings on satisfaction and self-management may have been biased by the Hawthorne effect. Sixth, some selection bias may have occurred because of patient unavailability at the time of the phone interview. We tried to control for this by calling back unavailable participants multiple times and by varying call-back times. Participants were also only recruited during office hours. Potentially confounding factors (eg, perceived work pressure by ED professionals) related to the discharge of patients out-of-hours may have been overlooked. Moreover, non-Dutch-speaking patients were excluded because of translation issues while this group would perhaps benefit the most from teach-back although via an interpreter. Seventh, we were not able to determine whether the pre–post differences in observed ED return visits were caused by better knowledge retention or self-management resulting from teach-back at discharge. Other external factors (eg, exacerbations) may have led to an inevitable ED revisit. Therefore, our findings need to be interpreted with caution. Finally, other confounding factors not adjusted for in the multivariable analysis could be another limitation. The bias that may be introduced by all of these factors requires a more rigid methodology, for which we think that a multicentre stepped wedge design would be ideal. Future studies should also adjust for health literacy level, as previous literature has shown that low literacy patients in particular might benefit from teach-back.11 51
In summary, this pilot study shows that teach-back is a feasible method that supports professionals in the ED in discharge communication with patients and carers and can contribute to safer and better transitional care from the ED to home. Managers, professionals and educators, therefore, need to consider implementing teach-back as a standard element of the discharge process in the ED. The integration of teach-back into routine discharge practice can be stimulated by the use of a variety of available educational resources and implementation guides.52–54 The positive results of our pilot warrant further investigation in a larger clinical trial to provide more evidence for structural implementation of teach-back in the ED, as it can be a feasible and valuable intervention to reduce the risks at discharge from EDs.
Data availability statement
Data are available upon reasonable request. The original quantitative SPSS datasets generated during and/or analysed during the study are available upon reasonable request from the corresponding author. Datasets will contain individual deidentified data of participants who gave written consent.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank all patients and carers for their participation in this study. The authors would also like to thank Reinier Akkermans for his assistance with the statistical analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
GH and ÖS are joint first authors.
Handling editor Mary Dawood
Author contributions GH, OS and YS conceived and designed the study, obtained research funding, and supervised the conduct of the study. NK and CT were responsible for data collection. NK, CT and OS were responsible for the implementation of the intervention. GH and OS analysed and interpreted the data. GH and OS drafted the manuscript, which was critically revised for important intellectual content by YS, NK, CT, MM and MOR. GH and OS share their first authorship and take responsibility for the paper as a whole.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.