Article Text

Abstract
Objective To determine the relative importance members of the US public place on different patient attributes in triage decisions about who should receive the last available intensive care unit (ICU) bed.
Methods A discrete choice experiment was conducted with a nationally representative sample of 2000 respondents from the YouGov internet panel of US households. Respondents chose which of three hypothetical patients with COVID-19 should receive an ICU bed if only one were available. The three patients differed in age, gender, Alzheimer’s-like disability and probability of survival if the patient received the ICU bed. An experimental design varied the values of the four attributes of the three hypothetical patients with COVID-19 that a respondent saw in four choice tasks.
Results The most important patient attribute to respondents was the probability the patient survives COVID-19 if they get the ICU bed (OR CI: 4.41 to 6.91). There was heterogeneity among different age groups of respondents about how much age of the patient mattered. Respondents under 30 years of age were more likely to choose young patients and old patients, and less likely to select patients aged 40–60 years old. For respondents in the age group 30–49 years old, as the age of the patient declined, their preference for saving the patient declined modestly in a linear fashion.
Conclusions Respondents favoured giving the last ICU bed available to the patient with the highest probability of surviving COVID-19. Public opinion suggests a simple guideline for physician choices based on likelihood of survival as opposed to the number of life-years saved. There was heterogeneity among respondents of different age groups for allocating the last ICU bed, as well as to the importance of the patient having an Alzheimer’s-like disability (where religion of the respondent is important) and the gender of the patient (where the gender and racial identity are important).
- COVID-19
- triage
Data availability statement
Data are available upon reasonable request. Data are available from the authors upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this subject
Current guidance on triage choices is largely focused on the ethical principles that should be used, with some consideration to what is practical in an emergency situation in which health professionals have little time to deliberate.
What this study adds
The US public do not support triage policies that would put less weight on saving the lives of older adults.
Physicians in emergency settings such as the COVID-19 pandemic can make rapid judgements based on a simple heuristic of ‘what patient has the highest probability to survive if they get the ICU bed,’ without having to consider a host of other ethical considerations.
Introduction
The COVID-19 pandemic has forced doctors in many locations around the world to face the difficult triage question of who should get the last intensive care unit (ICU) bed when the demand for facilities exceeds supply. The question of how to allocate scarce health resources has been discussed in the literature, for natural disasters and healthcare emergencies,1–4 and specifically for COVID-19.5–9 This literature on triage choices is largely focused on the ethical principles that should be used, with some consideration to what is practical in an emergency situation in which health professionals have little time to deliberate. For example, Emanuel et al 5 put forth a number of recommendations for triage choices. Among these, they advise physicians to concentrate on the number of lives saved, but also propose the alternative metric of the number of life-years saved (recommendation 1). But they also note: ‘Limited time and information in a COVID-19 pandemic … counsel against incorporating patients’ future quality of life, and quality-adjusted life-years, into benefit maximization.’
In addition to the limited time available for decision-making, what distinguishes triage decisions in the COVID-19 pandemic is the fact that the probability of death due to COVID-19 is much higher among elderly patients.10 However, age is not perfectly correlated with survival probability11; pre-existing health conditions and disabilities are also associated with higher mortality risk.12 At least one US political leader has indicated a willingness to sacrifice elderly patients and those with Alzheimer’s in order to open up the economy and prevent business losses.13 Although this argument is in opposition to the ethical recommendations put forward by health and other experts, it continues to receive considerable national and international attention and public support.14
We wished to determine how the American public would like such triage decisions to be made, that is, what choices would members of the American public make if they were put in the shoes of an ED physician who is forced to choose which patient with COVID-19 should get the last available ICU bed. Such evidence on public opinion is important for two reasons. First, a public health policy that aligns with the public’s preferences is likely to face less resistance and be easier to implement. Knowing whether any particular plan is congruent or divergent from the public’s view is critical information for developing communication strategies that effectively convey the rationale for the policy adopted and in understanding objections that might be raised. Second, a public health policy on how to manage ICU triage that has the support of the public has more claim to legitimacy than a policy designed solely by experts.
In a large nationally representative survey, we asked respondents to choose which of three hypothetical patients with COVID-19 should receive an ICU bed if only one bed was available. The analysis of these survey data enables us to determine if the US public’s preferences are consistent with Emanuel et al’s main triage recommendation.
Methods
We used a discrete choice experiment15 to analyse the data collected from 2000 respondents from the YouGov internet panel of US households. In the survey research community, a sample size of 500 respondents is considered adequate to represent the views on the US population on standard survey questions (eg, a sample size of 500 translates into a 95% CI of ±4.3% for a true split of 50/50 in the population on a favour/oppose type question). A random sample of 2000 Americans is considerably larger than used in most academic and policy relevant studies, and ensured that our sample would not be underpowered.
YouGov maintains an online panel of several million respondents who answer their clients’ surveys. For our survey, YouGov drew a random sample of their respondents that matched the demographic characteristics of the US population. The sample of 2000 respondents from the YouGov panel used in this study closely matches the 2019 census population averages for key socioeconomic and demographic characteristics (see online supplemental table S1).
Supplemental material
Respondents were interviewed between 28 August and 4 September 2020. The questionnaire provided respondents with a simple explanation of what survival probability means and then presented respondents with four ‘choice tasks’ in which they had to choose which of three hypothetical patients with COVID-19 (based on combination of attributes) should receive an ICU bed if only one bed was available. The ICU bed is described as having both oxygen and ventilator available. Respondents were told that all three patients were ‘almost certain’ to die without an ICU bed. The three patients differed in four ways: (a) age, (b) gender, (c) the presence or absence of an Alzheimer’s-like disability and (d) the patient’s probability of survival if they received the ICU bed. The sampling methodology and survey administration are described in the online supplemental materials (see S1 YouGov Sampling Methodology and S2 IRB Approval and Survey Administration).
Age was the key patient attribute used to distinguish a respondent’s preferences between saving a patient’s life now and saving a patient with the most life-years remaining. We included the patient’s gender and mental disability because our pretest results suggested that these attributes were important for some respondents. In order to clearly distinguish the mental disability attribute from the probability of survival, we described it as ‘Alzheimer’s or a similar mental disability that makes it impossible for the person regardless of their age to take care of themselves.’
Table 1 presents an example of the table respondents saw for one of the four choice tasks they received. The values of the four attributes for patients A and B were randomly assigned using an experimental design described in the online supplemental materials (see S3 Experimental Design). For age, the levels are 20, 40, 60 and 80 years old. For gender, female and male; and for having an Alzheimer’s-like mental disability, the two levels are yes and no. For survival probability, the levels are 20%, 40%, 60% and 80%. The values for the four attributes for patient C were fixed and the same for all four choice tasks and for all respondents (50 years old, female, not having an Alzheimer’s-like mental disability and having a survival probability of 50% if they received the ICU bed) (see S4 for data results that show the effectiveness of the randomisation process).
Example of respondent choice task
The four discrete choice tasks that each respondent answered can be conceptualised as a generalisation of a simple dose–response experiment in which there are only two patients and the patient characteristics are identical except for one variable such as survival probability. In a simple dose–response experiment, this single variable is randomly varied for patient B and the response (picking patient B or not) is observed. Our experimental design allows multiple characteristics to be simultaneously varied and the use of three rather than two hypothetical patients and four choice sets greatly increases statistical power. The decisions respondents make reveal their trade-offs between the attributes of the patients.
Based on random utility theory,15 16 we used a conditional logit model to explain the choices that respondents made regarding which of the three hypothetical patients should receive the remaining ICU bed (see S5 Random Utility Models in the online supplemental materials). Including the option of patient C (whose attribute levels were fixed) in the respondents’ choice sets ensured statistical identification (because it allowed a common comparison) and increased statistical efficiency in the centre of the ranges of values that respondents saw for the attributes age and survival probability. If most respondents tend to pick the youngest patient for the ICU bed, the coefficient on age would be negative (as the age of a patient increases, the probability of choosing that patient declines). If most respondents tend to avoid giving the ICU bed to the patient with an Alzheimer’s-like mental disability, the coefficient on that variable would be negative (because the probability of choosing a patient with a mental disability is less than of choosing a patient without a mental disability). Since we are using a logit model, the parameters can easily be expressed in OR form.
Patient and public involvement
Neither the respondents nor the public were involved in the development of the research questions or outcome measures, nor informed by their priorities, experience, and preferences. However, the objective of the research was to determine respondents’ preferences and priorities. No patients were involved in this study.
Results
The model results presented in table 2 show that the most important patient attribute (OR CI: 4.41 to 6.91) in determining which of the three hypothetical patients most respondents chose to receive the last ICU bed is the probability the patient survives COVID-19 if they get the ICU bed.
Conditional logit model results
The results in table 2 also show that on average our respondents have a slight preference for female patients receiving the ICU bed (OR CI: 1.16 to 1.28) and against patients with an Alzheimer’s-like mental disability (OR CI: 0.74 to 0.83). The average respondent would be indifferent between allocating the remaining ICU bed to a male patient and a female patient with 10% smaller survival probability than the male patient. The average respondent would be indifferent between allocating the remaining ICU bed to a patient without a mental disability and a patient with an Alzheimer’s-like mental disability and a 14% higher survival probability than the patient without an Alzheimer’s-like mental disability. Respondents do not favour giving the last ICU bed to younger patients (ie, they do not prioritise saving the most life-years); indeed, the OR of the age attribute is greater not less than one (OR CI: 1.000 to 1.004). The ORs for how the four patient attributes affect respondents’ choices are shown in figure 1.

ORs for patient attributes: results from conditional logit model.
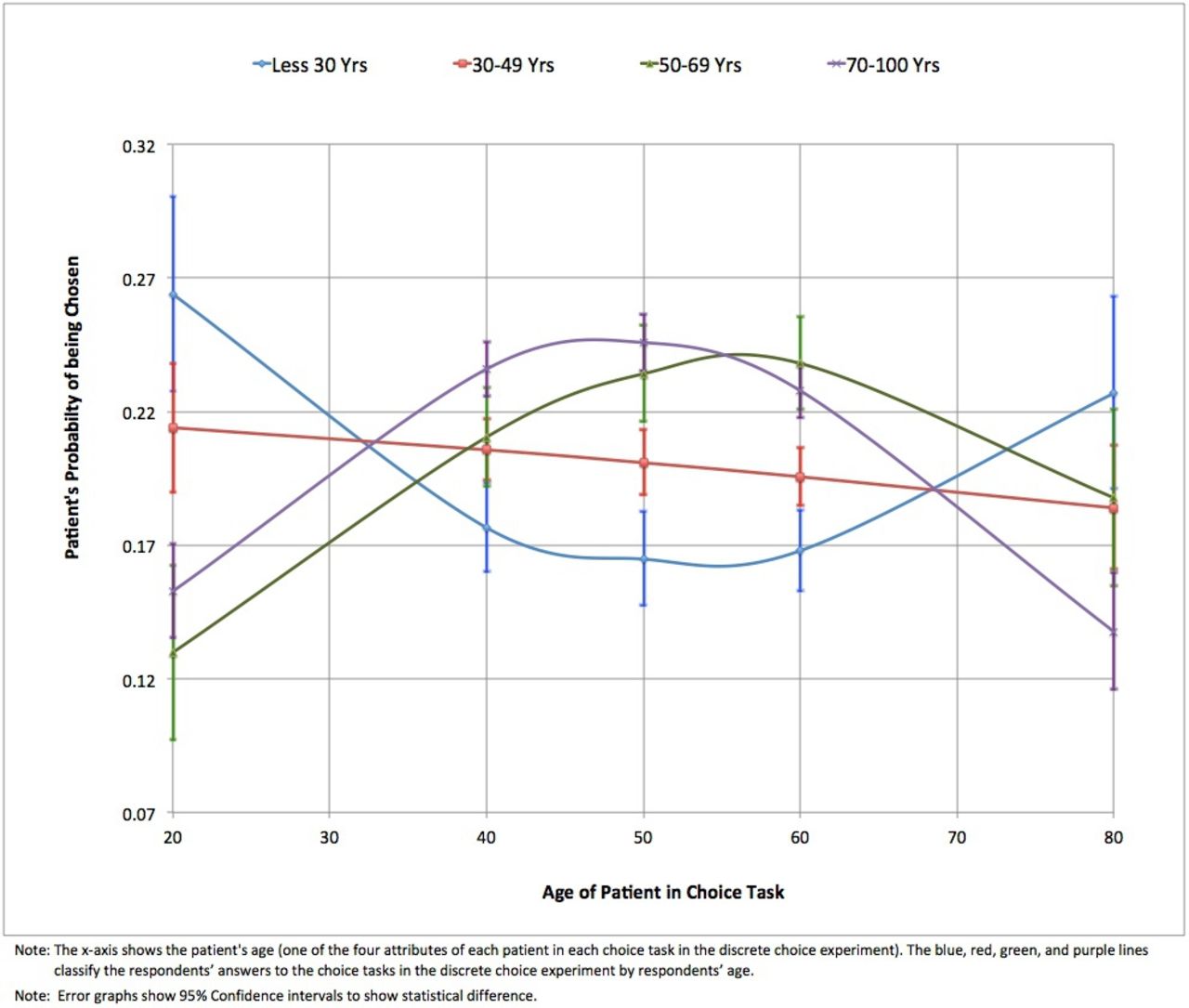
Our results summarize on average the opinions of members of the US public about who should receive the scarce ICU bed, but mask considerable underlying preference heterogeneity. Figure 2 shows how the age of the patient affects the probability that the patient is chosen to receive the remaining ICU bed for four different age groups of respondents (<30 years, 30–49 years, 50–69 years, >70 years). The age variable on the x-axis in figure 2 shows the attribute of the patient that respondents saw in the choice experiment. The age groups in figure 2 represented by the blue, red, green and purple lines classify the respondents’ answers to the choice experiment by the respondent’s age. Respondents under 30 years of age were more likely (other things equal) to choose young patients and old patients, and less likely to select patients aged 40–60 years old. The preferences of respondents in the age group 30–49 years old were different; their choices revealed that as the age of the patient declined, their preference for saving the patient declined modestly in a linear fashion. The choices made by respondents in the two oldest age groups (50–69 years old and >70 years old) revealed that they had very different preferences from both the youngest age group (<30 years old) and the middle-age group 30–49 years old. The two older age groups (50–69 and >70 years old) preferred to allocate the ICU bed to patients in the age groups 30–49 and 50–69 years old, not to the young or the old.
{kind=link}
{kind=link}
Probability of choosing a patient as a function of the patient’s age (for four different age groups of respondents).
The error bars in figure 2 show 95% CIs for the estimates of respondents’ preferences for patient age by age of respondent. Respondents’ preferences over patients’ age (when holding all the other attributes constant) are not statistically different for each level of the attribute of patient’s age for respondents less than 30 and between 30 and 49 years, or between the groups of 50–69 years and more than 70 years. However, the preferences of respondents less than 50 years are statistically different from respondents over 50 years of age. These differences are also more pronounced when comparing preferences over young patients and middle-aged patients.
These heterogeneous preferences were also shown for race: African Americans and Hispanics put less weight on survival probabilities than white respondents (OR CI: 0.201 to 0.481, p=0.000). White respondents, especially those who are retired, are less likely to give the ICU bed to a patient with an Alzheimer’s-like disability (OR CI: 0.556 to 0.712, p=0.000) (see online supplemental table S7).
Discussion
Health economists have long advocated for evaluating health outcomes in terms of the value of life-years saved, thus putting more weight on saving younger individuals.17 18 At the beginning of the COVID-19 epidemic, the lieutenant governor of Texas, Dan Patrick, said that grandparents were willing to sacrifice themselves in order to keep the economy from shutting down.13 Our study suggests that the US public do not support triage policies that would put less weight on saving the lives of older adults.
The setting for our study is a hospital facing a spike in critically ill patients with COVID-19. We asked a national representative sample of the American public what types of patients should receive priority for a limited supply of ICU beds. Their answers reveal what they would like physicians to do in such a triage situation. Our results suggest that physicians in emergency settings such as the COVID-19 pandemic can make rapid judgements based on a simple heuristic of ‘what patient has the highest probability to survive if they get the ICU bed,’ without having to consider a host of other ethical considerations. In other words, the public preferences captured through our choice experiment and modelled with a conditional logit model support Emanuel et al’s5 recommendation that physicians should focus on maximising lives saved (the survival probability attribute in our discrete choice experiment), but not worry about saving the most life-years. From our perspective, the much smaller magnitude of the effects of age, gender and mental disability suggests these attributes are not relevant to practical triage policy.
Grover et al 19 have also recently evaluated public preferences for scarce medical resources in the context of the current COVID-19 pandemic using a method that ranks eight ethical positions with respect to the allocation of scarce resources. They found the highest rank for ‘saving the most lives,’ followed by ‘sickest first’, and then in a third and less preferred place for ‘youngest first’. However, their ranking method does not enable them to identify the trade-offs respondents would make between patient attributes, which our approach does by asking survey respondents to make an explicit choice between patients with different attributes.
Our results do indicate that respondents’ preferences are complex and heterogeneous, especially with respect to the priority given by different respondents to the age of the patient. This complex age effect is largely driven by middle-aged respondents exhibiting a stronger preference for saving middle-aged patients. All the casual talk by some political commentators that old folks in nursing homes, who are at high risk of COVID-19 infection and mortality, are a drain on the economy, and should be jettisoned first, is inconsistent with what the majority of the American public want. Further, our respondents had little proclivity to sacrifice someone with an Alzheimer’s-like mental disability if their probability of survival is noticeably higher than another patient who needs the scarce ICU bed. We expect that even this modest adverse selection factor would be considerably smaller for the vast majority of other disabilities a physician might encounter in a triage situation.
In summary, in an overwhelmed hospital situation, the US public favour a simple triage decision rule: if physicians have to choose how to allocate a scarce ICU hospital bed, pick the patient with the best chance of making it. Of course, following public preferences is not the only way to determine who should receive an ICU bed. Clearly, healthcare professionals may have different opinions, given their experience. Policies based on public preferences are not a priori the optimal approach to select patients for an ICU bed. However, whether public preferences are convergent or divergent from those of healthcare professionals, knowledge of them should be useful in developing effective communication strategies by doctors and hospitals. We make no claim that these findings would apply in countries outside the USA.
Limitations
In most surveys in which respondents are asked to make decisions that relate to risks that change survival probabilities, the changes in survival probabilities are quite small and can be hard for many individuals to understand. Also, respondents are often presented with choice situations that are hard to understand and have little policy relevance. Our situation is quite different. Our respondents are asked questions about changes in survival probabilities that were large; where the choice context was easily understandable due to media reports on the COVID-19 pandemic; and where the relevance of public input to the policy process was clear.
Nevertheless, there are three main limitations of our study. First, like the vast majority of doctors, our respondents have never been put in a situation where they would actually need to make choices similar to those posed in the survey. Thus, they have no prior experience making this type of decision. If a sample of participants with prior experience was desired, one would need to turn to medical personnel with experience in active war or disaster zones. As noted in the introduction, our research findings should not be seen as a substitute for informed medical judgement but rather as an input to a broader process for drafting guidance for handling triage decisions in epidemics or large-scale disasters where the choices might be similar to the situation we described to respondents.
Second, we provided our respondents with a relatively short list of patient attributes: age, gender, major disability and survival probabilities. We could have presented respondents with choices in which the hypothetical patients had more attributes. For instance, other attributes might be the nature of the medical problems that the patient faces after time spent in the ICU. Additional patient attributes could be added to our existing survey instrument, but we think researchers should be careful not to add attributes that concern problems about which people expect doctors to make expert judgements.
Third, our research only looks at the COVID-19 context. While a reasonable assumption would be that that our work is applicable to other contexts, such as earthquakes, tropical cyclones or pandemics that involved diseases with characteristics substantively different than that of a respiratory virus, it would be useful to establish this with empirical work.
Abstract translation
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.Data availability statement
Data are available upon reasonable request. Data are available from the authors upon request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The Institutional Review Board of Arizona State University determined that the protocol for this research (IRB ID: STUDY00011907) is considered exempt pursuant to Federal Regulations 45CFR46 on May 4, 2020. Participants gave informed consent to participate in the study before taking part.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Richard Body
Correction notice This article has been corrected since it was first published. The open access licence has been updated to CC BY.
Contributors MH, RTC and DW conceptualised the research and designed the survey instrument. JJL and RTC prepared the experimental design. RTC and HCC conducted the data analysis. All authors participated in the interpretation of the results and drafting the manuscript. DW is the guarantor of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.