Article Text

Abstract
Background Guidelines for adults presenting to the emergency department (ED) with suspected sepsis recommend protocols and bundles that promote rapid and potentially intensive treatment, but give little consideration of how patient characteristics, such as age, functional status and comorbidities, might influence management. This study aimed to describe the characteristics, management and outcomes of adults attending the ED with suspected sepsis, and specifically describe the prevalence of comorbidities, functional impairment and escalations of care.
Methods We undertook a single-centre retrospective observational study involving medical record review of a random sample of adults admitted to an ED between February 2018 and January 2019 with suspected sepsis. Descriptive statistics were used with 95% confidence intervals (CIs) for key proportions.
Results We included 509 patients (median age 74 years), of whom 49.3% met the Sepsis-3 criteria. Less than half of the patients were living at home independently (42.5%) or could walk independently (41.5%), 19.3% were care home residents and 89.2% of patients had one or more comorbidity. 22% had a pre-existing do not attempt resuscitation order. 6.5% were referred to intensive care, and 34.3% of the 13.2% who died in-hospital had an escalation plan explicitly documented.
Conclusion Adults with suspected sepsis have substantial functional limitations, comorbidities and treatment directives that should be considered in guidelines, especially recommendations for escalation of care.
- emergency department
- infection
- intensive care
- clincial management
- resuscitation
- clinical care
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Statistics from Altmetric.com
Key messages
What is already known on this subject
Guidelines for suspected sepsis recommend rapid and potentially invasive treatment focused on saving lives.
There has been limited research investigating when these treatments may not be appropriate or epidemiological studies describing the cohort of patients with suspected sepsis.
Adults attending the emergency department often have functional limitations and comorbidities that, if reflected in people with suspected sepsis, may limit the potential benefit of intensive treatment.
What this study adds
This retrospective, single-centre study has demonstrated that patients with suspected sepsis are typically elderly, less than half are living at home independently or can walk independently, almost one-fifth are care home residents, and few have no comorbidities.
Guidelines for suspected sepsis should include these characteristics in management recommendations, especially treatment escalation decisions.
Introduction
Sepsis is a life-threatening dysregulated response to infection that can lead to organ dysfunction, causing 52 000 deaths annually in the UK.1 Diagnosing sepsis is difficult, as reflected in the evolution of its definition. The latest definition, ‘Sepsis-3’, combines the presence of infection with the Sequential Organ Failure Assessment (SOFA) score. The latter requires a change from baseline SOFA score of 2 or more to represent organ dysfunction, and the assumption that the baseline score is zero unless the patient is known to have pre-existing organ dysfunction before the onset of infection.1 The quick SOFA (qSOFA) was developed for recognising those at a greater risk of poor outcome outside of the intensive care unit (ICU) (see online supplemental material).1 2
Supplemental material
The number of patients presenting to emergency departments (ED) is increasing and we have an ageing population; between 2003 and 2015, the number of people aged over 85 years presenting to ED increased by nearly 40%.3 Multiple risk factors for infection exist in the elderly including immunosuppression, malnutrition, hospitalisation and medical procedures. Additionally, the population is increasingly comorbid and as people age they are more likely to live with long-term conditions (LTC) or frailty.4 14% of those aged under 40 report having a LTC, increasing to 58% in the over 60s with 25% having two or more LTCs.5 These conditions influence outcomes in sepsis and sepsis also worsens their chronic disease.6
Clinical protocols aim to facilitate early recognition and treatment, most prominently the Surviving Sepsis Campaign (SSC) 1-hour bundle which describes the ‘Sepsis-6’: administration of antibiotics, fluids and oxygen, and measurement of lactate, urine output and blood cultures in suspected sepsis.7 8 More invasive treatment options include vasopressors, mechanical ventilation and central lines; these will require ICU admission and should prompt discussions regarding escalation of care.7
Earlier disposition decisions, such as admission to ICU, result in lower hospital mortality.9 Despite this, guidelines contain limited recommendations about the effect of functional status and comorbidities on escalation decisions and this may fail to create realistic expectations about outcomes.10 The Surviving Sepsis Guidelines recommend that prognosis and care goals are discussed with patients early, and palliative care initiated if appropriate.7 However, these guidelines focus on ICU care. There is a drive for this decision making earlier to improve the quality of care by involving patients promptly in treatment decisions. The SARS-CoV-2 pandemic has brought these issues to the fore. The use of the Clinical Frailty Score has become standard practice and discussions regarding prognosis, escalation and patient wishes are occurring more frequently in the ED.11
The National Institute for Health and Care Excellence (NICE) guidelines are evidence-based recommendations used in England. NICE sepsis research recommendations highlight the need for epidemiological studies to help plan services.12 This is especially relevant as the population presenting to the ED changes. We aimed to describe the patient characteristics of suspected sepsis in the ED and factors influencing their escalation and treatment decisions.
Methods
We conducted a retrospective observational study of adults presenting to a type 1 ED, the Northern General Hospital (NGH) in Sheffield, with suspected sepsis. It followed the Strengthening the Reporting of Observational Studies in Epidemiology guideline for cohort studies (online supplemental material).
Setting and study population
The NGH is Sheffield’s only adult ED, with approximately 100 000 attendances annually. In 2019, Sheffield had a population of 584 853. Its median age was 35.4 (40.3 for the UK as a whole), there is a noticeably large proportion of 20–24 years old thought to be due to the student population at its two universities, It is an ethnically diverse city with approximately 19% of the population from black or minority ethnic groups.13 14
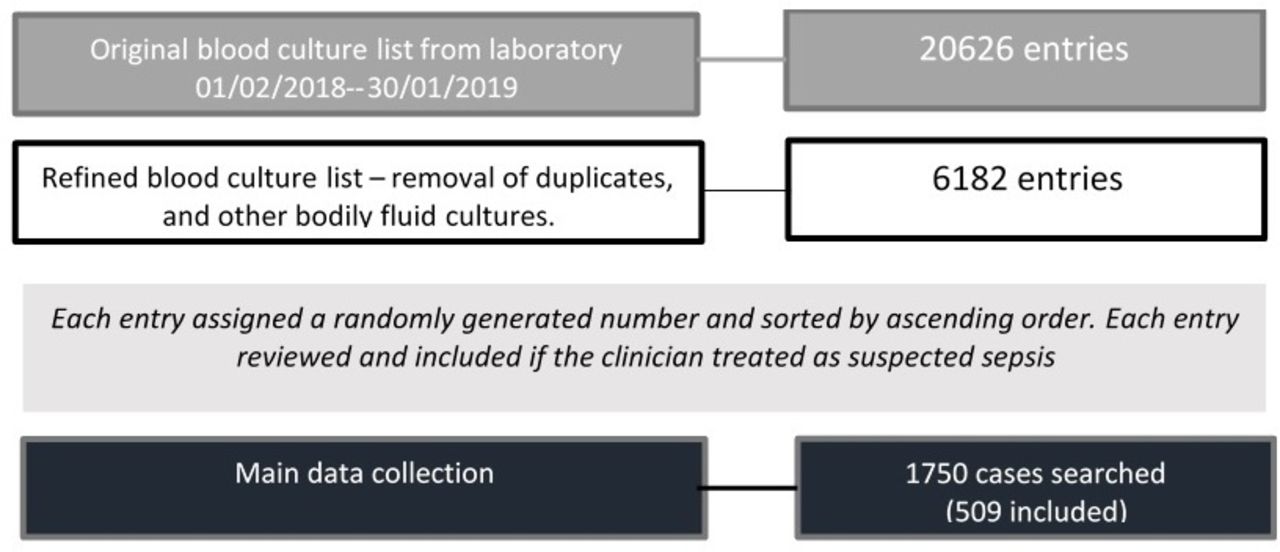
All patients in whom blood cultures were performed in the ED between 01 January 2018 and 31 January 2019 were identified, as a screening method for suspected sepsis. The sample size was estimated (see below) and then cases were randomised using a computer-generated randomisation sequence and each entry was subsequently looked at in an ascending order of randomisation number for inclusion until the prespecified sample size was achieved.
Two clinicians (LS and LW) reviewed charts and determined whether the case was included based on whether the ED clinician suspected sepsis. This specifically required documentation of suspected sepsis, but also included other wording such as ‘Sepsis-6/Red-Flag Sepsis/Sepsis bloods/BUFALO’ (BUFALO is an acronym for the components of Sepsis-6; at NGH this is printed on all charts as an aid memoire with a box for a signature for treatments for audit purposes). Any ambiguity was discussed, and additional documentation reviewed such as ED discharge coding. If a patient had multiple presentations within this period, the first eligible event was included. Direct referrals to specialties were excluded in addition to incomplete electronic records.
Definitions
Cases were retrospectively evaluated according to the Sepsis-3 criteria, defined by evidence of infection and a change in baseline SOFA score ≥2. The baseline score was assumed to be zero where it was not known if there was any pre-existing organ dysfunction. The infection site was determined from culture results, raised inflammatory markers or radiological evidence, where this was not clear cases were discussed to agree whether infection was present. Positive blood cultures, in the absence of a clear source, were diagnosed as bacteraemia. Blood cultures documented as ‘likely contaminant organism’ were not included. The latter are flagged by the microbiologist by the type of bacteria (skin flora suggesting contaminant at venepuncture, and the time it takes for a BC to flag as positive—small numbers of contaminating bacteria take longer to grow compared with a real bacteraemia). All investigation results were reviewed before a decision on excluding these as usually this is a clinical decision made by assessing the patient and the likelihood that the result does represent a contaminant; often a repeat blood culture is sent.
The SOFA score was modified to substitute PaO2/FiO2 (partial pressure of arterial oxygen/fraction of inspired oxygen) with SpO2/ FiO2, (oxygen saturations/fraction of inspired oxygen) as previously validated,15 but was otherwise unchanged.1
Sample size
This is a descriptive study; therefore, the aim was for a study size sufficient to estimate a typical proportion. A sample size of 500 was chosen, which allowed us to estimate a typical proportion of around 20% with a reasonable degree of precision (ie, a 95% CI 16.6% to 23.8%).
Outcome measures
The outcome measures were descriptive: describing the characteristics, management and outcomes of adults attending the ED with suspected sepsis. Specifically, the prevalence of comorbidities, functional impairment and ceilings of care within this group.
Data extraction
Electronic ED records, discharge summaries, laboratory and radiology reporting systems were reviewed to obtain data including the patient demographics, medical and social history, management (including escalation plan) and outcomes. This was recorded using a standardised extraction form, with explicit definitions for study variables, by two data collectors (LS and LW).
The coroner’s office was contacted for those patients who had been referred to them. The General Register Office was contacted for patients that had died in the community to obtain the date and cause of death.
qSOFA and National Early Warning Score (NEWS) were calculated from the initial ED observations.1 16 For missing values, the next recorded value was taken, and it was documented that the initial value was missing. To convert the Glasgow Coma Scale (GCS) to the Alert, Voice, Pain, Unresponsive (AVPU) scale for NEWS, GCS ≤13 was accepted as being equivalent to VPU.17
SOFA scores were calculated from the initial observations and blood results; missing values were assumed to score zero. Charlson Comorbidity Index (CCI) was calculated based on the comorbidities recorded on admission.18
Statistical analysis
Descriptive statistics are used with 95% CI for key proportions. Continuous data, if normally distributed, are presented as mean±SD and if skewed, as median (IQR). Categorical data are presented as proportions (percentages).
Parametric assumptions for statistical tests were checked. All statistical data analyses were performed using SPSS V.25.0 (IBM).
Patient and public involvement
The design and methodology of this study was presented to the Sheffield Emergency Care Forum who advised on the study concept.19
Results
A total of 1750 patients were randomly selected from the blood culture list and reviewed, resulting in 509 patients treated as suspected sepsis (figure 1). Extrapolating this to the total number of BCs taken in the year suggests an estimated incidence of suspected sepsis per year of 1798 cases, which is similar to other studies.20 21

Summary of the identification of the main study participants.
Patient characteristics
Table 1 describes characteristics of the study population. The median age was 74 years (IQR 58–82). 81.5% of the cohort arrived by ambulance and 44.8% were seen in the resuscitation room. Almost 50% met the Sepsis-3 criteria (49.3% (45.0%–53.6%)). The most common suspected sources were chest or urinary and there did not appear to be a seasonal pattern in the date of presentations (online supplemental material).
Baseline characteristics
Regarding the calculated qSOFA, 25.9% (22.1%–29.7%) would have met the qSOFA criteria to suggest investigation for sepsis. The median NEWS score was 6 (IQR 3–8).
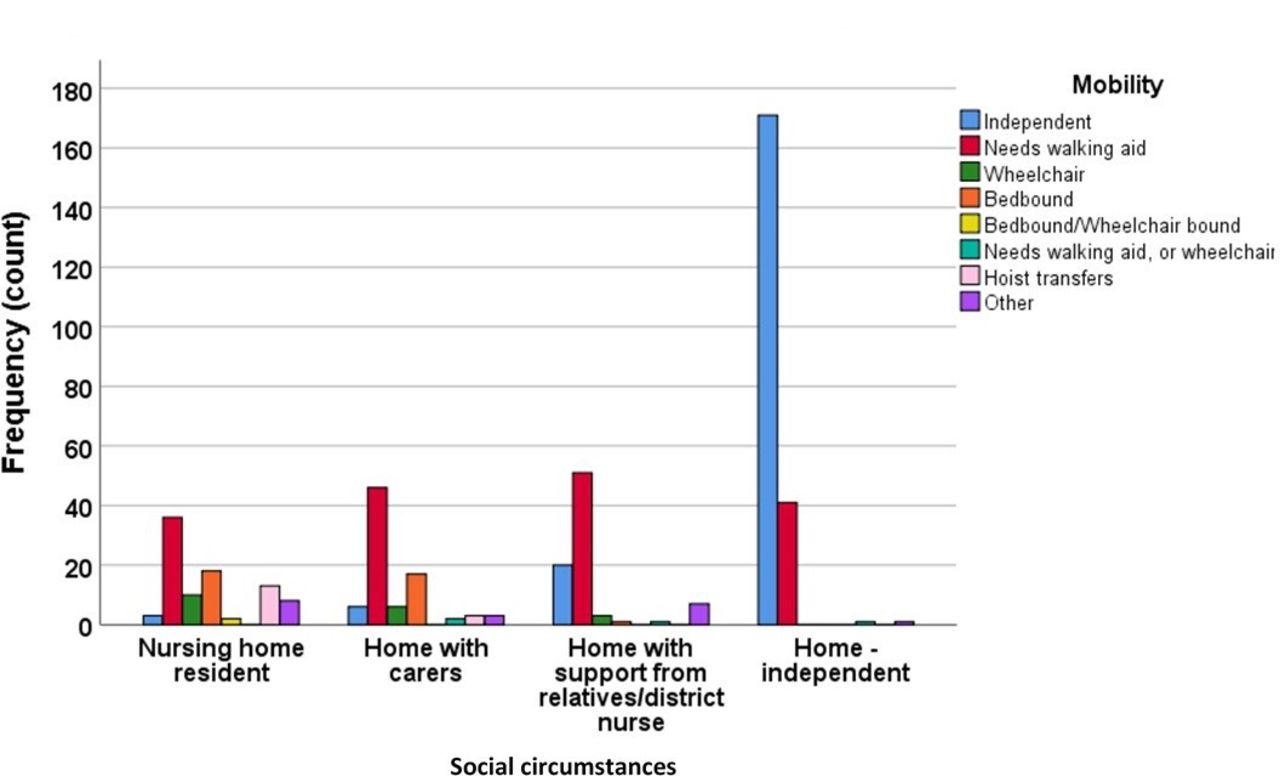
Table 2 shows patient social circumstances: 42.6% (38.3%–46.9%) were living at home independently; 17.3% (14.0%–20.6%) with a care package and 19.3% (15.9%–22.7%) in a care home. Less than 50% were mobile independently (41.5% (37.2%–45.8%). Figure 2 graphically demonstrates that care home residents or those with a package of care are less independently mobile than those at home without a care package.

{kind=link}
{kind=link}
Distribution of mobility of the study population by social circumstance.
Social circumstances and mobility
The comorbidity burden was high with 10.8% of the study population having no comorbidities (table 3). The most common comorbidity was pulmonary disease (30.6%, 26.6%–34.6%), the median CCI was 5 (IQR 2–6).
Comorbidities, CCI and medication
Table 4 shows that 22% (18.4%–25.6%) of the study population had an existing do not attempt resuscitation (DNAR) order. 39 (7.7%) patients had a discussion regarding resuscitation in the ED (11 of which were by the medical or ICU team).
Do not attempt resuscitate decisions and escalation
16.5% (13.3%–19.7%) had an escalation plan explicitly documented. 6.5% (4.4%–8.6%) were referred to ICU; patients were seen by the ICU team and decided appropriate for level 3 care (ICU care), 13 patients for level 2 care (high-dependency unit (HDU)). For both groups, the median NEWS was 11 (IQR 10–11); higher than the median NEWS of 6 (IQR 3–8) for the study population.
Regarding treatment, 98.8% (97.9%–99.8%) of the study population received antibiotics, and 93.3% (91.1%–95.5%) had fluids (online supplemental material).
Just over 13% (13.2%) of patients died in-hospital with a median time from admission to death of 5 days (IQR 2–16).
Sepsis-3-defined sepsis
Online supplemental table 5 includes a summary table for the whole cohort and those that meet the Sepsis-3 definitions of sepsis. Online supplemental tables 6–8) describes the characteristics of the Sepsis-3-defined sepsis cohort in more detail. 49.3% met the Sepsis-3 definitions of sepsis, these patients were older with a median age of 77 years (IQR 65.0–85.0), 90.4% arrived by ambulance a greater proportion were treated in the resuscitation room (59.4%). This is reflected in the physiology with the NEWS scores being higher for this group 7 (IQR 5–10).
Generally, these patients were less independent than the whole cohort; 25.1% were care home residents, with 34.3% living independently at home. Median CCI was 5 (IQR 3–7), and more patients were likely to already have a DNAR in place on presentation (27.5%).
This group had a larger proportion referred to ICU (10.4%), and higher in-hospital mortality (19.5%, median 5 days, IQR 13). Of the latter, 19 out of 49 patients had an explicit escalation plan (10 patients for ward-level care, 1 for a palliative care bed and 8 for full escalation).
Discussion
Adults attending the ED with suspected sepsis are elderly (median age 74 years) and dependent, with fewer than half living at home independently or walking independently, and almost 20% from a nursing home. Only 10.8% of the population have no comorbidities and over 20% of the study population have an existing DNAR order. Despite this, only 16.5% have an escalation plan explicitly documented in the ED (ie, the level of care escalation for the patient—ward or higher level such as HDU or ICU). Those meeting the Sepsis-3 definition (49.3%) were particularly elderly (median age 77 years), and likely to be dependent, have comorbidities and an existing DNAR order.
A quarter of patients that met the Sepsis-3 criteria were from a care home. Other authors report similar results.22 Similarly, ICU admission (4.4%) and in-hospital mortality (13.2%) were both within the range reported by other studies.23–25
The reporting of comorbidities in the literature is variable. For example, studies looking at sepsis outcomes in specific populations are likely to have a different distribution of comorbidities, similarly trials are likely to report fewer comorbidities due to exclusion criteria sometimes encompassing advanced directives or clinician decision regarding suitability for aggressive care.
One of the drivers for doing this study was to define the prevalence of comorbidities, baseline functional state and consideration of escalation decisions in patients managed as sepsis in the ED. There is little current literature that combines these factors together or discusses escalation decisions. Some studies report proportions of patients with a DNAR order in place, and these are similar to these study results, although, of note, the additional information of whether these discussions were had in the ED are not reported in these studies.26 27
The majority of those that died in-hospital did not have an explicit escalation plan documented. This suggests that either implicit ceiling of care decisions are being made and not documented or that recognition of those patients that may require ICU is poor.
Studies have demonstrated that acute infections worsen chronic diseases which can lead to poor longer term outcomes,6 therefore knowledge of the prevalence of chronic diseases in an ED population will help improve our understanding of management of sepsis in an ageing population. The SSC advise ‘setting goals of care’ in the acute setting and having these escalation discussions with patients early.7 This study suggests that given the characteristics of the population described the guidelines should reflect and create realistic expectations for both patients and clinicians, not simply a 1-hour target.
Feedback from the patient and public involvement group welcomed these discussions in the ED. Some members related to personal experience of being unaware of a relative’s poor prognosis and despite the difficulties surrounding these conversations in a busy environment, overall, they welcomed having these candid discussions.
Physiological scoring may be helpful for predicting the need for intervention, but our findings suggest that comorbidities may have an important role in determining prognosis. Treatment and escalation decisions therefore need to take both physiological scoring and comorbidities into account.
This research area has not been well explored therefore the main strength of this descriptive primary research study is to address this gap and address one of the NICE research recommendations—an epidemiological study on presentation and management of sepsis in England. Many of the previous studies have either used selected cohorts or routine data sources so may have underestimated the rate of comorbidities with little reporting of functional status. In this study, we have looked at the proportion of suspected sepsis patients that have risks of poor outcomes and the need for discussions of care and more individualised treatment goals. We hope this will develop the guidelines that are currently focused on rapid intensive treatment, to include decision making in a population described in this study.
Limitations
All scores were calculated retrospectively; if applied prospectively, this may have altered decision making, for example, if scores reached a threshold for action such as senior involvement. Furthermore, both the calculation of the scores and selection of the cases were performed by the researchers who knew both the outcomes and hypothesis of the study; this could lend itself to observer bias.
Second, using blood cultures to identify the cohort may not identify all relevant cases due to variable compliance with blood cultures being taken (29% in a multicentre study),28 either due to an omission or intentional decision that the investigation was not clinically appropriate for example, during end-of-life care.
Finally, with regard to the SOFA score, the adaptation to the respiratory component due to unavailable arterial oxygen results could have resulted in differing results. Similarly, the cardiovascular component did not consider other medication given for treating hypotension.
Conclusions
This study demonstrates that adults with suspected sepsis are elderly, have substantial functional limitations, comorbidities and treatment directives that should be considered in guidelines, especially recommendations for escalation of care. There must be a balance to create realistic treatment expectations and involvement of patients regarding these.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
The project was registered with the Clinical Research and Innovation Offic and was determined to not require NHS Research Ethics Committee review, as it involves analysis of data collected in routine clinical care. An independent scientific review, local costs and approvals were submitted. The project was also registered and approved by the School of Health and Related Research (ScHARR) Research Ethics Committee. The University of Sheffield is the Research Governance Sponsor.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Ed Benjamin Graham Barnard
Contributors LS and SG were responsible for the conception and design of the study, data extraction (LS and LW), and analysis and interpretation (LS and SG). LS drafted the article and all other authors have revised it critically.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Commentary